





When it comes to cataract surgery, you must respect the corneal endothelium! This is especially true in eyes with Fuch’s Endothelial Corneal Dystrophy (FECD), a disease of the corneal endothelium that commonly co-exists with patients undergoing cataract evaluation.
Here, we present the pathology of FECD and review how best to approach cataract surgery in eyes with FECD for the best possible vision outcomes.
Pathology
Commonly, the endothelium is involved with the active transport of ions and regulation of water content in the corneal stroma. Through this regulation, endothelial cells help maintain the deturgescence of the stroma.1 Over time, the number of endothelial cells decreases, and the endothelium's mitotic activity, in general, is limited. In FECD, the rate of endothelial loss is accelerated.
Additionally, endothelial cells become dysfunctional and cause swelling, exhibiting polymegathism and pleomorphism (varying in size and shape). Deposition of collagen and extracellular matrix occur in the Descemet’s membrane and cause thickening.
There are a total of four stages of FECD. There is a loss of endothelial cells and Descemet's membrane swellings early. These excrescences create an appearance called “guttata” on slit-lamp examination.
Figure 1, demonstrates guttae visualized with retroillumination on slit lamp exam.

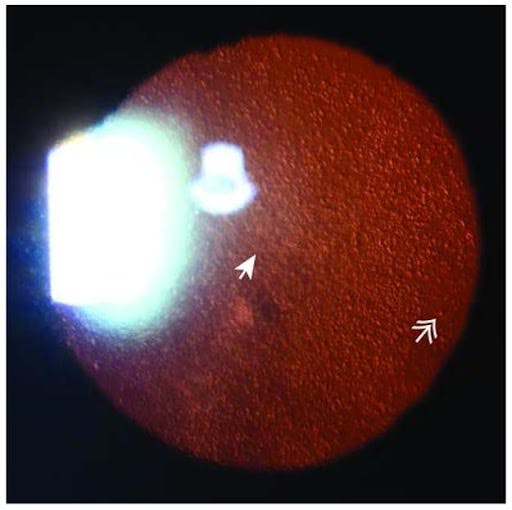
Corneal guttata first develop centrally and then spread peripherally. The guttae can enlarge during the later stages of the disease. In the second stage, the integrity of the endothelium becomes compromised and causes stromal edema. Following this, the third stage may exhibit increased stromal edema and thickening of the Descemet membrane. The edema can cause epithelial bullae and bullous keratopathy. In end-stage disease (Stage 4), subepithelial fibrosis, scarring, and peripheral superficial vascularization are evident.2
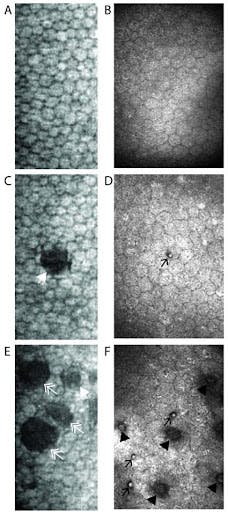
Figures 2 illustrates specular microscopy (first column) and confocal microscopy (second column) of guttae. Images A and B represent a healthy individual. Image C demonstrates Stage 3 guttae. Image D demonstrates Stage 1 guttae. Image E shows Stage 2 (solid arrowhead) and 3 (double arrowhead) guttae. Image F demonstrates Stage 1 (arrow) and Stage 2 guttae (solid arrowhead).

Although the cause of FECD is unknown, some families demonstrate an autosomal dominant inheritance pattern based on the COL8A2 gene.
Symptoms
Corneal edema in FECD leads to decreased visual acuity, contrast sensitivity, and glare. Symptoms also worsen during awakening in the morning due to reduced surface evaporation during sleep. Ocular pain can occur due to edema or rupture of bullae. The prevalence of these symptoms tends to be more common in greater than 50 years of age.
Diagnosis
Evaluation methods for FECD include specular microscopy and corneal pachymetry. Specular microscopy can be used in the initial evaluation of FECD and it helps monitor endothelial cell loss. However, there are limitations to this method when there are diffuse confluent guttae as specular microscopy relies on a smooth and transparent cornea.3-4 Observing the guttae will appear as round or dark oval areas and present as a small central point of reflection.5
The parameters evaluated include density, coefficient of variation, and percentage of hexagonal cell.3
On the other hand, corneal pachymetry measures corneal thickness and can give a relative measure of corneal endothelial function. Pachymetry is especially useful in monitoring progression over time and providing information about the safety of cataracts or other intraocular surgery in FECD patients as surgery can lead to further endothelial cell loss and damage.
