




WHAT YOU'LL LEARN
How diagnostic imaging can efficiently assist eyecare providers in staging diabetic retinopathy for better management.
How telemedicine screenings can increase accessibility to care and make detection of diabetic retinopathy earlier.
Introduction
Diabetic retinopathy is the number one cause of blindness in people 20-74 years of age, and healthcare professionals can decrease the risk of blindness in about two-thirds of these patients if diagnosed and treated in the early stages. The National Committee for Quality Assurance states that only 40% of the diabetic population is screened for diabetic retinopathy using traditional screening methods.
In addition to the inadequate screening methods for diabetic retinopathy, the ratio of eyecare professionals to diabetic patients is shockingly disproportionate. According to the American Optometric Association, as of 2015 there were an estimated 30 million adults with diabetes within the U.S. The incidence of diabetes in the U.S. is increasing at roughly 1.4 million cases per year, with only an average of 2000 eyecare professionals emerging each year. These rates suggest that we will need at least one eyecare provider for every 700 diabetic patients to screen and evaluate for vision-threatening diabetic retinopathy!
Screening methods aren’t reaching enough of the diabetic population, and now there aren’t enough eyecare professionals available to fill in the gaps. How can we meet these future demands and properly manage such a large volume of diabetic patients? This course will emphasize how diagnostic imaging can efficiently assist eyecare providers in staging diabetic retinopathy for better management, and how telemedicine screenings can increase accessibility to care and make detection of diabetic retinopathy earlier.
Reviewing the Stages and Management of Diabetic Retinopathy
It’s important to recognize the stages of retinopathy in order to determine an appropriate follow-up and treatment plan. Diabetic retinopathy falls into two main classes: nonproliferative and proliferative, the latter having a greater potential for serious visual consequences. Decades of clinical research from major studies including the Diabetic Retinopathy Study (DRS) and the Early Treatment Diabetic Retinopathy Study (ETDRS) has led to the development of a severity scale and management plan for diabetic retinopathy, which is summarized in the American Academy of Ophthalmology’s Preferred Practice Pattern (Figure 1 & 2).
Diabetic Retinopathy Disease Severity Scale and International Clinical Diabetic Retinopathy Disease Severity Scale

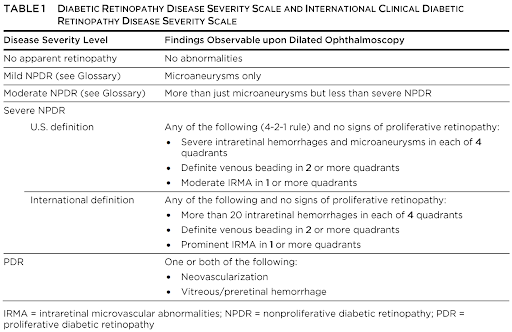
Figure 1. Severity scale of diabetic retinopathy found in AAO’s Preferred Practice Pattern for Diabetic Retinopathy. Further information can be found on Table 1, pages 81-82.
Remember that diabetic macular edema may be present at any severity level of nonproliferative or proliferative retinopathy, and if untreated, can also increase the risk of vision loss.
Initial Management Recommendations for Patients with Diabetes

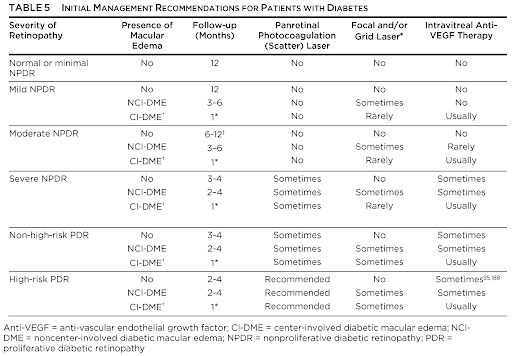
Figure 2. Retinip. Further information can be found on Table 5, page 90.
Imaging Modalities
Widefield and Ultra Widefield Fundus Imaging
Widefield and Ultra Widefield CLARUS fundus imaging can detect mid-peripheral and peripheral retinopathy lesions. What’s the difference between the two imaging techniques?

