




Residency serves as a time for young surgeons to learn, develop, and hone their craft before practicing independently. It is a crucial stage for every physician as they advance in their career. While there are many ophthalmic surgeries and procedures, we identify five critical ones that every resident should master to function as a competent and comprehensive ophthalmologist in any post-residency setting.
Corneal foreign body removal1
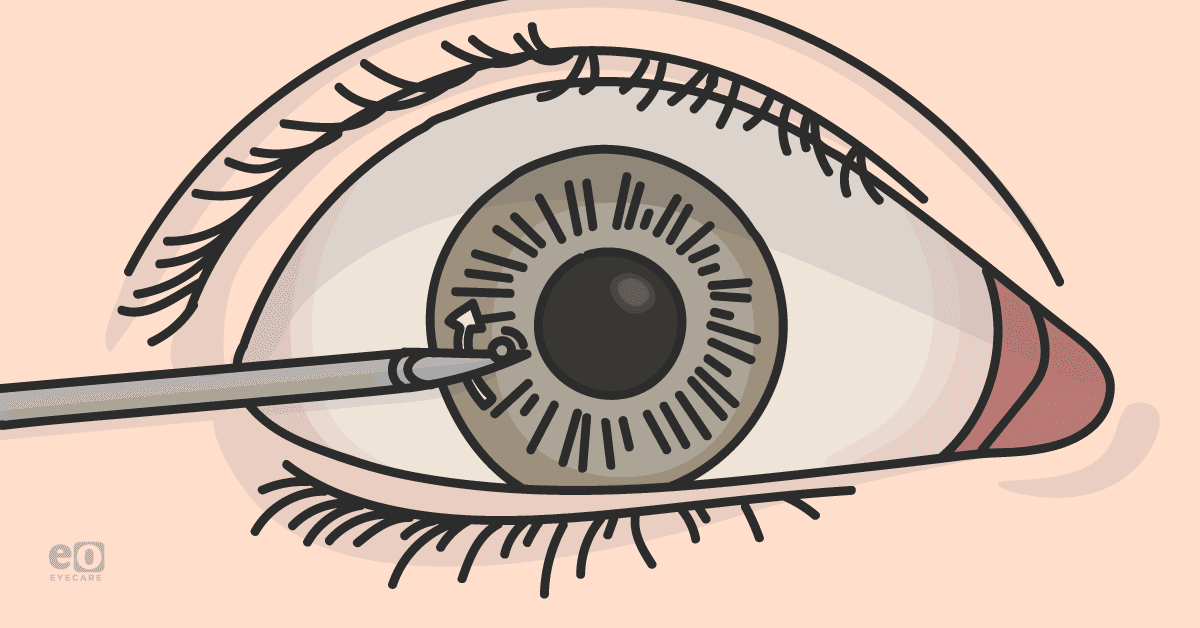
Corneal foreign bodies may lie within the external ocular surface or be embedded deeper within the cornea, potentially causing penetrating injury. Before removal, a thorough history and slit-lamp examination are required to characterize the nature of the foreign body and assess the depth of corneal penetration. Some materials embedded to certain depths may be left alone, while others pose a high infectious risk and should be removed immediately.
Figure 1 illustrates a corneal foreign body.

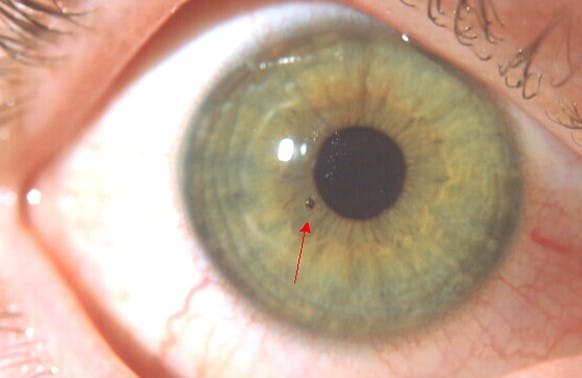
Figure 1: Image courtesy of David Almeida, MD, MBA, PhD
Corneal foreign bodies are essential to address as they may be highly uncomfortable, pose a risk for infection or chemical injury, and may potentiate the risk of perforation. After assessing no penetrating injury, which is done by ensuring Seidel negative fluorescein staining, complete a thorough anterior segment exam.
- If it’s determined that the foreign body is superficial, using a moist cotton tip or lavage may be sufficient for removal.
- If embedded, a needle or pair of fine forceps may be used to gently dislodge and lift the foreign body away from the cornea with an upward force.
The authors have found that bending the bevel of an 18-gauge needle (on the edge of the sterile cap) provides the best tool to remove large foreign bodies or rust rings. The bent, large gauge needle provides the adequate surface area to remove a FB without increasing the risk of perforation if the patient shifts during the procedure. In the specific case of materials leaving rust rings, a rotating burr can be utilized to remove additional affected tissue.