Treatment
Initial treatment mainly involves targeting the corneal edema and providing pain relief. Sodium chloride drops and ointment can be used to help relieve the edema. In addition, lowering intraocular pressure (IOP) may alleviate symptoms. A bandage contact lens may be used in complicated cases where the bullae have ruptured. For restoration of advanced cases, endothelial keratoplasty (EK) is preferred over penetrating keratoplasty, focusing on replacing the pathologic endothelial cells.3
The procedures under the umbrella of endothelial keratoplasty (EK) include Descemet’s Stripping Automated Endothelial Keratoplasty (DSAEK) and Descemet Membrane Endothelial Keratoplasty (DMEK). Complications with surgical management include graft and wound complications, infection, ocular hypertension secondary to steroid use, and cataract formation.7,8
FECD and cataract surgery
As Fuchs tends to present in middle-age and older, cataract comorbidity is common. However, cataract surgery and other intraocular surgeries cause further corneal endothelial cell loss (ECL).10, 11, 12 Whether to proceed with cataract surgery alone or together with an EK procedure (either staged or combined) is dependent on the severity of endothelial dysfunction.2
Predictors of possible corneal decompensation after intraocular surgery include Endothelial cell count <1000/mm2, increased corneal thickness (>640um) with morning blurring, or epithelial edema.3 A staged or combined cataract and EK procedure is recommended in those cases.
It is important to note that some patients with naturally thinner corneas may present with CCT <600 um despite moderate endothelial dysfunction.
A combined procedure, also known as a triple procedure, includes keratoplasty, cataract extraction, and intraocular lens (IOL) implantation. Performing combined procedures helps patients with financial costs, reduces the risk of having multiple procedures, and allows for faster visual rehabilitation.21,22
However, there are also downsides to combined surgery in some eyes, including increased complications and potential endothelial cell loss in those with intraoperative floppy iris syndrome, hyperopia secondary to a short axial length (higher risk of pupillary block), and eyes with known zonular instability. These eyes may benefit from sequential surgeries instead. Studies have shown similar outcomes between staged and combined cataract and EK procedures.
For a combined surgery to succeed, it is essential to use a highly cohesive viscoelastic, which allows for complete removal from the anterior chamber before tissue insertion. It is also necessary to create a smaller capsulorhexis, to allow for more stability of the IOL during the tissue transplant.21 Many of the findings in FECD cause opaque appearances of the cornea, creating a dim view for the surgeon when performing intraocular surgery. In these cases, debridement of the corneal epithelium or application of glycerin on the corneal surface may help to improve the surgeon’s intraoperative view.
Postoperative complications involving ECL have shown no significant difference between combined procedures involving DSAEK versus DMEK.21,22,23 It has been observed that cystoid macular edema (CME) is less common following DSAEK versus that seen with DSAEK combined surgery.24 Moreover, there is evidence that ECL may be higher in combined DMEK and cataract surgery cases than sequential procedures.9
Cataract surgery alone can be considered (and even recommended) in patients exhibiting a CCT less than 640 µm and an ECD count greater than 1000 cells/mm,2 as there is a high likelihood of good outcomes. Ophthalmic viscosurgical devices (OVDs) have demonstrated effectiveness in protecting the corneal endothelium perioperatively and have even shown a near return to preoperative corneal thickness at 6 months.27
One study found a 6.4% ECD loss using a soft-shell technique, which employs a dispersive OVD, versus a 16.3% ECD loss with cohesive viscoelastic alone.26 The benefits of using femtosecond laser-assisted cataract surgery (FLACS) over conventional phacoemulsification for these patients remain controversial. FLACS may reduce phacoemulsification time and energy resulting in decreased perioperative ECL, but some studies have shown no significant differences in outcomes beyond 12 months postoperatively.28
FECD and IOL selection
A hyperopic shift should be anticipated in approaching IOL calculations for FECD patients, especially in staged or combined triple procedures. This is due to an induced change in the refractive index of the cornea secondary to edematous changes causing flattening of the posterior corneal curvature and the DSAEK or DMEK lenticule acting as a negative powered lens.29, 13, 14, 15 Evaluating the posterior cornea with Scheimpflug tomography and using a modified corneal power for IOL calculations can help to improve refractive predictability.30
The most commonly used method aims for a more myopic refractive target (-0.50 D for DMEK and up to -1.25 for DSAEK). This is due to the expectation that there will be a natural hyperopic shift in FECD patients with or without EK surgery.16, 17, 18, 21
Lens selection in this population is another important topic of discussion. Studies have shown an increased risk of IOL calcification during DMEK and DSAEK. While the etiology is unknown, there seems to be an increased risk of using hydrophilic lenses or air or gas in the anterior chamber, which also increases IOP.31 Therefore, hydrophobic lenses are recommended if a patient undergoes an EK procedure.