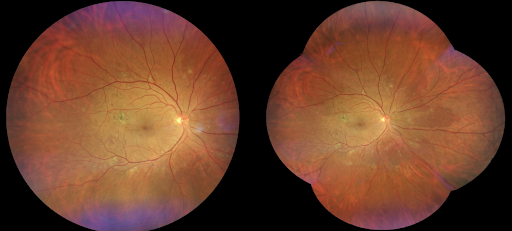
Figure 3: Image courtesy of Carolyn Majcher, OD, FAAO and Munish Sharma, MD, OD, MBA, FAAO.
Widefield imaging (shown on the left) reaches up to the vortex vein ampullae in one shot, obtaining 133 degrees in diameter of retinal views. Ultra-widefield imaging(shown on the right) reaches at least four vortex vein ampullae, covering a diameter of 200 degrees. These images can be montaged to demonstrate up to 80% of the retinal surface in one image.
OCT-A Angioplex Montage
OCT Angiography (OCT-A)evaluates retinal vascularity and capillary function. The high image quality provides fine detail of the vasculature and is a great non-invasive alternative to fluorescein angiography. Also, areas of neovascularization and nonperfusion are identified easily with OCT-A when compared to standard fundus photography.
Patients with diabetic retinopathy often show early signs of nonperfusion within the mid-periphery and periphery of the retina. Individual 8x8mm cube scans of the OCT-A can be combined into a 14x14mm OCT Angioplex montage (Figure 4) to identify areas of retinal nonperfusion further into the periphery of all four quadrants. Areas of nonperfusion indicate an increased risk of developing proliferative diabetic retinopathy, therefore these patients would likely benefit from early treatment with PRP or anti-VEGF injections.

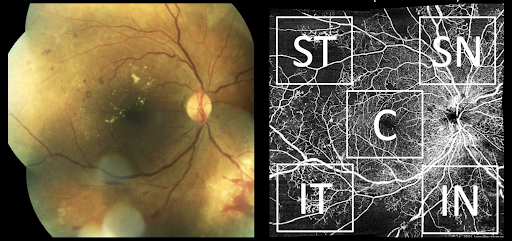
Figure 4: Example of an OCT-A Angioplex 14x14mm montage (five 8mm cube scans) showing areas of nonperfusion in the mid-periphery in all four quadrants that could be missed on standard posterior pole photography. Image courtesy of Carolyn Majcher, OD, FAAO.

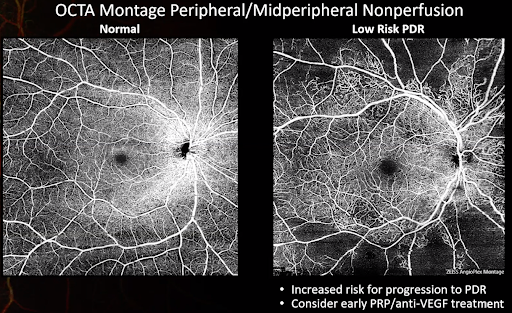
Figure 5: Another example of a patient with peripheral nonperfusion that puts them at high risk for developing proliferative diabetic retinopathy. Patients in this scenario tend to benefit from early treatment with PRP and/or anti-VEGF therapy to prevent progression. Image courtesy of Carolyn Majcher, OD, FAAO.

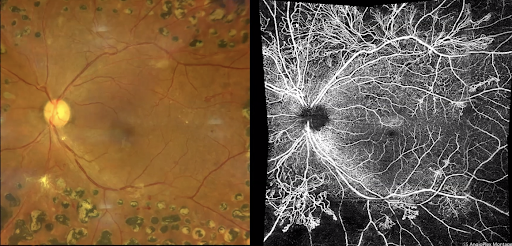
Figure 6: This image shows the difference between mature, involuted neovascularization along the superior arcades versus active, growing neovascularization along the inferior arcades. Active neovascularization appears as leaves on tree branches, while old neovascularization appears as long naked branches. Image courtesy of Carolyn Majcher, OD, FAAO.
The OCT-A offers vitreoretinal interface imaging which is specifically designed to show areas of pre-retinal neovascularization around the optic disc. OCT-A imaging can also identify enlarged foveal avascular zones which can explain the level of central vision loss diabetic patients may experience from retinopathy, even if there is an absence of macular edema or thinning on a regular macular OCT scan.
OCT Macular and Optic Nerve Cube Scan
OCT scans are an excellent way to monitor the status of the posterior hyaloid and retinal changes for progression over time. Early changes to the vitreous or retinal structures may indicate a higher risk for a tractional retinal detachment. High resolution OCT scans can even highlight subtle vitreous hemorrhaging that may not be observed on normal fundoscopy.