Complications include incomplete foreign body removal, intraocular penetration, endophthalmitis, and retinal detachments. Be sure to thoroughly evaluate the patient’s history and examination to determine whether the foreign body has penetrated the cornea. Complete a full dilated eye exam to rule out posterior segment trauma and involvement further.
Patients should be given post-procedure antibiotics with appropriate follow-up and for trauma with vegetative matter consider adding a fluoroquinolone antibiotic for additional mild antifungal coverage.2

Download the 5 Procedures Cheat Sheet!
This handy guide, with diagrams and images, covers five must-know procedures.

Temporal artery biopsy3,4
Temporal artery biopsy (TAB) is indicated when seeking a definitive diagnosis for giant cell arteritis (GCA). A TAB should be performed after a thorough history, physical, and laboratory workup has been completed, and suspicion for GCA remains high. Still, if clinical suspicion of GCA is high, do not hesitate to initiate systemic immunomodulatory therapy before biopsy to reduce the risk of serious sequelae, including loss of vision.
After identifying the temporal artery and administering local anesthetics, here are the steps involved in performing a TAB:
- Begin by making a skin incision with a 15-blade scalpel.
- Next, bluntly dissect the fascia layer overlying the temporalis muscle, where the temporal artery will be located immediately deep into this fascia.
- Continue dissecting the fascial plane to expose at least three centimeters of the temporal artery.
- Using a needle driver, pass two silk ties, each beneath the proximal and distal ends of the temporal artery.
- Excise the temporal artery by cutting the proximal and distal ends of the vessel between the two sutures placed on either end. Cauterize the arterial stumps that are left behind.
- Then achieve hemostasis, perform wound closure, and dress the wound.
Complications may include wound infection and hematoma formation. Additional complications specific to TAB include facial nerve trauma due to its proximity to the temporal artery and scalp necrosis when insufficient vessel collateralization occurs.
Canthotomy and cantholysis5,6
For the ophthalmology resident, a lateral canthotomy and cantholysis will typically be performed in the setting of orbital compartment syndrome, a true ocular emergency. Orbital compartment syndrome, which is a clinical diagnosis and requires no confirmatory imaging, is a rapid increase of intraocular pressure and can result in permanent vision loss without prompt intervention.
Compartment syndrome is most commonly caused by retrobulbar hemorrhage in high-impact trauma but may also arise secondary to orbital cellulitis, carotid-cavernous fistula, or orbital emphysema, among other entities.
While also performed in controlled settings for eyelid reconstruction, the technique in the emergency setting is intended to be done much faster.
To perform lateral canthotomy and cantholysis:
- Begin by locally anesthetizing the area proximal to the lateral canthus and using blunt-tipped scissors to create a full-thickness cut of the canthus. Optionally, hemostats may be clamped for one minute at the lateral canthus before incision to reduce bleeding.
- Once the amount has been made, use large tooth forceps to grasp the eyelid and expose the lateral canthal tendon with gentle anterior traction.
- Cut the tendon to decompress the globe.
The eyelid should move away from the globe once released by the forceps and note rapid decreases in intraocular pressure upon successful cantholysis.
The most common complication is incomplete cantholysis. Ensuring adequate decompression with close monitoring afterward is warranted. Another common complication is excessive bleeding, given the emergent nature of the procedure and inadequate time to stop or reverse anticoagulation.
Cataract surgery: phacoemulsification and intraocular lens implantation–“divide and conquer”7,8
Cataract surgery is the bread-and-butter procedure for the ophthalmology resident. While the most frequently performed surgery in the United States, this surgery is delicate, complex, and requires tremendous practice. Several variations of technique exist; however, the same general principles guide the ophthalmologist.
Figure 2 demonstrates cataract surgery.

