Eyecare providers have the privilege of providing care to patients of all backgrounds, and this privilege includes caring for patients with disabilities. According to the Centers for Disease Control and Prevention (CDC), 61 million adult Americans have some type of disability.1
Quite often, the families and caregivers of patients with disabilities play a major role in health outcomes for their loved ones, and it is vital that the
eyecare provider communicate effectively with the family members and the patients themselves.
This article provides general guidelines for caring for patients with disabilities, as well as optimizing eyecare outcomes by involving their family members and caregivers.
What are intellectual and developmental disabilities (IDDs)?
- Developmental disabilities are a broader category to describe the lifelong challenges that can be intellectual, physical, or both.
- Intellectual disability is a term to describe differences in intellectual functioning (learning, reasoning, problem-solving) and adaptive behavior (social and life skills), which are present before age 18.
Intellectual and developmental disability refers to situations in which intellectual disabilities are present. For example, disorders of the brain, spinal cord, and nervous system can affect intelligence and learning, which lead to speech or language delays, seizures, behavioral disorders, and difficulty with movement.
Cerebral palsy, Down syndrome, Fragile X syndrome, and autism spectrum disorders are examples of IDDs related to the nervous system.
IDDs that may be encountered in an eyecare setting include:
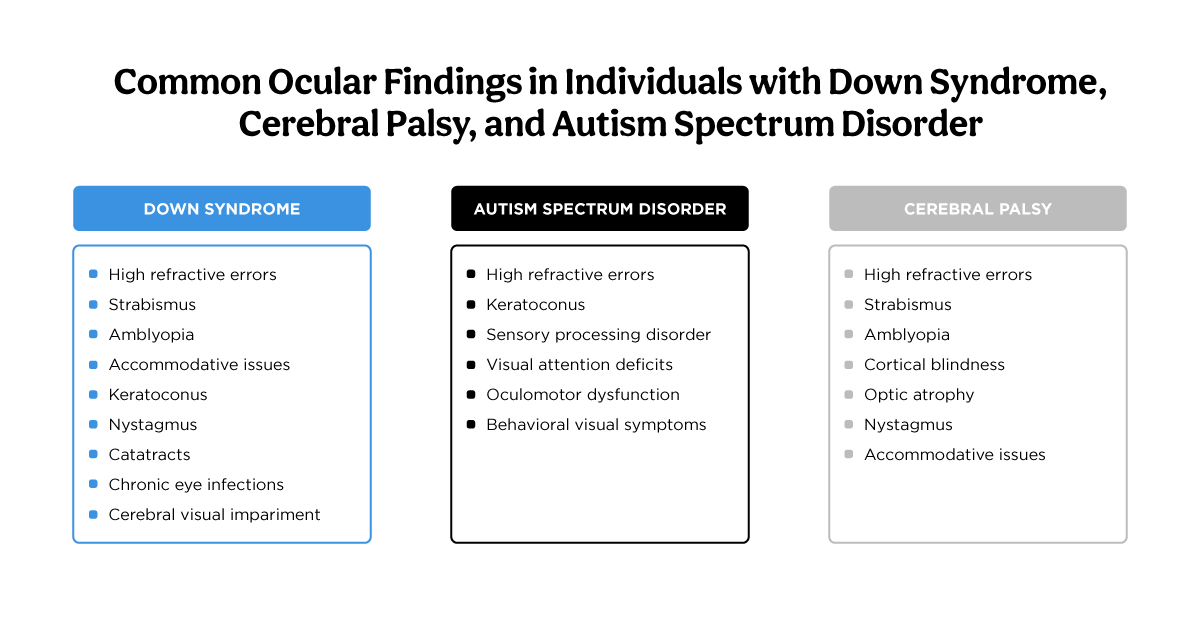
Three of the most common out of the list above are autism spectrum disorder (ASD), Down syndrome (DS), and Cerebral Palsy (CP). Of these conditions, common ocular issues encountered include high refractive errors, strabismus, amblyopia, and keratoconus.
