


As optometrists, we are all aware of the myriad effects diabetes can have on nearly all aspects of ocular health, especially diabetic retinopathy and ischemic cranial nerve palsies. Prediabetes can also have a big impact on ocular health. Given that those with prediabetes have a 50% increase in risk of developing type 2 diabetes within 5 to 10 years, patients with pre-diabetes and their doctors should be just as concerned for their eyes, vision, and overall health.
This article will discuss the potential effects of prediabetes on the eye.
How does prediabetes affect the eye?
Prediabetes is defined clinically as an HbA1c between 5.7% and 6.4% or a fasting plasma glucose between 100-125 mg/dL. Prediabetes affects one in three adults under age 65 and half of those over 65. Prediabetes is reversible and, if reversed, can prevent type 2 diabetes. But often, people may not know they have prediabetes as it is often asymptomatic.
Many patients may see an optometrist more frequently than they would see a primary care physician. This permits optometrists to have a prime role in diagnosing prediabetes. Often when optometrists see diabetic-related ocular changes, these are primarily in the form of diabetic retinopathy. However, new research suggests that there are changes in the anterior segment of the eye that can show changes from obesity, prediabetes and diabetes well before diabetic retinopathy begins.
Table 11
| Ocular Structure | Obesity | Prediabetes | Diabetes |
|---|---|---|---|
| Corneal endotheleum | NR | NR | Decreased cell density |
| Increased pleomorphism | |||
| Increased polymegathism | |||
| Increase in auto-fluorescence | |||
| Corneal stroma (thickness) | Increased thickness | NR | Increased thickness |
| Increased stiffness (hysteresis) | |||
| Corneal nerve and DCs | NR | Decreased subbasal nerve density | Decreased subbasal nerve density |
| Decreased mechanical, thermal, and chemical sensitivity | |||
| Increased DC density in the central cornea | |||
| Corneal epithelium | NR | NR | Increased risk of neuropathic keratitis and ulceration |
| Increased number and persistence of defects | |||
| Decreased wound healing | |||
| Decreased basal and wing cell density | |||
| Thickened basement membrane | |||
| Conjunctiva | Increased cell metaplasia | Increased cell metaplasia | Increased cell metaplasia |
| Decreased goblet cell density | Decreased goblet cell density | Decreased goblet cell density | |
| Increased hyperemia | |||
| Increased conjunctival microvasculopathy | |||
| Eyelids and Meibomian glands | NR | NR | Increased Meibomian gland dysfunction |
| Increased blepharitis | |||
| Ocular surface Microbiome | NR | NR | Increased risk of acute bacterial conjunctivitis |
| Increased levels of positive bacterial culture | |||
| Increased bacterial diversity | |||
| Tear function and eve symptoms | NR | NR | Decreased tear volume |
DC: dendratic cells
NR: not reported
Corneal changes in obesity, prediabetes, and diabetes
While the effect of obesity and prediabetes on the cornea has not been well established, it stands to reason that changes could be seen before a person is diagnosed with diabetes as it is a continuum of the same disease process. In their cornerstone article on the topic, Richdale et al. reviewed existing research on the effects of diabetes on the anterior segment of the eye, and their paper is must-read for any primary care optometrist. The following section is a brief overview of their findings.
Increased corneal thickness
Average corneal thickness is between 540-560 microns. Central corneal thickness increases by 10-30 microns in patients with type 1 or type 2 diabetes, even if the A1c is well-controlled (<7%). The hypothesis is that increased glucose levels in corneal tissue and increased accumulation of advanced glycation end-products leads to the increased corneal thickness. One study showed increased CCT even in patients with independent risk factors of impaired glucose tolerance and obesity.
Corneal hysteresis also increases in patients with hyperglycemia. This, combined with increased corneal thickness, can lead to an overestimation of intraocular pressure, which may contribute to misdiagnosis of glaucoma.
Corneal innervation
Corneal subbasal nerve length, density and branching are reduced in people with prediabetes, type 1 and type 2 diabetes as measured with in vivo confocal microscopy. Corneal nerve length has been shown to correlate with diabetic peripheral neuropathy in patients with type 1 and type 2 diabetes. More than 50% of people with diabetes have reduced corneal nerve sensitivity due to damaged corneal nerves.
Corneal nerves regulate wound healing and lacrimal response. So decreased corneal nerve density can lead to delayed corneal wound healing, dry eye and ocular surface disease. In fact, up to 70% of patients with diabetes have some type of keratitis, whether superficial punctate keratitis, recurrent corneal erosions or neurotrophic ulcer.
Corneal immune response
Corneal epithelial dendritic cells are antigen presenting cells that initiate the immune response to infectious or inflammatory agents. They are increased in patients with prediabetes, type 1, and type 2 diabetes. This may make patients with prediabetes or diabetes has a prolonged or exaggerated immune response to offending corneal agents.
Figure 1, below, shows in vivo confocal images of central corneal innervation (purple lines), which is reduced in patients with prediabetes and diabetes. Corneal epithelial dendritic cells are increased in patients with prediabetes and diabetes, as shown by the yellow arrows above.