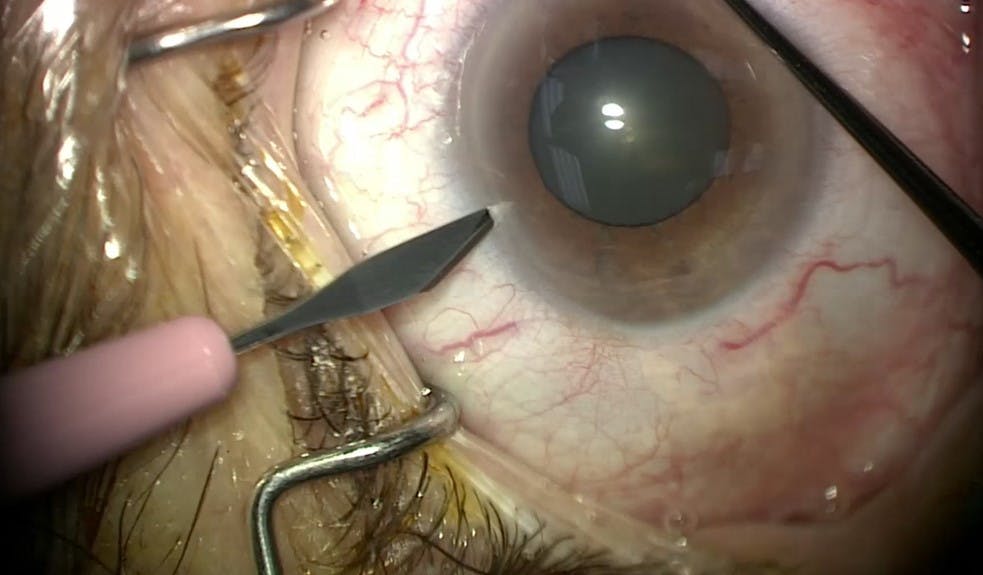
Figure 2: Image courtesy of David Almeida, MD, MBA, PhD
Cataract surgery is so frequently performed as senile cataracts form in every adult patient. However, other indications exist, including juvenile cataract formation in the setting of inborn errors of metabolism or vertically transmitted maternal infections or cases of trauma. With such varied etiologies, planning, timing, and follow-up may vary.
However, in most cases, the ophthalmology resident will perform phacoemulsification with intraocular lens (IOL) implantation in adult patients with senile cataracts. The “divide and conquer” technique, which is the first technique one should master before perfecting more advanced techniques, is described below.
“Divide and conquer” technique
- Performing this cataract surgery begins by dilating the pupil with topical drops of choice. Additional mydriatics may be given intraoperatively once access to the anterior chamber has been achieved.
- Administration of local anesthesia, whether via topical drops or through peri- or retrobulbar blocks, will then be performed. Rarely will general anesthesia be administered, though this is typically reserved for pediatric patients or those with a mental state that would prevent a safe surgery.
- Once adequate anesthesia is achieved, create a paracentesis by passing a side port blade through the cornea at the limbus.
- Through the paracentesis, insert a cannula and fill the anterior chamber with dispersive viscoelastic ensuring not to overfill and cause sudden increases in intraocular pressure.
- Continue injecting the viscoelastic as the cannula is withdrawn from the paracentesis to evacuate air bubbles.
- Following this, create a larger, precise corneal incision that should be large enough to accommodate an intraocular lens (IOL) cartridge. Typically, this second incision is placed about 60 degrees apart from the paracentesis and often in the temporal quadrant, though a superior main incision can also be used.
- The next step is the capsulorhexis, which in most cases is the removal of the anterior lens capsule. In select cases, the posterior lens capsule may also be removed.
Performing capsulorhexis
The capsulorhexis is started centrally puncturing the anterior capsule with a bent needle and then extending the tear circumferentially.
Next:
- With forceps, gently pull the flap with tangential force to reduce the risk of radially developing a tear.
- Once the anterior capsule is removed, perform hydrodissection by placing a hydrodissection cannula beneath the capsulorhexis and injecting a balanced salt solution until the lens moves freely.
- With the cortex exposed, introduce the phaco tip and begin creating a vertical groove through the nucleus.
- Once a track has been carved through the nucleus, submit another instrument through the paracentesis and, using both the second instrument a phaco tip, apply lateral force to crack the nucleus.
- Spin the nucleus 90 degrees perpendicular to the first.
- Crack the nucleus again in this new groove; the result should be four nuclear quadrants.
- With the phaco tip, aspirate the quadrants using ultrasound energy as necessary to break up the nuclear fragments.
- Use the second instrument to guide the fragments to the phaco tip while also protecting the posterior capsule.
- Follow this with removing the epinucleus and stripping the cortex from the capsule in an anterior to posterior fashion.
- Finally polish the posterior capsule to remove any remaining cortical debris. After injecting the anterior chamber and capsular bag with viscoelastic, polish the anterior capsule.
IOL implantation will now be performed.
- Load the IOL into the injector and through the clear corneal incision.
- Place it into the eye and guide it gently into the capsular bag; the IOL will slowly unfurl as it is being placed. The orientation of the IOL haptics should appear to be a backward “S” when appropriately placed. The axis of haptic alignment is especially important when using toric lenses and should align with markers typically made preoperatively.
- Once the IOL is properly positioned, the remaining viscoelastic in the capsular bag and anterior segment should be aspirated.
- Finally, seal the incisions with stromal hydration and refill the eye with a balanced salt solution to ensure normal intraocular pressure.
- Assess for leaks at the incision sites and place a single 10-0 suture or sealant if any concern is.