Figure 7. The macular OCT scan on the left shows a V-shaped vitreoretinal traction without complications. Two months later, the updated scan on the right shows a vitreous hemorrhage that is decreasing the quality of the scan, and a pocket of subretinal fluid underneath the area of vitreoretinal traction. This patient would now benefit from a referral to a retina specialist for further management and close monitoring. Image courtesy of Carolyn Majcher, OD, FAAO.
Macular cube OCT scans are also used to detect macular edema and changes to the retinal tissue thickness. The high resolution images with a 21 line raster can highlight cystic pockets of fluid, suggesting a risk for retinal detachment.
Increasing Accessibility to Care with Telemedicine
Increasing Accessibility to Care with Telemedicine
Another approach to tackling the increasing volume of diabetic patients is telemedicine. The future requires decentralizing diabetic retinopathy screening methods to smaller optometric practices across the nation to reach more eyecare professionals. In addition to that, offline cameras for imaging should be available in other healthcare settings where diabetic patients are managed, such as family doctors and endocrinologists. This way, all healthcare providers can efficiently contribute to the patient’s care.
Current telemedicine programs involve imaging of diabetic patients at their primary care physician or endocrinologist’s office. The images are then interpreted by an optometrist who determines whether the patient can be monitored or referred for further treatment. This method increases the number of diabetic patients that have access to optometric care. This also provides an opportunity to converse with the patient on the importance of an eye examination for diabetic management.
Implementing Imaging in the Management of Diabetic Retinopathy
Patient Case Example #1
- 29yo American Indian male
- CC: Routine DM exam, wants glasses
- OHx: Severe NPDR OU dx 5 yrs ago
- MHx: DM Type 2 dx 20 yrs ago, last HbA1c 8.2%. Two toes amputated due to DM ulcer
- BCVA OS: 20/30-1
Ultra Widefield CLARUS imaging of the left eye shows neovascularization elsewhere along the superior temporal arcade and extensive hemorrhaging within the periphery of the retina.


Figure 8: Image courtesy of Carolyn Majcher, OD, FAAO.
OCT Angiography imaging shows large regions of nonperfusion which are not easily detected with standard fundus photography. Areas of neovascularization are well defined within the arcades, as well as around the optic disc.


Figure 9: Image courtesy of Carolyn Majcher, OD, FAAO.
Looking at the macular OCT scans, we can see an absence of macular edema. So why is the patient experiencing decreased vision if the macular tissue appears fairly intact? OCT-A imaging revealed the contour of the foveal avascular zone being much larger than a normal, healthy patient. So the reason for decreased vision in this patient’s left eye is likely due to having an enlarged foveal avascular zone secondary to macular ischemia.

