



Ocular surface disease (OSD) treating clinicians already know the satisfaction of helping patients feel better and see better. You can elevate that satisfaction further by also helping your patients look better. How? By focusing on the DAO.
The DAO is an acronym that borrows from the Taoist principle of The Way. This concept is literally a roadmap to the pathway in a variety of philosophical journeys, but it also applies to the OSD treating clinician and their patients. One look at before and after pictures and the point is crystal clear.
In my practice, I’ve developed an approach to treating dry eye and other ocular surface disorders (OSDs) centered around the DAO: an acronym for addressing the dermatologic, aesthetic, and ophthalmologic aspects of eyecare.
The DAO is a Venn diagram–like approach that borrows from other subspecialties to better understand what’s happening on ocular surfaces as well as the surrounding “neighborhood” which enables our patients to have healthier, more beautiful, and more comfortable eyes.
As illustrated in Figure 1, the intersection of the overlapping circles is the sweet spot I aim for in restoring the ocular surface health of my patients.


Figure 1
The D in DAO: Dermatology
The most common culprit is rosacea. Ocular rosacea is multi-disciplinary, expert consensus panel recognized clinical diagnosis recognized by eyelash changes, lid margin or eyelid telangiectasias, lid thickening, lid edema, meibomian gland dysfunction (MGD), conjunctivitis, keratitis, and even neovascular scarring in severe cases.1 Pediatric rosacea is significantly under-recognized and may present as chronic or recurrent chalazia or styes.
Less common but also important to recognize and treat is seborrheic dermatitis and atopic dermatitis. Driven by a spaghetti and meatballs-looking fungal organism, Malassezia furfur, seborrheic dermatitis can be subtle. Ask and look for dandruff in the scalp, eyebrows, and other facial hair. This fungal organism needs treatment with antifungal agents such as selenium disulfide, 2% ketoconazole prescription shampoo and 2% ketoconazole skin cream.
Intense pulsed light (IPL) also helps treat Seborrheic dermatitis, but IPL must be avoided in hair that you do not want to lose (brows, lashes, male pattern facial hair). The sebum units of the skin are hypersecretory with a dysfunctional sebum and this is a veritable smorgasbord for Demodex mites. IPL, ketoconazole, and targeted skin care (www.Epionce.com) helps decrease sebum production of the skin that may contribute to the mite load.
Given the other favorite location for Demodex (eyelashes and meibomian glands), the need for in-office and at-home debridement will be greatly enhanced by the widely anticipated FDA approval of TP-03 (Tarsus Pharmaceuticals).
The A in DAO: Aesthetics
Even with the growth of aesthetic medicine, many clinicians rarely discuss cosmetics and beauty topics with their patients—a shame, considering that any doctor focused on ocular surface disease understands the dangers and costs of common beauty or hygiene practices. This isn’t just limited to our female patients; everyone wants to look their best, but the everyday products and treatments utilized by all our patients across the gender spectrum can have very real impacts on ocular health.
Educating your patients on the effects their skincare can have on their ocular health is absolutely worth your time! On our intake questionnaire, we ask all of our new dry eye patients what skincare products they use, and it often includes a cleanser like Cetaphil, which strips the meibum protecting the tear film. Make sure your patients know that the eye area requires special hygiene agents, and the cleansers that are good for their skin are not typically good for the eye area.
“Cosmetics are an extremely complex topic”
The retinoids are fraught with confusion. With Vitamin A as the root (carrot pun), multiple derivatives are possible and some are purified, concentrated and added to cosmetics, skin care, and even prescription treatments. However, not all retinoids are bad. In fact, vitamin A and cis-retinoic acid receptors can support the corneal and conjunctival epithelium.
Cosmetics must be preserved to prevent bacterial and fungal contamination. Certain preservatives like formaldehyde-donating preservatives (i.e., sodium hydroxymethylglycinate, quaternium-15, DMDM hydantoin, ureas) and benzalkonium chloride (BAK), are added to prevent fungal or bacterial contamination and are well known for their ocular surface impacting side effects.
