


Meibomian gland dysfunction (MGD) is characterized by insufficient quality and/or quantity of meibum produced from the meibomian glands. Appropriate production of meibum is essential for maintaining optimal ocular surface homeostasis and contributes to vision.1
Several studies have shown the close link between MGD and age, screen time, medication use, and systemic conditions, as well as the connection between MGD and other ocular conditions such as Demodex blepharitis and chronic dry eyes.2-4
More about MGD
According to the TFOS DEWS II report, dry eye syndrome affects hundreds of millions of individuals globally.3 Approximately 50% of the US population suffers from dry eyes, with 50 to 80% of these cases being classified as its evaporative form due to MGD.1,3,4 Studies have also estimated that within the population of individuals aged 60 and over, at least 70% of these individuals suffer from MGD.4
Risk factors for MGD:4-7
- Age (primary risk factor)
- Eyelid defects
- Demodex infestation
- Cosmetic application and contact lens use
- Medication / hormonal changes
- Environmental conditions or factors
- Screen time
- Systemic conditions (ex., rosacea, psoriasis, atopic dermatitis)
Signs and symptoms of MGD:4-7
- Burning sensation
- Itchy eyes
- Red / inflamed eyelid margins
- Watery eyes
- Pain / photophobia
- Blinking often
- Contact lens intolerance
- Blurry vision
- Foreign body sensation / grittiness / sandy sensation
Physiology of the meibomian glands
The meibomian gland (MG) is a holocrine acinar gland located at the tarsal plate of the eyelids.2,4 There are roughly 20 to 30 linear-shaped meibomian glands in each upper eyelid and 30 to 40 present in each lower eyelid.2,4
Each gland consists of a central duct spanning the complete length of the gland, which opens at the surface of the eyelid margin via the excretory duct.2 Inside the acini that make up each MG resides many specialized cells called meibocytes, which are responsible for the development of meibum.2,4
When the acini mature, they release meibum into the central duct by rupturing, and during each blink, the clear meibum is passively squeezed out of the central duct and onto the surface of the eyeball to stabilize the tear film.2
Meibum consists of an array of lipids such as free fatty acids, cholesterol and waxy esters, as well as proteins which include cytokines, immunoglobulins, enzymes and proteoglycans.4 Insufficient production or low-quality production of meibum by the meibomian glands compromises the integrity of the tear film, leading to the evaporative form of dry eye disease.3,4
Age-related meibomian gland dysfunction
Aging is a common and unavoidable risk factor for many conditions. Similar to cataract formation and macular degeneration, MGD and dry eye disease can progress with age.1,4-7
As we age, MGD may develop due to structural or functional changes within or nearby the MGs, including:1,4-7
- Changes in the size of the meibomian glands
- Structural changes at the eyelid margins
- Hyperkeratinization of the central duct of the meibomian glands
- Compositional changes to the meibum
- Decreased cell proliferation of the acinar basal cells
- Potentially increased infiltration of inflammatory cells in the meibomian glands
It is important to note that all of these changes eventually lead to meibomian gland atrophy and dropout.
Studies on the causes of age-related MGD
Several studies have shown the correlation between age and meibomian gland size.1,6 It is hypothesized that the meibomian glands become smaller in size, which can lead to decreased production of meibum.1
Other studies suggest morphological changes to eyelid; structural changes include rounding of the upper eyelid margin, increased vascularity at the eyelid margin, and increased incidence of telangiectasia and hyperkeratinization of the periocular skin.4
Hyperkeratinization
One of the most mentioned causes of age-related MGD (ARMGD) includes hyperkeratinization of the central duct of the meibomian glands.1,2,4-6 Patients with MGD have about 10% more keratin protein in meibum than those without MGD.4 It is proposed that as we grow older, levels of reactive oxygen species (ROS) increase, leading to keratin accumulation within the epithelial acinar cells of the meibomian gland.4
This causes duct obstruction, meibum stasis, and plugging at the meibomian gland orifices, which results in the atrophy of the acini and meibocytes, eventually leading to poor production of meibum, both qualitatively and quantitatively.1,4,5 The long-term effect of this process is meibomian gland atrophy and dropout.3
Decreased lipid interactions
Recall that meibum is composed of a variety of lipids and proteins.