Figure 1 outlines common ocular findings associated with autism spectrum disorder, Down syndrome, and Cerebral Palsy.3-5
Image 1: Adapted from Haseeb A et al., Chang MY et al., and Sasmal NK et al.
Recognizing the unique healthcare needs of patients with IDDs
It is vital to remember that each person with a disability is a unique human being, and it is impossible to generalize or universalize each person’s needs or characteristics. They are not defined by their disabilities, and they deserve a comprehensive eye exam to meet their visual needs.
Terminology about disabilities continues to be an evolving topic. Some patients and their families may identify with the term “disability,” while others may see themselves as “differently-abled.” The provider should follow their lead in referring to their abilities.
This article provides general guidelines for approaching an eye exam for a person with developmental and intellectual disabilities. Because each individual is unique, these guidelines may not apply to all but will provide a good starting point.
Establish a rapport with the family and patient
- How to most effectively communicate with the patient
- How to best examine the patient, and
- The treatment and management plan.
A friendly and calm greeting should be addressed directly to the patient with good eye contact and then to their family members/caregivers while respectfully asking about their relationship with the patient. As you walk in, observe the body language of the patient and their family members. Are they making eye contact with each other, what is the method of communication if they are interacting, and what is the mood?
Some friendly opening questions to the patient, if verbal or using a communication device, might be:
- What do you like to do for fun?
- What is your favorite music?
- Who is your favorite character?
Responses to these questions may give answers that will serve as exam tools later in the appointment. The doctor can ask the caregiver for their advice on the best approach to the examination, both verbal and physical. This may allow you to be aware of a patient’s aversion to being touched, clapping, cheering, or a preference for high fives and a certain type of music as positive reinforcement.
An example of how to ask would be, “Is there anything I should know about Sally’s preference for being examined or how she likes to be told she did a great job?”
Don’t forget the family and their healthcare journey
Throughout the exam, be sensitive to the
patient's and family's emotional needs due to complex medical histories and post-traumatic stress disorder (PTSD) from a potentially complex journey with their loved one. They have likely seen many medical professionals, which affects how they interact with you as the provider.
First-person language vs. identity-first language
For patients who are old enough to independently respond for themselves, it is a best practice to speak in the first person to the patient, even if the family member needs to add to their response. In this way, the patient is respected and has a voice in their own health outcomes.
In addition, when referring to a person with disabilities, the provider should follow the patient’s lead. Some prefer person-first language, while others prefer identify-first language.
- Person-first language: Uses the person before the diagnosis while speaking about them.
- Identify-first language: Uses the diagnosis/condition before the person.
Instead of saying, “Downs’ kids often have high plus prescriptions,” it is best practice to say, “kids with Down syndrome generally are more prone to having high plus prescriptions.” Individuals with
autism spectrum disorder may prefer identity-first language, such as saying, “he is autistic.” But a person with Down syndrome would not want to be referred to as “he is the Down syndrome boy.” This can be confusing for health professionals, but when in doubt, use person-first language and follow the family’s and patient’s lead.
Tips for attaining an accurate history
Patients with special needs often have complex case histories, which necessitate efficiency and perceptiveness to verbal and nonverbal cues. It is vital for the clinician to be able to prioritize the
relevant information to ocular health and to probe eye history further while ensuring that the patient and their family feel heard and seen as a whole person and not just a pair of eyes or a list of body parts.
During the history, use observational assessment to obtain clues about what aspects of the exam may need to be adjusted for the patient by asking:
- Is the patient sitting on the chair independently, or are they sitting on the lap of the caregiver or in a stroller?
- Is the patient mobile, speaking verbally, and looking around the room with alertness?
- What are the emotions in the room—is the patient or family member anxious, tired, calm, excited, etc.? Is the family member prompting the patient to say hi?