Multifocal IOLs should generally be avoided in patients with FECD as they can further degrade vision quality and contrast. However, one study showed good visual and refractive outcomes using presbyopia-correcting IOLs in FECD following a staged DMEK after corneal edema had cleared.32 The preferred IOL for FECD patients is an aspheric, hydrophobic, monofocal lens.
Billing and coding
The ICD-10 code for FECD is H18.51 - Endothelial corneal dystrophy. The CPT code for endothelial keratoplasty is 65756 and for routine cataract surgery is 66985.25
Conclusions
When encountering a cataract patient with FECD, it is essential to carefully assess endothelial cell function to decide whether to proceed with cataract surgery alone or together with an EK procedure (staged or combined). Intraoperatively, several precautions can be taken to minimize complications and endothelial cell loss to ensure a better outcome for patients with FECD.
References
- 2019-2020 Basic and Clinical Science Course, Section 02: Fundamentals and Principles of Ophthalmology. San Francisco, CA: American Academy of Ophthalmology; 2019.
- Moshirfar M, Somani AN, Vaidyanathan U, et al. Fuchs Endothelial Dystrophy. [Updated 2021 Nov 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-.
- 2019-2020 Basic and Clinical Science Course, Section 08: External Disease and Cornea. San Francisco, CA: American Academy of Ophthalmology; 2019.
- Hara M, Morishige N, Chikama T, Nishida T. Comparison of confocal biomicroscopy and noncontact specular microscopy for evaluation of the corneal endothelium. Cornea. 2003 Aug;22(6):512-5.
- Adamis AP, Filatov V, Tripathi BJ, Tripathi RC. Fuchs' endothelial dystrophy of the cornea. Surv Ophthalmol. 1993 Sep-Oct;38(2):149-68.
- Repp DJ, Hodge DO, Baratz KH, McLaren JW, Patel SV. Fuchs' endothelial corneal dystrophy: subjective grading versus objective grading based on the central-to-peripheral thickness ratio. Ophthalmology. 2013 Apr;120(4):687-94.
- Feizi S. Corneal endothelial cell dysfunction: etiologies and management. Ther Adv Ophthalmol. 2018 Jan-Dec;10:2515841418815802.
- Nanda GG, Alone DP. REVIEW: Current understanding of the pathogenesis of Fuchs' endothelial corneal dystrophy. Mol Vis. 2019;25:295-310.
- Shahnazaryan D, Hajjar Sese A, Hollick EJ. Endothelial Cell Loss After Descemet's Membrane Endothelial Keratoplasty for Fuchs' Endothelial Dystrophy: DMEK Compared to Triple DMEK. Am J Ophthalmol. 2020;218:1-6. doi:10.1016/j.ajo.2020.05.003
- Baradaran-Rafii , Rahmati-Kamel M, Eslani M, Kiavash V, Karimian F: Effect of hydrodynamic parameters on corneal endothelial cell loss after phacoemulsification. J Cataract Refract Surg 2009; 35: pp. 732−7.
- Heo WJ, Lee JY, Kim HK: Comparison of clinical outcomes between high and low fluid-dynamic parameters during phacoemulsification. J Korean Ophthalmol Soc 2015; 56: pp. 1860−6.
- Choi JY, Han YK. Long-term (≥10 years) results of corneal endothelial cell loss after cataract surgery. Can J Ophthalmol. 2019;54(4):438-444. doi:10.1016/j.jcjo.2018.08.005
- Fritz M, Grewing V, Böhringer D, et al. Avoiding hyperopic surprises after descemet membrane endothelial keratoplasty in Fuchs dystrophy eyes by assessing corneal shape. Am J Ophthalmol. 2019;197:1–6.