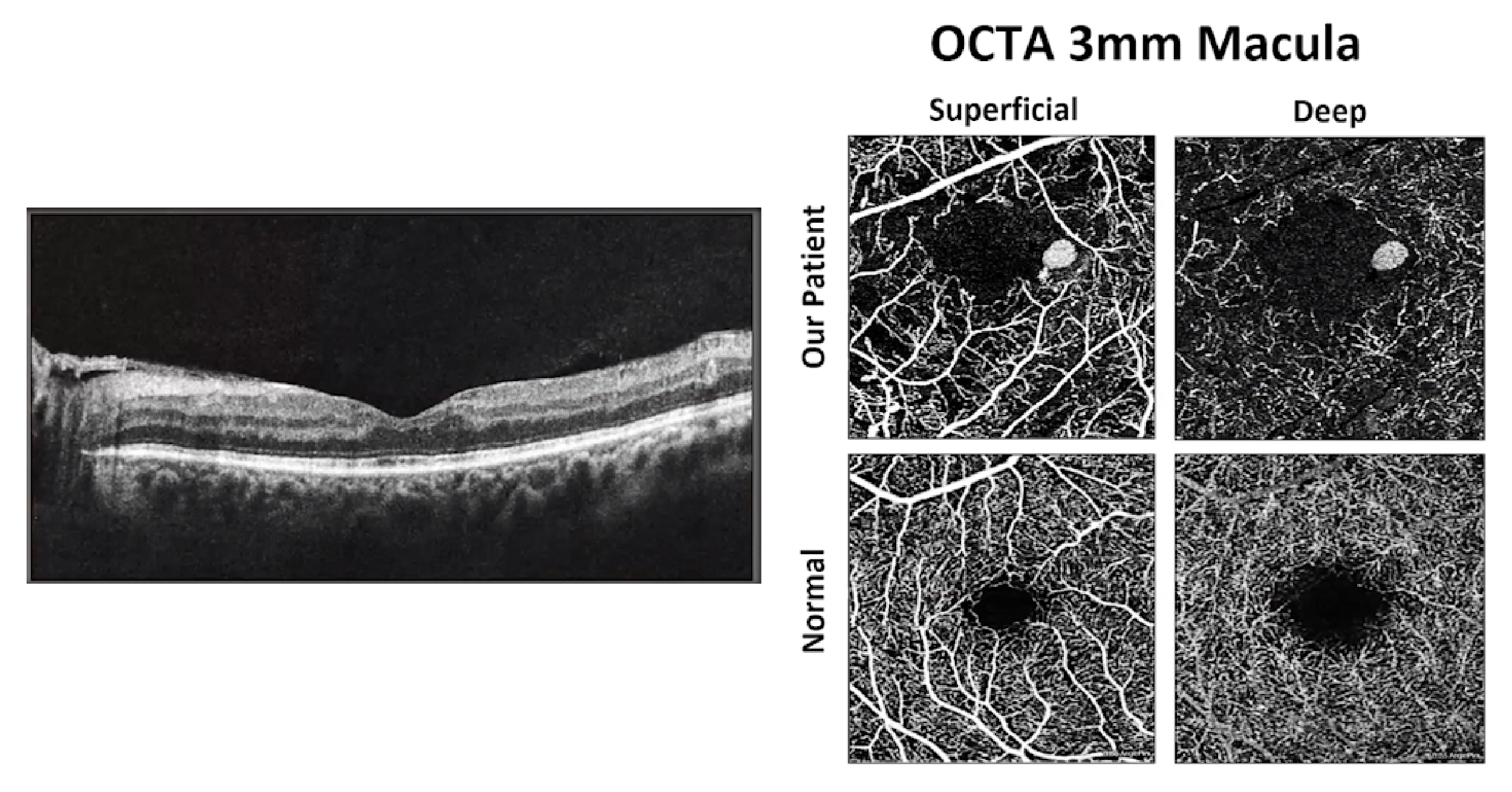
Figure 10: Image courtesy of Carolyn Majcher, OD, FAAO and Munish Sharma, MD, OD, MBA, FAAO.
Focusing back to the optic nerve head, the OCT-A images highlight details of optic disc neovascularization as well as pre-retinal neovascularization from the vitreoretinal interface image. This puts the patient at a high risk of developing a tractional retinal detachment.

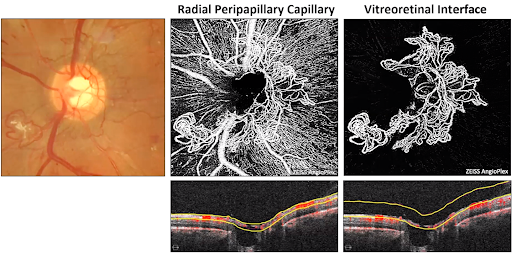
Figure 11: Image courtesy of Carolyn Majcher, OD, FAAO and Munish Sharma, MD, OD, MBA, FAAO.
Taking all of the diagnostic imaging into consideration for the patient’s left eye, we can identify areas of active neovascularization and confidently diagnose the patient with high-risk proliferative diabetic retinopathy without macular edema. Recommended treatment options include PRP laser and possible combination therapy with intravitreal anti-VEGF injections.
Patient Case Example #2
- 50yo American Indian male
- CC: Decreased vision
- OHx: Severe NPDR OU dx 2 yrs ago
- MHx: DM Type 2 dx 11 yrs ago, last HbA1c 11.2%, HTN, high cholesterol, sleep apnea
- BCVA OD: 20/20
Ultra Widefield CLARUS imaging of the right eye shows retinal infarctions and hemorrhaging within the posterior pole and extending into the mid-periphery. There is no obvious neovascularization, however the vasculature close to the optic disc looks suspicious. More diagnostic imaging is required to identify any areas of disc neovascularization.


Figure 12: Image courtesy of Carolyn Majcher, OD, FAAO.
OCT-A imaging shows quite large regions of nonperfusion which are not easily detected with standard fundus photography.