Ensure that you are at eye level with the patient, maintaining an open and friendly posture. Keep some distance between you and the patient, giving them time to adjust to your presence if they have sensory issues. Consider not wearing your white coat for the exam if it would help for a patient who is sensitive to medical exams.
Recording an accurate medical history for patients with IDDs
Medical history can be complex in patients with disabilities. It is most efficient to review all medical conditions in the problem list in the EHR or patient questionnaire in list form and then ask further detailed questions for conditions that merit further probing.
An example would be: “To confirm, besides hearing loss, there is a g-tube for feeding, strabismus, amblyopia, and hypotonia. Is there anything else I have missed? Let’s talk more about the eye turn and amblyopia. How is she doing with eyeglass wear? Is her right eye still turning in when she’s tired?”
Recording an accurate social history for patients with IDDs
Social history should always include questioning about a patient’s functional needs. This will inform the need for a near prescription, special lens materials, further testing, or care coordination with daycare, school, and other organizations caring for the patient.
- Does the child have an Individualized Education Plan (IEP)?
- What are the child’s visual accommodations in school (if any)?
- What are their functional needs and abilities at home?
- What does the child do for fun?
- How much daily screen time does the child have?
- Are they compliant with their glasses wear (if any)?
- How far away does the child hold a book?
- Are any atypical eye movements noted?
- What do they like to do for fun?
- What kind of visual needs are there during the day? (The response should indicate if they have a job, are in school, in a day program, etc)
- Tell me about what kind of screen time (TV, tablet, phone) there is during the day.
- How far away is the reading material held?
- Any symptoms of dryness, burning, or watering?
- Is the current type of glasses working well (progressive, bifocals, or two separate pairs)?
Think outside the box for eye exams
The key to exams that do not follow the usual eye exam routine is to be flexible. As early as calling the patient from the waiting room, the doctor can observe the patient’s functional vision and communication skills as a starting point for the exam.
Sensory issues are common
The doctor will need to take into account a patient’s sensitivities in order to conduct the exam. For example, a child with
Down syndrome may be happy to be there but may tend to lose attention quickly. The doctor can sing a song to recapture their attention or ask the family member what would work best.
Keep in mind that patients with speech delay may need extra time to provide an answer. At times, if an exam becomes overwhelming, a patient may benefit from a break in a quiet room.
Respect the patient’s boundaries, and work with the family to navigate the need for physical touch during the exam.
Set goals with the patient and their family
A full exam may be exhausting for both the patient and their family members. Once the history is complete and you have an idea of how the exam will proceed, it is important to involve the
patient and family in deciding the course of the exam. If cooperation or fatigue are issues, the provider can set goals for that day’s visit and set a course of action with the patient and family.
A good assessment of strabismus status was achieved today, but the patient is becoming agitated. At that point, the provider can discuss with the family whether cycloplegic refraction should be done on this day or another day.
You may even want to start the exam with the expectation that it may take multiple exams to complete a full exam so that the parents/caregivers know what to expect and are not disappointed if you ask them to come back!
Set goals with the patient and their family
A full exam may be exhausting for both the patient and their family members. Once the history is complete and you have an idea of how the exam will proceed, it is important to involve the patient and family in deciding the course of the exam. If cooperation or fatigue are issues, the provider can set goals for that day’s visit and set a course of action with the patient and family.
A good assessment of strabismus status was achieved today, but the patient is becoming agitated. At that point, the provider can discuss with the family whether cycloplegic refraction should be done on this day or another day.
You may even want to start the exam with the expectation that it may take multiple exams to complete a full exam so that the
parents/caregivers know what to expect and are not disappointed if you ask them to come back!
Potential strategies for engaging the patient include:
- Interact in the waiting room first before transitioning to the exam room.
- Sing nursery rhymes.
- Playing a video of a favorite character on an acuity screen or phone.
- Give them something interesting to hold.
- Give plenty of positive reinforcement after checking for preferred methods (ex., high fives).