- Finish by shielding the eye, using a patch if the eye was given more than topical anesthesia.
Intraoperative complications associated with this technique include pain, iris damage, hemorrhage, vitreous loss, wound leaks, posterior capsule rupture, loss of vision, or in the worst-case scenario, a loss of the eye.
Postoperatively, endophthalmitis, lens decentration or dislocation, intraocular pressure spikes, cystoid macular edema, retinal tears and detachments, posterior lens opacification, glaucoma, and failure to achieve desired visual outcomes are among the various complications.
Open globe repair9,10
Open globe ruptures are a surgical emergency requiring prompt attention to prevent herniation of intraocular contents that may result in irreversible vision loss. As soon as other life-threatening issues have been addressed, bringing the patient to the operating room is advised. Exercise great caution to not apply pressure to the eye when working up the patient with a suspected ruptured globe.
Figure 3 illustrates an open globe trauma injury showing uveal prolapse.


Figure 3: Image courtesy of David Almeida, MD, MBA, PhD
Given the severity of the injury, general anesthesia is recommended. If only local anesthesia will be used, ensure a moderate amount of peribulbar anesthesia to not cause too much retrobulbar pressure and further expulsion of intraocular contents.
Open globe repair generally begins with the closure of scleral and corneal wounds. When placing sutures, attempt to bury the knots. Any extruded uveal contents should be ideally placed back into the globe or excised. Any prolapsed vitreous must be removed. A vitrectomy may be necessary to prevent potential retinal detachments if the posterior segment is involved.
Following closure, intravitreal or intracameral antibiotics should be administered as postoperative endophthalmitis is of significant risk, with rates increasing with increasing duration from globe rupture to surgical repair.
Other complications may include retinal detachments, permanent vision loss, sympathetic ophthalmia, and retained foreign bodies. Specific postoperative complications may also result depending on the nature of the retained material.
Thankfully, with the internet, additional materials and resources, including exceptional videos, are abundant. We recommend the Cataract Coach series on Youtube to help develop a cataract surgery skillset and the Wills Eye Manual and Eye Guru to guide you through ophthalmic procedures such as the ones we mentioned above and additional necessary procedures such as anterior chamber paracentesis.
Plan B, C, and beyond
Learning these procedures and surgeries takes time, effort, and repetition of both theoretical and practical steps. Each rep provides a learning experience. Even the complication should be a prime learning experience to have plan B, plan C, and plan D ready in one’s armamentarium for unique surgical situations and complex cases.
Don't forget to download the 5 Procedures for Ophthalmology Residents Cheat Sheet.
References
- Guier CP, Stokkermans TJ. Cornea Foreign Body Removal. 2021 Aug 25. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32119365.
- Murchison, AP. Corneal Abrasions and Foreign Bodies.2022 May. [nternet] Merck Manual Professional Version. https://www.merckmanuals.com/professional/injuries-poisoning/eye-trauma/corneal-abrasions-and-foreign-bodies.
- Chase E, Patel BC, Ramsey ML. Temporal Artery Biopsy. 2022 Jan 21. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 29262071.
- Bowling K, Rait J, Atkinson J, Srinivas G. Temporal artery biopsy in the diagnosis of giant cell arteritis: Does the end justify the means? Ann Med Surg (Lond). 2017 Jun 15;20:1-5. doi: 10.1016/j.amsu.2017.06.020. PMID: 28663795; PMCID: PMC5479941.
- Ballard SR, Enzenauer RW, O'Donnell T, Fleming JC, Risk G, Waite AN. Emergency lateral canthotomy and cantholysis: a simple procedure to preserve vision from sight threatening orbital hemorrhage. J Spec Oper Med. 2009 Summer;9(3):26-32. PMID: 19739474.
- Desai NM, Shah SU. Lateral Orbital Canthotomy. 2021 Oct 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32491408.
- Carifi G, Miller MH, Pitsas C, Zygoura V, Deshmukh RR, Kopsachilis N, Maurino V. Complications and outcomes of phacoemulsification cataract surgery complicated by anterior capsule tear. Am J Ophthalmol. 2015 Mar;159(3):463-9. doi: 10.1016/j.ajo.2014.11.027. Epub 2014 Nov 26. PMID: 25461300.
- Hausheer, JR. Basic Techniques of Ophthalmic Surgery. 3rd ed. American Academy of Ophthalmology; 2019.
- Blair K, Alhadi SA, Czyz CN. Globe Rupture. 2022 Jan 31. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 31869101.
- Jordan DR, Dutton J. The Ruptured Globe, Sympathetic Ophthalmia, and the 14-Day Rule. Ophthalmic Plast Reconstr Surg. 2021 Sep 28. doi: 10.1097/IOP.0000000000002068. Epub ahead of print. PMID: 34593714.