Infrared spectroscopy analysis of meibum suggests that the composition of the meibum changes with age due to:4
- Decreased lipid-lipid interactions that occur in response to increased hydrogen bonding
- Increased polarity
- Changes to the types of bonds between the lipids
These studies suggest that such changes can occur with increased oxidation in aging.4 Changes to interactions between the components that make up meibum alter the consistency and color of the meibum, leading to hyperviscosity and hyposecretory MGD.
Increased oxidative damage
Additionally, some studies suggest that increased oxidative damage with age leads to low-grade chronic inflammation, a hallmark of aging, and overtime this chronic form of inflammation may lead to infiltration and accumulation of inflammatory cells in the meibomian glands potentially causing meibomian gland dropout.4
The downregulation of peroxisome proliferator-activated receptor gamma (PPARy) with age is also a notable cause of ARMGD. PPARy is a hormone that regulates lipid production, cell differentiation of sebocytes and adipocytes, and it is proposed to be a marker for meibocyte differentiation.1,2,4
The downregulation of PPARy receptor signaling contributes to disuse and atrophy of the acini, leading to meibomian gland dysfunction.2,4
Diagnosing age-related meibomian gland dysfunction
Diagnosing and managing age-related MGD requires an understanding of the severity of the MGD. Clinicians must evaluate the ocular surface, periocular skin, and eyelid margins.
It is important to observe for any structural eyelid margin changes, abnormalities at the meibomian gland orifices, and the integrity of the conjunctiva and cornea to aid in the evaluation of evaporative dry eyes. Additional testing can be performed, such as Schirmer test and meibography.5,6
Figure 1: Meibography images of a patient's upper and lower eyelids to show the meibomian glands.

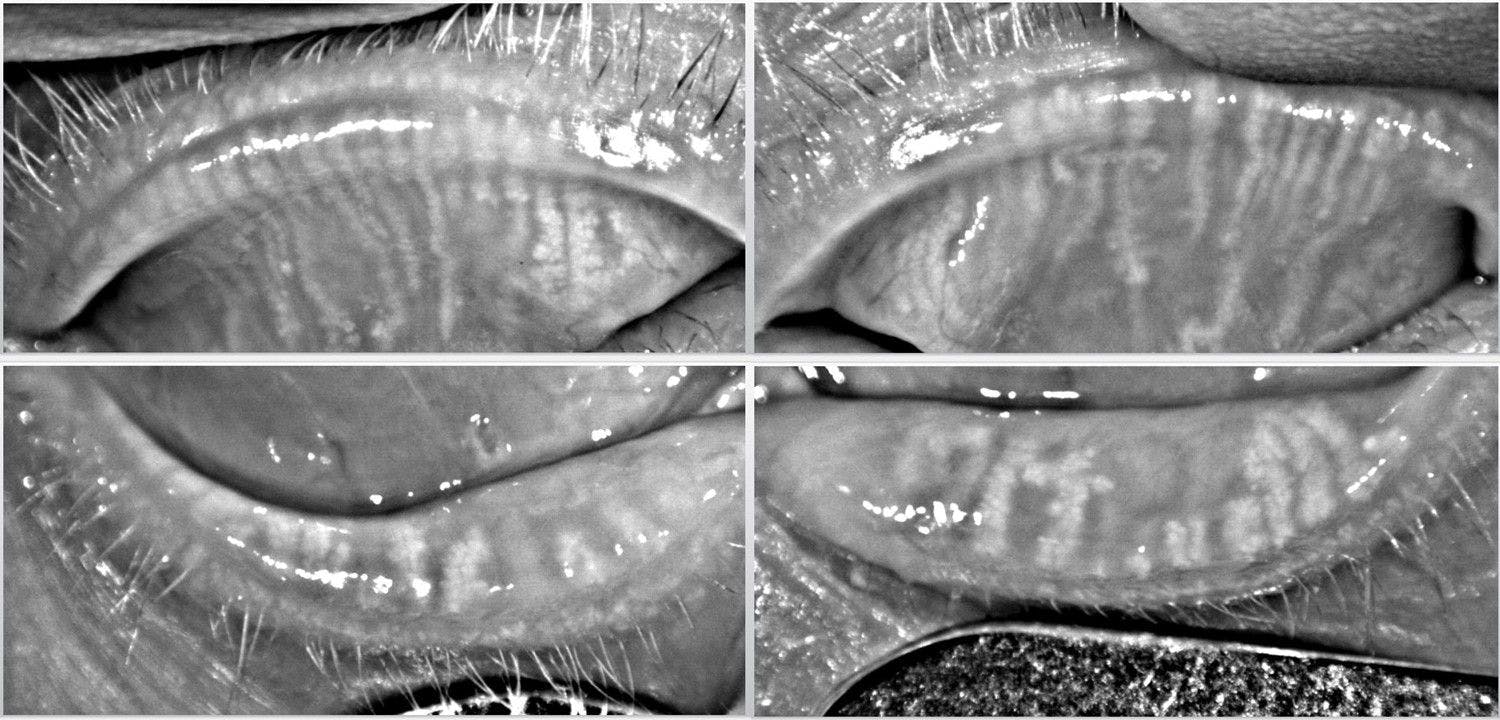
Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO.