- Ham L, Dapena I, Moutsouris K, et al. Refractive change and stability after Descemet membrane endothelial keratoplasty. Effect of corneal dehydration-induced hyperopic shift on intraocular lens power calculation. J Cataract Refract Surg. 2011;37(8):1455–1464. doi:10.1016/j.jcrs.2011.02.033
- Wacker K, Cavalcante LCB, Baratz KH, Patel SV. Hyperopic trend after cataract surgery in eyes with fuchs’ endothelial corneal dystrophy. Ophthalmology. 2018;125(8):1302–1304. doi:10.1016/j.ophtha.2018.03.060
- Yong WWD, Chai HC, Shen L, Manotosh R, Anna Tan WT. Comparing outcomes of phacoemulsification with femtosecond laser-assisted cataract surgery in patients with fuchs endothelial dystrophy. Am J Ophthalmol. 2018;196:173–180. doi:10.1016/j.ajo.2018.08.006
- Patel SV, Baratz KH. A commentary on the Yong article: comparing outcomes of phacoemulsification with femtosecond laser-assisted cataract surgery in patients with fuchs endothelial dystrophy. Am J Ophthalmol. 2019;199:258–259. doi:10.1016/j.ajo.2018.10.028
- Hwang RY, Gauthier DJ, Wallace D, Afshari NA. Refractive changes after DSEK: a simplified mathematical model. Invest Ophthalmol Vis Sci. 2011;22(52):1043–1054. doi:10.1167/iovs.10-5839
- Koo EH, Paranjpe V, Feuer WJ, Persad PJ, Donaldson KE. Refractive Outcomes in Fuchs' Endothelial Corneal Dystrophy: Conventional and Femtosecond Laser-Assisted Cataract Surgery. Clin Ophthalmol. 2021;15:3419-3429. Published 2021 Aug 12. doi:10.2147/OPTH.S309869
- Sarnicola, Caterinaa,b; Sarnicola, Enricaa,b; Panico, Edoardoc; Panico, Claudioa; Sarnicola, Vincenzob Cataract surgery in corneal transplantation, Current Opinion in Ophthalmology: January 2020 - Volume 31 - Issue 1 - p 23-27 doi: 10.1097/ICU.0000000000000635
- Terry MA, Shamie N, Chen ES, et al. Endothelial keratoplasty for Fuchs’ dystrophy with cataract: complications and clinical results with the new triple procedure. Ophthalmology 2009; 116:631–639.
- Chaurasia S, Price FW, Gunderson L, Price MO. Descemet's membrane endothelial keratoplasty: clinical results of single versus triple procedures (combined with cataract surgery). Ophthalmology 2014; 121:454–458.
- Jones SM, Fajgenbaum MA, Hollick EJ. Endothelial cell loss and complication rates with combined Descemets stripping endothelial keratoplasty and cataract surgery in a UK centre. Eye 2015; 29:675–680.
- Pedemonte-Sarrias E, Salvador Playà T, Sassot Cladera I, et al. Incidence of cystoid macular edema after Descemet's stripping automated endothelial keratoplasty. Int J Ophthalmol 2017; 10:1081–1087.
- https://www.aao.org/practice-management/news-detail/icd-10-code-fuchs-dystrophy
- Tarnawska D, Wylegała E. Effectiveness of the soft-shell technique in patients with Fuchs’ endothelial dystrophy. J Cataract Refract Surg 2007; 33:1907–1912.
- Arshinoff SA, Norman R. Tri-soft shell technique. J Cataract Refract Surg 2013; 39:1196–1203.
- Zhu DC, Shah P, Feuer WJ, et al. Outcomes of conventional phacoemulsification versus femtosecond laser–assisted cataract surgery in eyes with Fuchsendothelial corneal dystrophy. J Cataract Refract Surg 2018; 44:534–540
- Alnawaiseh M, Zumhagen L, Rosentreter A, Eter N. Intraocular lens power calculation using standard formulas and ray tracing after DMEK in patients with Fuchs endothelial dystrophy. BMC Ophthalmol 2017; 17:152.
- Campbell JA, Ladas JG, Wang K, et al. Refractive accuracy in eyes undergoing combined cataract extraction and Descemet membrane endothelial keratoplasty. Br J Ophthalmol 2021; 0:1–5.
- Darcy K, Apel A, Donaldson M, et al. Calcification of hydrophilic acrylic intraocular lenses following secondary surgical procedures in the anterior and posterior segments. Br J Ophthalmol 2019; 103:1700–1703.
- Price MO, Pinkus D, Price FW. Implantation of presbyopia-correcting intraocular lenses staged after Descemet membrane endothelial keratoplasty in patients with Fuchs dystrophy. Cornea 2020; 39:732–735.
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6629500/
