


Along with retinal detachments, full thickness macular holes are the most devastating complications of the ubiquitous posterior vitreous detachment. A full thickness macular hole is a disruption of all retinal layers from the internal limiting membrane to, but not including, the retinal pigment epithelium. When we think of full thickness macular holes, most clinicians immediately think of idiopathic full thickness macular holes: a full thickness macular hole that spontaneously arises from pathological tangential and antero-posterior vitreoretinal forces. But full thickness macular holes can also develop secondary to trauma, chronic macular edema, or vitreoretinal surgery. The majority of macular holes are of the idiopathic type and for the purposes of this article (and our word count!), I will use the term macular hole as a shorthand of idiopathic full thickness macular hole.
Welcome to Diagnostics & Imaging Monthly, a new column from Daniel Epshtein, OD, FAAO! This column will cover diagnostics and imaging of the anterior and posterior segment and will share both basic and advanced educational tips to help optometrists and ophthalmologists.
While you're waiting for the next column, check out these articles:
- OCT Diagnostics in 2021: When 45 Degrees Isn’t Enough
- The Ultimate Guide to SMILE Refractive Surgery for Optometrists
- Pathogenesis, Classification, and Treatment of Diabetic Retinopathy
- A Complete List of Ocular Diseases with Optical Coherence Tomography (OCT)
- How to Use Ultra-widefield HD 2.0 True Color Imaging in Full-Scope Optometry
- A Complete Guide to the Clarus 500 Ultra-widefield Retinal Camera