Steps for evaluating patients for MGD include:
- General observation:
- Blink rate and quality of blink
- Reduced blink rate: 14 to 17 blinks per minute
- Complete vs. incomplete blinking
- Blink rate and quality of blink
- Slit lamp
- Eyelids / eyelashes: Presence of collarettes/crusting
- Eyelid margin: Presence of rounding/thickening, telangiectasia
- Meibomian gland evaluation: Appearance at the MG orifices
- Meibomian gland expression: Assess the quality of meibum
- Conjunctiva: Injection / hyperemia
- Cornea: Presence of punctate epithelial keratitis (PEK), measure tear breakup time (TBUT)
- Diagnostic dyes
- NaFl and lissamine green to assess the integrity of the conjunctiva and cornea
- Measure TBUT with NaFl
- Normal: TBUT ≥ 10 seconds
- Evaporative DES: TBUT < 10 seconds
- Schirmer test
- Quantify tear production
- Normal: ≥ 15mm of wetting after 5 minutes (no anesthetic)
- Moderate to severe DES: < 10mm of wetting
- Quantify tear production
- Meibography
- Image the upper and lower tarsal plate and compare to normative scale to grade meibomian gland atrophy and dropout
- Interferometry
- Analysis of the lipid layer of the tear film
Table 1: Grading MGD based on meibum expression and quality.6 Note, *patients with Grades 2 to 4 MGD typically experience tearing due to excessive tear evaporation and present with red or inflamed eyelid margin, a marker for inflammation, and **Grade 4 MGD may also present with conjunctival injection
| Grade | Assessment |
|---|---|
| 0 | All glands are unobstructed with clear meibum, visible meibomian gland orifices |
| 1 | One or two glands are partially obstructed; clear meibum is digitally expressed |
| 2 | Three or more partially obstructed glands with mildly opaque meibum* |
| 3 | One or two obstructed glands, several partially obstructed* |
| 4 | Three or more blocked glands with the majority of others partially blocked*,** |
Table 1: Courtesy of Kaur et al.
Preventing age-related MGD
Patients diagnosed with ARMGD, irrespective of its stage, should be educated on clinical findings to promote better adherence to the treatment of the condition. Any underlying ocular or systemic conditions, such as ocular allergies, Demodex infestation, blepharitis, or rosacea, should also be managed.6,9
Since ARMGD may remain asymptomatic in early stages, it is crucial to educate patients that treatment can limit progression and the development of symptoms.9
Proactive prevention is preferred
The best form of treating a condition is preventing it from developing altogether. Prevention of ARMGD can begin with maintaining good eyelid hygiene, which may include emphasis on cleaning near the eyelid margin and eyelashes and the addition of eyelid cleansing wipes or hypochlorous acid to the periocular skin to reduce the risk of infection.5,6,9
Additionally, managing environmental factors, such as avoiding direct wind to the face and eyes, using humidifiers, and avoiding contact with allergens, may prevent damage to the meibomian glands and the areas surrounding the glands, decreasing the risk of developing ARMGD.6,7
Studies reveal the relationship between prolonged screen viewing and decreased blink rate.6,7 As previously noted, blinking is the force that passively expels meibum from the meibomian glands and onto the surface of the eye.4,6,7
Utilizing the 20-20-20 rule during prolonged screen time can also be useful; this rule instructs the patient to look about 20 feet away after every 20 minutes of continuous screen time, and blink for 20 seconds, then resume computer work.6,9
Treatment options for age-related MGD
For mild cases of MGD (Grade 1 to 2), gland expression can be improved by incorporating warm compresses at least twice a day for 5 to 10 minutes, followed by digital eyelid massage.5
Dietary omega-3 fatty acids (salmon, tuna) or supplementation may also benefit, along with lubricating eye drops, especially when working on the computer.5,6
Artificial tears with lipid components, such as Refresh Mega-3 or Systane Balance can also aid in age-related MGD.9
Topical medications for age-related MGD
In moderate to severe cases of ARMGD, consider adding topical macrolides or tetracycline eye drops, both of which have been shown to possess anti-inflammatory properties.6 The addition of lubricant gel eye drops at bedtime may further improve the condition and reduce patient symptoms.5,6
For severe cases, implementing lubricant eye ointment before bed may be beneficial, along with considering topical anti-inflammatory-specific eye drops like cyclosporine or a topical steroid eye drop.5,6
Varenicline
Additional treatment options include Tyrvaya, a prescription nasal spray with the generic name Varenicline, which treats dry eyes by stimulating the trigeminal pathway thereby increasing the production of all three components of the tear film and aiding in meibum production.5,6
Miebo
Miebo, or perfluorohexyloctane, is available for the treatment of dry eye, and is the only eyedrop that is FDA-approved for treating evaporative dry eye syndrome, a condition mainly caused by MGD.