- Don’t be afraid to do appropriate testing in a non-exam chair if more comfortable for the patient.
- Redirect the patient to an interesting task or stimulus if they are distracted.
- Talk about their favorite singer, celebrity, book, movie, etc.
Performing entrance tests on patients with disabilities
Taking visual acuity can be a fun game for the patient if done with positive reinforcement and efficient movements. Entrance tests should be done slowly, explaining to the patient what will be done and quickly moving on if something is not working so that you can come back to the test later. It is important not to make assumptions about what the patient can or cannot read. Some will be able to read letters, numbers, or shapes, and others may benefit from Teller acuity cards.
The provider should have a variety of fixation targets to turn to, depending on the patient’s ability to fixate and cooperate with testing. This may range from interesting toys that make sounds and light up, to movies on a screen at 20 feet, to their preferred media source held at a distance.
Measuring refraction
Objective findings such as
retinoscopy and cycloplegic refraction are essential to finalizing the glasses prescription. Other strategies are retinoscopy over existing glasses and holding lenses over the glasses for quick adjustments.
Be careful to explain the test and move smoothly, without erratic movements around the room and the patient. It can help to show the patient what the light looks like on your hand and then on their hand to show that there is no pain from the light. Use fun targets if cooperation is needed, and move efficiently.
Performing a slit lamp exam
Placing the chin in the
slit lamp can be fun or feel very constricting to a patient. If the patient is unable to sit in the slit lamp, a gross exam can be done with a 20D lens for major structures, and a shadow test can be done for angle assessment.
Some patients feel more comfortable with a provider singing a silly song or asking questions about fun topics while gently and efficiently doing the exam.
Instilling eye drops
Eye drops can be scary for any patient, and the provider will need to make quick assessments about the best way to instill the dilating drops.
Some strategies for instilling eye drops include:
- A social story about the eye exam experience before the appointment.
- The closed eyes method, where a drop is put on the corner of each eye, and on the count of three, the patient opens their eyes (explained as a game) for the “tickle” of the drops.
- A properly-prepared spray of the dilating drop combination can be an alternative strategy.
- Prescribing the dilating drops to be administered by the family before the appointment if the patient is already established in the clinic and is more successful with prior preparation and less waiting time.
Performing a fundus exam
Bright lights can be difficult for any patient. Interesting visual targets like videos on a phone held in various positions or having a family member stand at different points of the room can assist with fixation during the binocular indirect ophthalmoscopy (BIO) exam. Younger patients may need assistance from their families to hold them firmly enough for a quick BIO exam.
When a patient is not cooperative and does not wish to be examined, the provider will need to determine, in cooperation with the family, whether an exam under anesthesia makes sense. If a patient has risk factors for
retinal issues or has conditions impacting their vision, an exam under anesthesia may be in their best interest.
The provider should always ensure the patient has stable and functional vision, and good ocular health and look to optimize their ability to meet their visual needs.
Communicating the management plan with the patient and family
The management and treatment plan for the patient should be clear, concise, and summarized at the end of the visit.
The provider should ask questions like:
- “What question or concerns do you have for me?”
- “Is there anything you want me to explain further?”
Be careful to avoid stating management plans that may elicit guilt in a family member who has multiple complex issues to manage at home. This kind of framework makes the point of the
importance of compliance, emphasizes your good intentions, and lets the family know that you are on their side.
For example, “If she doesn’t wear her glasses full-time, her amblyopia may not improve” would be better said as “I know we both want the best vision for your daughter. If she does her best in wearing her glasses all the time, I think we can improve her vision during this critical age. I have some resources (see below) that may help you develop new strategies to motivate her to wear her glasses.”
Making optical recommendations
Optical recommendations from the provider should take into account any sensory needs and anatomical asymmetries as appropriate. Patients with sensitivity to frames on their faces will benefit from
specialized frames that are lightweight, flexible, and durable.