Clinically, macular holes often appear as reddish round-ovoid foveal defects with slightly rolled edges. Depending on the morphology and chronicity of the macular hole, retinal pigment epithelial changes within the hole, and a grayish edema cuff may be found around the hole. Patients will often complain of a central scotoma and have significantly reduced vision in the 20/80 to 20/400 range. Though the Gass classification of macular holes was based on clinical findings, the modern classification of macular holes is OCT-based and relies on the International Vitreomacular Traction Study criteria.1,2 I, for one, was ecstatic when the new OCT-based guidelines were adopted because the diagnosis of vitreomacular interface diseases was simplified (and because I could never remember the entire Gass classification system).

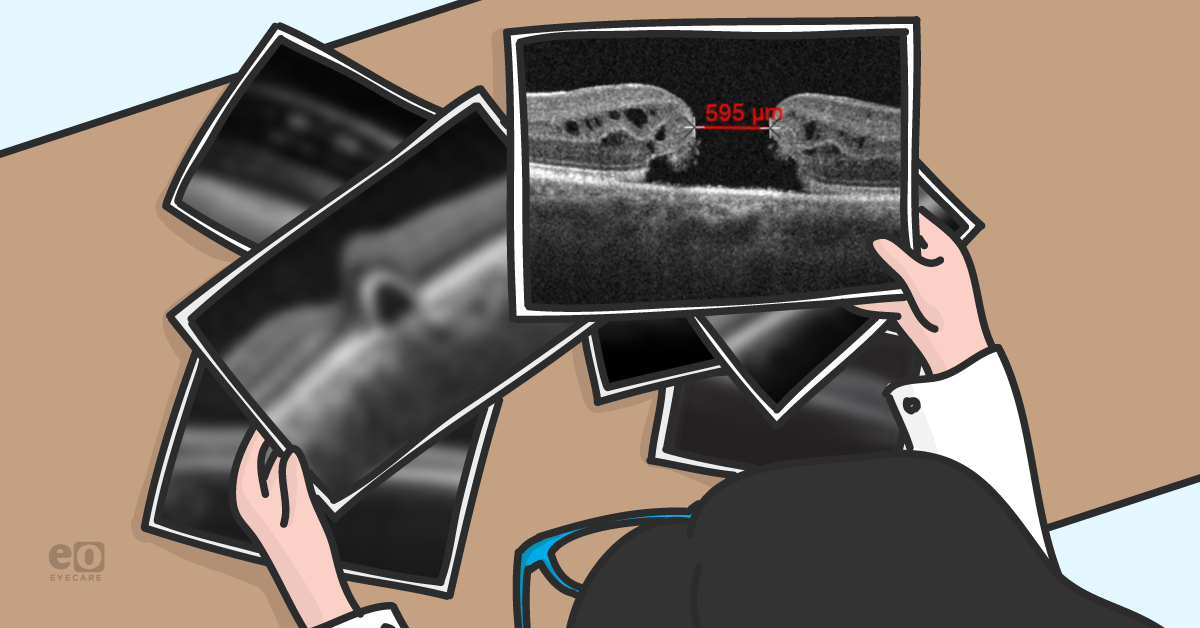
Figure 1: Full thickness macular hole with aperture size denoted
Macular holes can be subdivided into small (≤250 μm), medium (251 μm-399 μm), and large (>400 μm) depending on their minimum aperture width size.2 Macular holes are classified by size because each category has its own rate of success with pneumatic vitreolysis, pharmacological vitreolysis, or pars plana vitrectomy. In addition to size, the chronicity of the macular hole plays an important role in visual recovery after treatment. Earlier intervention of macular holes is associated with improved postoperative acuity and higher closure rates. Pars plana vitrectomy is the gold standard intervention for macular holes with closure rates ~90% in small and medium macular holes, whereas large and chronic macular holes have lower and more variable rates of closure.3
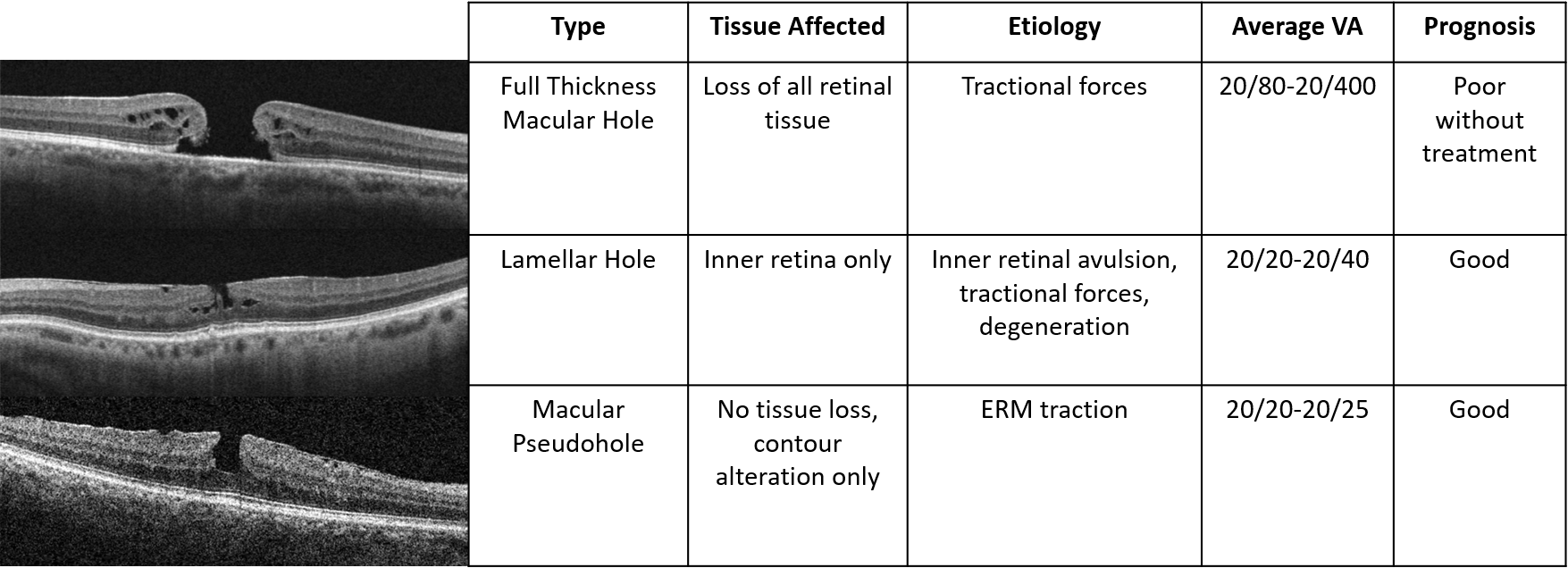
OCT is essential to the management of any vitreomacular interface disease due to its excellent ability to visualize the various retinal layers and vitreomacular interface. When diagnosing full thickness macular holes, it is imperative to rule out lamellar macular holes and macular pseudoholes, as they all have a very different management approach.