Meibo is indicated to be used four times a day, and studies have shown the efficacy of this tear film stabilizer, as it mimics the function lipid layer of the tear film by preventing tear evaporation.10
In-office treatments for MGD
In severe cases of MGD, if the above treatment options are ineffective, more invasive in-office treatment options such as intraductal probing, eyelid exfoliation, electronic heated devices, and laser therapy may be effective.5,6,12,13
Intraductal probing involves using a probe to dilate the meibomian glands; facilitating the release of meibum.6 Blephex is a tool used to exfoliate the eyelid margins and can be used to clean the orifices of the meibomian glands.6
Electronic devices like LipiFlow and iLux are in-office treatments that deliver heat to the upper and lower eyelids, while applying direct compression to simultaneously liquify and express the meibomian glands.5,6
In addition, MiBo Thermoflo is an in-office tool that delivers heat to the meibomian gland area for a short period of time, providing immediate improvement to patient’s symptoms, as well as improving clinical tear break up time (TBUT).5
TearCare is another form of in-office thermal therapy, which when coupled with manual gland expression, has been as effective as LipiFlow in improving tear break up time and meibum quality.11
IPL and radiofrequency for MGD
Intense pulsed light (IPL) has been introduced to dermatology over decade ago for the management and treatment of inflammatory conditions like rosacea, however more recent studies have proven its application to ophthalmology and optometry by its use in the reduction of eyelid margin inflammation and hyperemia; this also aids in the treatment of MGD and dry eye syndrome (DES).5,12
Although the mechanism of action is not quite understood, IPL treatment has shown improvement in both the patient’s symptoms, meibomian gland function and meibum quality after several treatments.5,6 IPL is extremely beneficial if MGD is associated with an inflammatory condition such as rosacea.5,6,12,13
Radiofrequency (RF) is another procedure commonly used by dermatology for skin tightening by using radio waves to generate heat to the skin; studies show that RF can aid in the management of MGD when applied on the eyelids, improving tear film stability and meibomian gland function.13
Several studies have shown that the combination of IPL and RF is more beneficial than one procedure alone; combining the two resulted in further improved the OSDI score, non-invasive TBUT, and meibography.
Figures 2 and 3: Slit lamp images of lower eyelid long-standing tattoo eyeliner and missing lashes (madarosis) and lower eyelid manual expression post-LipiFlow (1st visit), respectively.



Figures 2 and 3: Courtesy of Kambiz Silani, OD.
Conclusion
Age-related meibomian gland dysfunction is a very common condition and may present subclinically, without symptoms, but may also present with symptoms that may affect an individual’s quality of life.
It is important to screen for the signs of ARMGD for each patient and to educate the patient on their diagnosis, as well as explain the treatment options and protocol based on the severity of the condition.
New treatment methods such as Miebo, IPL, and LipiFlow create a new avenue for medical treatment and clinical modalities, and aid in more chronic and advanced cases of ARMGD.
5 key takeaways from the article
- Millions of individuals suffer from MGD
- Age is the primary risk factor for MGD
- Mild cases of ARMGD can be asymptomatic, but may progress to become symptomatic if left untreated
- Some systemic conditions and medications can contribute to or worsen MGD
- MGD can be treated with at-home treatments in early stages, but may require in-office treatment for more advanced cases