Some potential brands are: FlexWear, Dilli Dalli, NanoVista, Tomato Glasses, Specs4Us, and Gizmo glasses. Be aware of the need for a nose pad for eyewear stability, especially if there is minimal to no nose bridge. This will dictate which brands are generally best for your patient.
Ending the appointment with encouragement
A family with a loved one with complex medical needs usually appreciates encouragement as the final note of their visit.
Examples of things you could say at the end of the appointment include:
- “You have a wonderful daughter, and I want to say you are doing a great job as her parents.”
- “My day is better now that I’ve heard some music from [patient’s favorite musician]!“
- “Thank you for sharing your son with me today. You are all doing a great job, and I look forward to seeing you again next time.”
Scheduling follow-ups
For patients with complex medical needs, they may need the doctor to advocate for them at specific times of day for follow-ups.
- Schedule follow-ups at optimal times for the patient (less fatigued, avoid meal times).
- Suggest further social stories, as needed.
- Set goals for each visit, and take into consideration other appointments and logistical issues such as transportation, feeding schedules, etc.
Be an advocate for their healthcare needs
When gaining cooperation or subjective responses for an eye exam is more difficult, a provider must decide whether their care has been sufficient or if further care is needed. Unfortunately, people with developmental and intellectual disabilities can be dismissed as having vision that is “adequate,” and the provider stops there.
Owens et al. reported that available data suggested that vision problems such as refractive errors, strabismus, cataracts, and
keratoconus were more common among individuals with IDDs than those without. As optometrists, we can be part of the team of healthcare providers who ensure healthcare equity for patients with IDDs and be advocates for their eye health and overall well-being.
It can be difficult to navigate the healthcare system, especially for patients with complex needs. When left to their own efforts, it can be frustrating for a family member to arrange for the scheduling or interprofessional communication that they need. The provider should be quick to make a phone call, write a letter, or other forms of communication needed to assist the patient and their family in any assistance necessary to make their visit successful.
It is important to remember that in some cases, just getting to the appointment is stressful and requires careful planning on the family’s part to arrive at your office successfully.
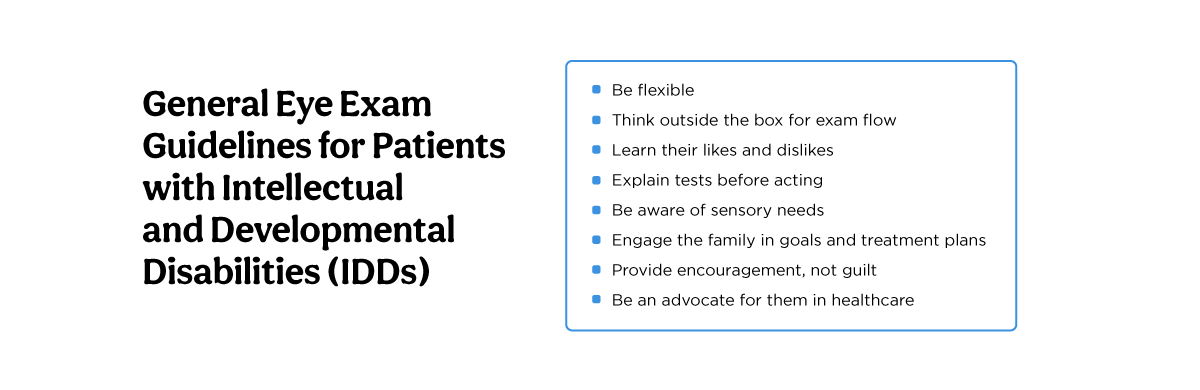
Top tips to remember when treating patients with IDDs
Remember the tips below to ensure your IDD patients have the most positive office experience and achieve their best vision results.
Figure 2 highlights general eye exam guidelines for patients with intellectual and developmental disabilities.6,7
Figure 2: Courtesy of Amy Moy, OD, FAAO, CPCO
Eyecare resources for patients/families with disabilities