Clinically, it may be difficult to distinguish between full thickness macular holes, lamellar macular holes, and macular pseudoholes because they will all appear as reddish round-ovoid foveal defects. Symptoms and visual acuity will help differentiate these entities, but OCT will provide the proper diagnosis in 100% of cases. Even if a full thickness macular hole has already been diagnosed, it is still important to run an OCT to rule out disease in the other eye, because fellow eyes have an up to 15% risk of developing a macular hole within five years.3
| Gass Classification | International VMT Study Classification System | Treatment |
|---|---|---|
| Stage 0 | Vitreomacular Adhesion | Monitor |
| Stage 1: Impending Macular Hole | Vitreomacular Traction (VMT) | Monitor* |
| Stage 2: Small Macular Hole | Small or Medium Macular Hole with VMT | Vitreolysis# or Vitrectomy |
| Stage 3: Large Hole | Medium or Large Macular Hole with VMT | Vitreolysis^ or Vitrectomy |
| Stage 4: Macular Hole with PVD | Small, Medium, or Large Macular Hole without VMT | Vitrectomy |
* Consider earlier intervention in patients with full thickness macular hole in fellow eye or monocular patients
# Either pneumatic or pharmacological vitreolysis
^ Can consider pharmacological vitreolysis in macular holes ≤400 μm
Lamellar macular holes are inner retinal defects with an intact photoreceptor layer.2 The inner retinal defect consists of retinal schisis and/or tissue loss. The pathogenesis of lamellar macular holes is still unclear but can be thought of as incomplete full thickness macular holes. Due to the frequent presence of a pseudo-operculum floating above the lamellar macular hole, some researchers theorize that a possible cause of lamellar macular holes is the avulsion of the superficial retina secondary to anteroposterior traction.
Lamellar macular holes can also be caused by tractional forces from surrounding epiretinal membranes or degeneration secondary to another retinal condition. The epiretinal membrane associated lamellar macular hole is more amenable to intervention since there is a progressive insult that can be altered, as opposed to the superficial avulsion type where the tissue is lost and anatomy cannot be normalized.
Vision is usually minimally affected in these patients with acuities in the 20/20-20/40 range with or without the presence of metamorphopsia. Unlike full thickness macular holes, there is no accepted intervention protocols for lamellar macular holes. Monitoring is frequently recommended due to the relatively good visual acuity and often stable nature of these lesions.
Personally, all the lamellar macular holes that I have managed have been fairly stable and most patients have been relatively asymptomatic. The majority of these cases were incidental and patients only realized the vision loss after I compared their vision in the affected eye to the fellow eye.
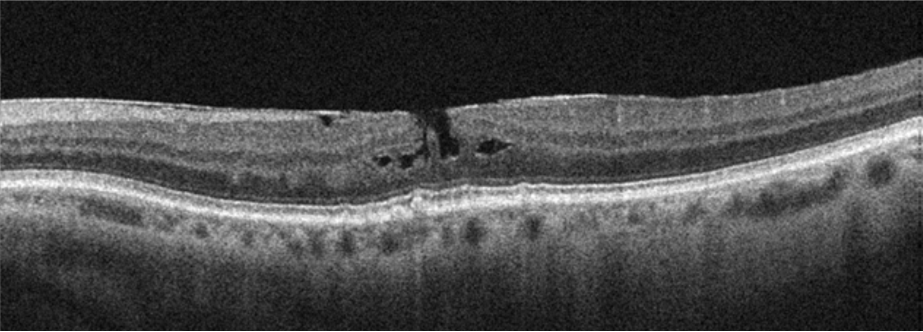
Figure 2: Lamellar hole with mild schisis
Macular pseudoholes are foveal defects caused by epiretinal membrane tractional forces.2 The membrane alters the foveal contour, often leading to a deeper rectangular foveal pit, without retinal tissue loss. Funduscopically, these lesions will look like round-ovoid reddish defects with a surrounding epiretinal membrane.
Vision will often be in the 20/20-20/25 range with or without the presence of metamorphopsia. These lesions are almost always more clinically impressive than they are visually significant. No intervention is necessary unless the epiretinal membrane progresses and vision deteriorates; pars plana vitrectomy and epiretinal membrane peeling can be considered in these cases.

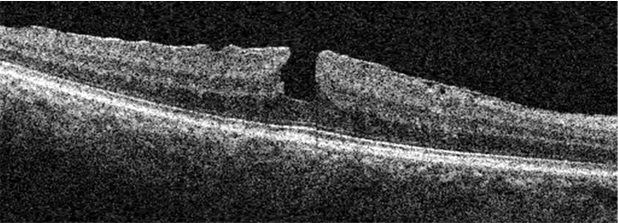
Figure 3: Macular pseudohole. Note the rectangular and veticalized foveal contour
Vitreomacular interface diseases (including vitreomacular traction and vitreomacular adhesion) are relatively common and can have devastating effects on vision in the advanced stages. Due to the significant ambiguity when relying on clinical features alone, modern nomenclature and classification systems are based on OCT findings. The OCT patterns in vitreomacular interface disease are almost intuitive and are a great way to dive into OCT analysis for those new to the technology. Hopefully, this has illuminated the sometimes-equivocal subject of vitreomacular interface disease and provided another stepping-stone to OCT mastery.

We have a direct partnership with ZEISS!