Other preservative agents such as parabens and phenoxyethanol, on the other hand, are important and common preservatives that do not demonstrate cell death in human meibomian gland cell culture when at low concentrations.2,3 The challenge is that consumers and clinicians do not know the concentrations in cosmetic products and we do not have in vivo evidence of the direct impact of topical products on the meibomian gland stem cells deep within the glands.
What about cosmetic injections or procedures? When done properly, Botox injections can help with dry eye—as long as they’re not used in the crow’s feet, where they’ve been shown on an age-dependent basis to negatively impact Schirmer scores.4 However, when used strategically, Venkateswaran et al found that Botox can be effective for relieving dry eye associated symptoms of photophobia and pain in migraineurs with neuropathic pain and dry eye.5
Neurotoxins such as Botox can also be used judiciously to effectively address friction syndromes such as superior limbic keratoconjunctivitis and filamentary conjunctivitis.6

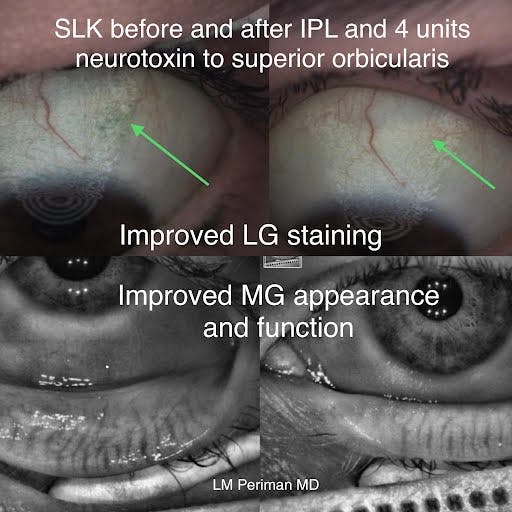
Figure 2: Provided by author.
The O in DAO: Ophthalmology
As you’ve seen, aesthetics and dermatology are not so different when it comes to eyecare. When we consider our patients as whole individuals, we see how much impact their everyday habits have on their ocular health—and we can adjust our treatment plans accordingly.
In 2017, we surveyed dry eye patients to uncover the relationship between cosmetic use and OSD, and found that respondents who did not remove their makeup had higher SPEED scores than those who did so regularly.7 As previously discussed, makeup removers and cleansers can have a huge impact on the ocular surface—but we’re not going to tell our patients not to clean their faces!
Avoiding using facial cleansers near the delicate eyelids can help prevent overstripping of the precious meibum. We use surfactant-free hygiene systems such as in-office ZEST (Zocular) micro-blepharoexfoliation followed by home care with Optase TTO gel (SCOPE) and NuLids (NuSight Medical) in patients with low meibum production.
Other major aspects of ocular health that are frequently overlooked is diet and nutrition. Studies have shown that reduced gut microflora biodiversity is often associated with rosacea, and may explain inflammation across the whole system.8,9 Remember, supplements aren’t enough: we all know to reach for omega fatty acids for our dry eye patients, but it’s worth considering their whole diet as well. I’ll often suggest the Whole 30 nutrition program, which is designed to help its followers identify physical responses to dietary triggers, and to adjust their long-term diets accordingly.
The typical offenders in the rosacea patients are gluten and dairy. Often, other GI symptoms such as gastro-esophageal reflux disease (GERD) also improve enough to where dry eye-exacerbating H2 Blockers can be discontinued. Clean nutrition can help the skin health and appearance of glow.
As rosacea is addressed foundationally (nutrition, avoiding dietary triggers, omega fatty acid supplementation) as well as topically (in-office treatments such as IPL, professional skin care, and often, compounded dermatology triple creams oxymetazoline/ivermectin/niacinamide), the ocular and skin redness improves and this is, of course, an aesthetic benefit of the integrated DAO approach to treatment.
And then, there’s sleep—sleep is critical to overall health. Sleep apnea is a known contributor to ocular surface disease, demonstrating yet another way systemic conditions can affect ocular health. Continuous positive airway pressure (CPAP) machines are the most common way to address the nightly hypoxic episodes experienced by patients with sleep apnea, but CPAP devices are known for drying out the ocular surface.