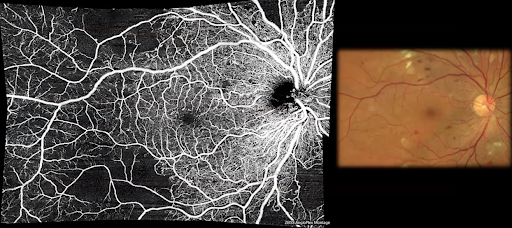
Figure 13: Image courtesy of Carolyn Majcher, OD, FAAO.
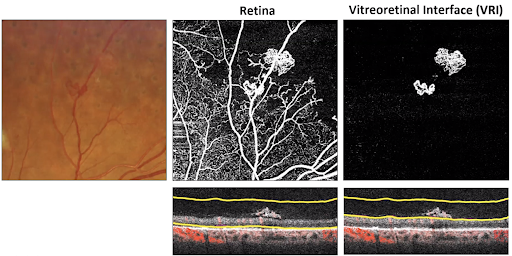
Looking closely at an OCT-A of the optic nerve and vitreoretinal interface imaging, it is apparent that there are some small areas of neovascularization of the disc with overlying vascular fibrous tissue. With vitreoretinal interface imaging, the red highlighted areas through the scan show areas of active blood flow, indicating that the fibrous tissue is likely new.

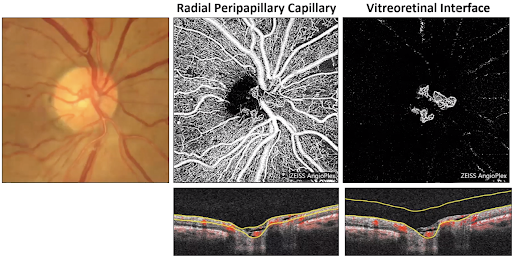
Figure 14: Image courtesy of Carolyn Majcher, OD, FAAO.
This patient’s case is an excellent example of how OCT-A imaging can provide us with an immediate outline of the vasculature, while a fluorescein angiography would require a longer wait time for staining from leakage in the later phase. Although this patient’s vision is 20/20 without macular edema, he still requires treatment with PRP and/or anti-VEGF therapy as his diabetic retinopathy puts him in the high-risk PDR category.
Patient Case Example #3
- 59yo American Indian male
- CC: Increased floaters OD for 2-3mo, rare flashes
- OHx: OS enucleated in 2015 due to chronic inflammation, PRP OD in 2017
- MHx: DM Type 2 dx 12 yrs ago, last HbA1c 7.3%
- BCVA OD: 20/70 PHNI
Widefield CLARUS imaging of the right eye shows areas of neovascularization and hemorrhaging surrounded by few areas of PRP laser scars in the periphery. Notice the zoomed-in area along the superior nasal arcade showing neovascularization with a feeder vessel within the fibrous tissue.

Figure 15: Image courtesy of Carolyn Majcher, OD, FAAO.
An OCT scan can be used to evaluate the integrity of the posterior hyaloid within the area of fibrous tissue. This image highlights a subtle vitreous hemorrhage that cannot be identified on fundus photography. Also notice that the vessels of the neovascularization are scaffolding to the thickened posterior hyaloid membrane.

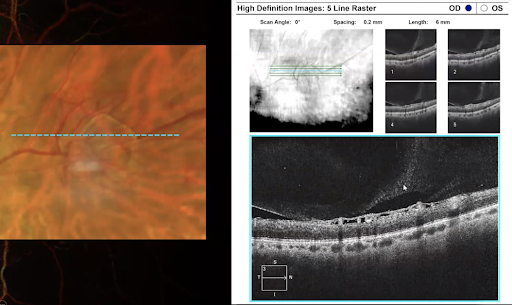
Figure 16: Image courtesy of Carolyn Majcher, OD, FAAO.
The vitreoretinal interface scan provided by OCT-A confirms the area of active neovascularization with blood flow moving through the fibrous tissue.

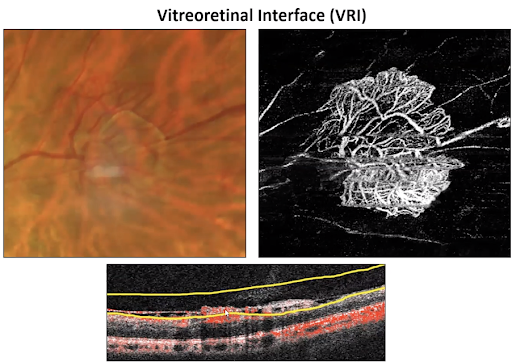
Figure 17: Image courtesy of Carolyn Majcher, OD, FAAO.
The patient was referred to a retinal specialist within one week but did not follow through with the referral. Eight days later, the patient returned to the clinic with increased floaters and hazy vision in the right eye, with counting fingers vision. Widefield imaging showed a pre-retinal hemorrhage overlying the area of active neovascularization, likely due to traction.