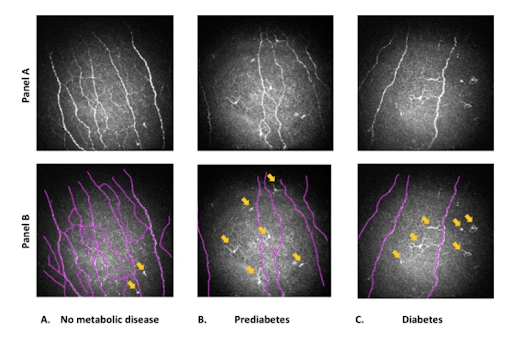
Figure 1
Tear film, conjunctiva, eyelid, and Meibomian glands
Patients with type 1 and type 2 diabetes have been shown to have faster tear break up time, decreased tear production and volume, higher tear osmolarity and increased rates of Meibomian gland dysfunction compared with healthy controls. Even patients with obesity, most of whom also had prediabetes, showed increased conjunctival metaplasia and goblet cell loss which would lead to a lack of mucin in the tear film. These changes are likely caused by both microvascular and neuropathic changes in the lacrimal and Meibomian glands. Additionally, decreased corneal sensitivity leads to a decrease in reflex tear production.
Figure 2 shows Meibomian gland dropout in patients with prediabetes and diabetes compared with healthy controls. None of these patients were previous contact lens wearers.

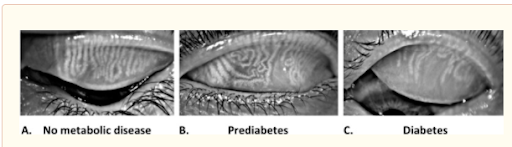
Figure 2
Ocular microbiome
Due to higher glucose levels in tears in patients with diabetes, they are found to have different bacterial species compared with healthy controls. Additionally, patients with diabetes were found to have more bacterial diversity including pathogenic species. This combined with elevated levels of ocular surface inflammation made these patients more susceptible to acute bacterial conjunctivitis compared with health controls.
Other considerations
Patients with poorly controlled diabetes who wear contact lenses should be followed more closely due to increased risk of infection, decreased rate of wound healing and increased rate of corneal endothelial cell loss. They should also be managed more closely when having ocular surgery, for example cataracts and LASIK, due to increased rate of endothelial cell loss compared with healthy controls.
Patient education
We are familiar with discussing lifestyle changes with our patients with diabetes, however we may not always make these recommendations when we see patients we prediabetes or obesity. It is a good reminder that these patients are also at risk of the same complications as our patients with diabetes due to risk of future disease progression as well as the inherent risks those conditions present on their own.
Start with explaining to your patients the disease progression from early insulin resistance and obesity to prediabetes and ultimately type 2 diabetes. Explain what you’re finding on your exam (anterior segment findings may likely be more easy to find than retinopathy in patients with early stage disease). This helps the patient connect their symptoms with their condition and may motivate them to make lifestyle changes that will better control their blood glucose levels.
Encouraging patients with simple lifestyle tips can have a big benefit on their blood sugar levels and overall health. For instance, exercise - whether it’s walking 20 minutes after meals, biking or weight lifting, our patients need to move their bodies. Sleep - patients should aim for 7-9 hours/night, as poor sleep habits can raise our cortisol and blood sugar levels while also increasing sugar cravings throughout the day. Diet - patients with prediabetes, obesity or diabetes should focus on Limiting carbohydrate consumption to 45% of total daily calories to help improve A1c. Eating within a 10 hour window daily can also help achieve adequate blood sugar control.
For more lifestyle tips for diabetes and obesity, check out the Vision Refocused YouTube channel.
Conclusion
Having quantifiable data to show patients can be useful in explaining how their elevated blood glucose is affecting their eyes, even in the absence of diabetic retinopathy. Whether it’s an increase in pachymetry, intraocular pressure, corneal hysteresis, Meibomian gland dropout, dry eye or recurrent bacterial conjunctivitis, correlating these specific ocular findings to their systemic health can motivate patients to better care for themselves. So often when a patient does not have retinopathy, we say they are “fine” and send them on their way for another year.
Eye care providers need to pay closer attention to the anterior segment in patients with obesity and prediabetes, as well as diabetes, to interject ways patients can keep their ocular health optimal and preserve their vision in the long-term.