I typically suggest that CPAP users wear a silicone vaulted eye mask (EyeSeals 4.0 EyeEco.com) or other covering (www.eyesleeptite.com) when they sleep to address this common issue. Interestingly, some of the floppy eyelid syndrome changes (lash ptosis, excess lid laxity, papillary reaction of the upper eyelids) slowly reverse as sleep apnea is treated.10
The DAO in practice
In summary, an integrated ocular surface disease mindset that identifies and treats the Dermatologic, Aesthetic and Ophthalmologic aspects of ocular surface disease elevates your care from just seeing better to the DAO trifecta of feel better, look better and see better.
References
- Tavassoli S, Wong N, Chan E. Ocular manifestations of rosacea: A clinical review. Clin Exp Ophthalmol. 2021 Mar;49(2):104-117. doi: 10.1111/ceo.13900. Epub 2021 Feb 3. PMID: 33403718.
- Wang J, Liu Y, Kam WR, Li Y, Sullivan DA. Toxicity of the cosmetic preservatives parabens, phenoxyethanol and chlorphenesin on human meibomian gland epithelial cells. Exp Eye Res. 2020 Jul;196:108057. doi: 10.1016/j.exer.2020.108057. Epub 2020 May 5. PMID: 32387382.
- Periman LM, Maiti S. Cosmetics and tear film inflammation. Video presented at: Eyes on Dry Eye 2022 virtual conference; March 15, 2022.
- Gunes A, Demirci S, Koyuncuoglu HR, Tok L, Tok O. Corneal and tear film changes after botulinum toxin-a in blepharospasm or hemifacial spasm. Cornea. 2015;34(8):906-910. doi:10.1097/ICO.000000000000048
- Venkateswaran N, Hwang J, Rong AJ, Levitt AE, Diel RJ, Levitt RC, Sarantopoulos KD, Lee WW, Galor A. Periorbital botulinum toxin A improves photophobia and sensations of dryness in patients without migraine: Case series of four patients. Am J Ophthalmol Case Rep. 2020 Jul 4;19:100809. doi: 10.1016/j.ajoc.2020.100809. PMID: 32671286; PMCID: PMC7350146.
- Gumus K, Lee S, Yen MT, Pflugfelder SC. Botulinum toxin injection for the management of refractory filamentary keratitis. Arch Ophthalmol. 2012;130(4):446-50. doi:10.1001/archophthalmol.2011.2713.
- O’Dell LE, Periman LM, Sullivan AG, Halleran CC, Harthan JS, Hom MM. An evaluation of cosmetic wear habits correlated to ocular surface disease symptoms. Ophth Vis Sci. 2017;58:ARVO
- Daou H, Paradiso M, Hennessy K, Seminario-Vidal L. Rosacea and the Microbiome: A Systematic Review. Dermatol Ther (Heidelb). 2021 Feb;11(1):1-12. doi: 10.1007/s13555-020-00460-1. Epub 2020 Nov 10. PMID: 33170492; PMCID: PMC7859152.
- Morss-Walton P, McGee JS. Rosacea, not just skin deep: Understanding thesystemic disease burden. Clin Dermatol. 2021 Jul-Aug;39(4):695-700. doi: 10.1016/j.clindermatol.2020.08.006. Epub 2020 Aug 11. PMID: 34809774.
- Vieira MJ, Silva MJ, Lopes N, Moreira C, Carvalheira F, Sousa JP. Prospective Evaluation of Floppy Eyelid Syndrome at Baseline and after CPAP Therapy. Curr Eye Res. 2021 Jan;46(1):31-34. doi: 10.1080/02713683.2020.1776332. Epub 2020 Jun 16. PMID: 32482105.
Dr. Periman is founder and director of Dry Eye Services and Clinical Research at Periman Eye Institute in Seattle. For more, visit: www.dryeyemaster.com IG, Twitter, TikTok: DryEyeMaster
Disclosures: Aerie, Alcon, Aldeyra, Allergan, Bausch + Lomb, Bruder, Eyedetec Medical Inc., EyeEco, Horizon, Kala Pharmaceuticals, Lumenis, Novartis, NuSight Medical, Olympic Ophthalmics, Quidel, Santen Pharmaceuticals, Science Based Health, Scope Eyecare, Sun Ophthalmics, Tarsus, TearLab, Visant Medical, Zocular.