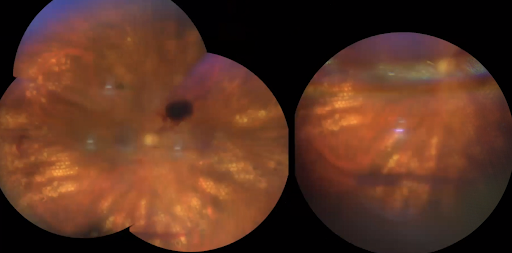
Figure 18: Image courtesy of Carolyn Majcher, OD, FAAO.
Diabetic imaging in this case accurately evaluated the patient’s risk of developing a tractional detachment and hemorrhaging before the complications occurred. Unfortunately, lack of patient compliance to the management plan resulted in further progression of diabetic retinopathy.
Patient Case Example #4
- 63yo American Indian male
- CC: Routine exam, no complaints
- OHx: PRP OS 2 yrs ago
- MHx: DM Type 2 dx 8 yrs ago, last HbA1c 7.9%
- BCVA OS: 20/20
Widefield photography shows a fairly quiet posterior pole with mild cotton wool spots and one area of questionable IRMA vs. neovascularization along a branch of the superior temporal arcade, adjacent to the cotton wool spot. In addition, there is a sclerosed vessel just superior temporal to the macular region with an adjacent area of patchy discolouration, suggesting nonperfusion.

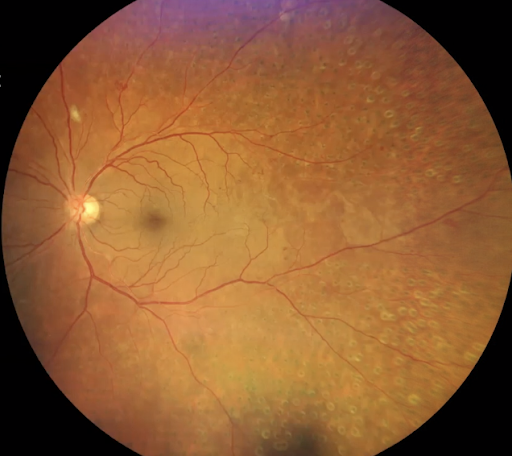
Figure 19: Image courtesy of Carolyn Majcher, OD, FAAO.
These areas need to be further evaluated by OCT-A imaging. OCT-A shows even more areas of neovascularization above the area of questionable IRMA that weren’t even observed on fundus photography. There is a lot of peripheral nonperfusion as well.

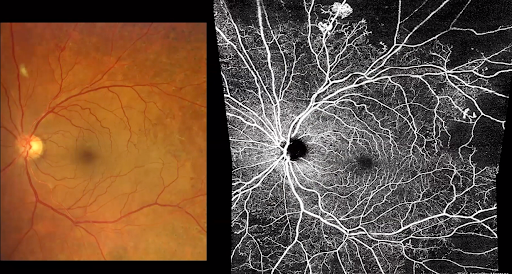
Figure 20: Image courtesy of Carolyn Majcher, OD, FAAO.
A key take-home point with this case is to remember that IRMA and neovascularization tend to develop at the border of perfused and nonperfused retina, as seen in this patient’s OCT-A. In this case, OCT-A imaging has confirmed that the patient’s diabetic retinopathy is progressing and he is at risk of developing a tractional retinal detachment. Based on the imaging results, the patient was diagnosed as non-high-risk PDR without macular edema and was advised to continue monitoring the condition every three months.
Conclusion
Conclusion
Multimodal imaging and telemedicine are absolutely major components of the solution to the challenge that we are facing as optometrists with the increasing number of diabetic patients. These imaging modalities allow us to screen more patients and prevent vision-threatening complications. Widefield and OCT-A montage imaging helps to accurately stage the retinopathy with confidence and efficiency. Decentralizing offline imaging at multiple doctor’s offices increases access to care and opens the conversation about the importance of diabetic eye care management. Implementing these methods in the future will ensure that every diabetic patient has sufficient access to optometric care.
References
References
- American Optometric Association. Evidence-based clinical practice guideline: eye care of the patient with diabetes mellitus. Retrieved from: https://www.aoa.org/practice/clinical-guidelines/clinical-practice-guidelines?sso=y. Accessed Nov 9, 2020.
- Flaxel CJ, Adelman RA, Bailey ST, Lim JI, et al. Diabetic retinopathy preferred practice pattern. J Ophthalmol. 2019;127(1):66-145. doi:http://dx.doi.org/10.1016/j.ophtha.2019.09.025
