



Dry eye disease (DED) affects more than 18 million US adults, although an estimated 38 million may experience related symptoms.1-3 As one of the most common ocular conditions presenting in clinical practice,4 DED is a multifactorial condition that results in tear film dysfunction that can lead to a vicious cycle of tear hyperosmolarity, cellular apoptosis, inflammation, and injury.5
While there have been major strides in dry eye diagnostic technology—ranging from noninvasive tear breakup time to lipid layer interferometry—one tool has emerged as indispensable: meibography. Yet even as meibography becomes more mainstream, a surprising and persistent oversight remains: most clinicians still only image the glands of the lower lids.
This trend is often driven by workflow challenges rather than clinical rationale, as upper lid eversion is more technically challenging than lower lid eversion. Additionally, many technicians, who are often tasked with obtaining meibography images, may not be as experienced or comfortable manipulating patients' upper eyelids as the doctor.
But skipping upper gland evaluation means you are literally only seeing half the story. As both clinical practice experience and emerging evidence make clear, upper eyelid meibography is essential for accurate diagnosis, early detection, and comprehensive management of DED and meibomian gland dysfunction (MGD).6
Why the meibomian glands matter
Traditionally, dry eye has been separated into three main categories: aqueous-deficient, evaporative, or combined DED, as many cases display elements of both.5 Aqueous-deficient dry eye is caused by a reduction in aqueous production by the lacrimal glands, leading to a low tear volume.
Meanwhile, evaporative dry eye, in which the tear film evaporates prematurely, is considered a major cause of DED and is primarily attributed to MGD, with an estimated prevalence of 51 to 86% among those with DED.5,7-10
Importantly, the TFOS DEWS III report recognizes that evaporative dry eye occurs in at least ~67% of patients with DED and has multiple etiologies, including lid and ocular surface abnormalities.5 Consequently, MGD often plays a central role in the pathophysiology of DED. Of note, it may occur independently or be secondary to the condition itself.
Changes to meibum quality or production—whether from inflammation, obstruction, or gland dropout—create a damaging cycle characterized by altered lipid composition, increased meibum viscosity, bacterial overgrowth, and compromised tear film stability, all of which perpetuate the dry eye cycle and its symptoms.11-13
The importance of meibomian gland assessment
Growing evidence suggests that clinicians may be underdiagnosing, inadequately assessing, or delaying the diagnosis of MGD, as asymptomatic disease is remarkably common.14 Many patients show extensive meibomian gland loss on meibography despite minimal or absent symptoms.14 In fact, asymptomatic MGD occurs more frequently than symptomatic disease.15
However, traditional clinical testing frequently fails to detect early-stage MGD because the body's compensatory mechanisms, particularly increased aqueous tear production and meibomian gland dilation, to maintain tear film stability.16 However, these mechanisms effectively mask the underlying pathology, making early detection difficult with traditional assessments.16
Therefore, direct evaluation of the meibomian glands is vital to early detection of MGD, as changes to gland morphology represent some of the first signs of the disease.6
Performing a thorough MGD evaluation
MGD evaluation starts with assessing gland structure and function. The meibomian gland orifices should be evaluated for signs of obstruction or inflammation.17 Additionally, other eyelid findings such as lash collarettes or telangiectatic vessels should be noted, as they are associated with Demodex blepharitis and ocular rosacea, respectively, and can cause or exacerbate MGD.17
Below are key steps to performing a comprehensive MGD evaluation:
- Direct visualization of the glands is vital and can be performed either manually or via meibography, however each method begins with eyelid eversion.
- Manual evaluation of the meibomian glands can be performed by everting the eyelid and then placing a transilluminator against the external aspect of the lid, which allows for visualization of gross gland structure (Figure 1).18-20
- Infrared meibography (Figure 2) can be used to image the glands in greater detail as it facilitates identification of structural abnormalities, such as gland dropout, tortuosity, and atrophy.6
Figure 1: Meibomian gland transillumination in a patient with MGD.


Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO.
Although meibography has shown to be essential in identifying early MGD and has started to gain wider implementation, it still ranked seventh in popularity among diagnostic tests used in a survey of 215 optometrists.21 The survey found that about 4% always use meibography, 28% use it only in dry eye patients or suspects, and 68% never use it,21 illustrating a gap in the current DED and MGD diagnostic landscape.
When assessing structural changes to the glands, it is essential to look beyond gland dropout. Early-stage disease is often characterized by gland thickening and tortuosity, with gland dropout typically occurring later in the disease process.6,16,22 Therefore, diagnostic approaches that focus primarily on gland dropout to classify and grade the severity of MGD may lead to delayed diagnosis.22
Figure 2: Meibography of upper and lower eyelids in a patient with MGD.

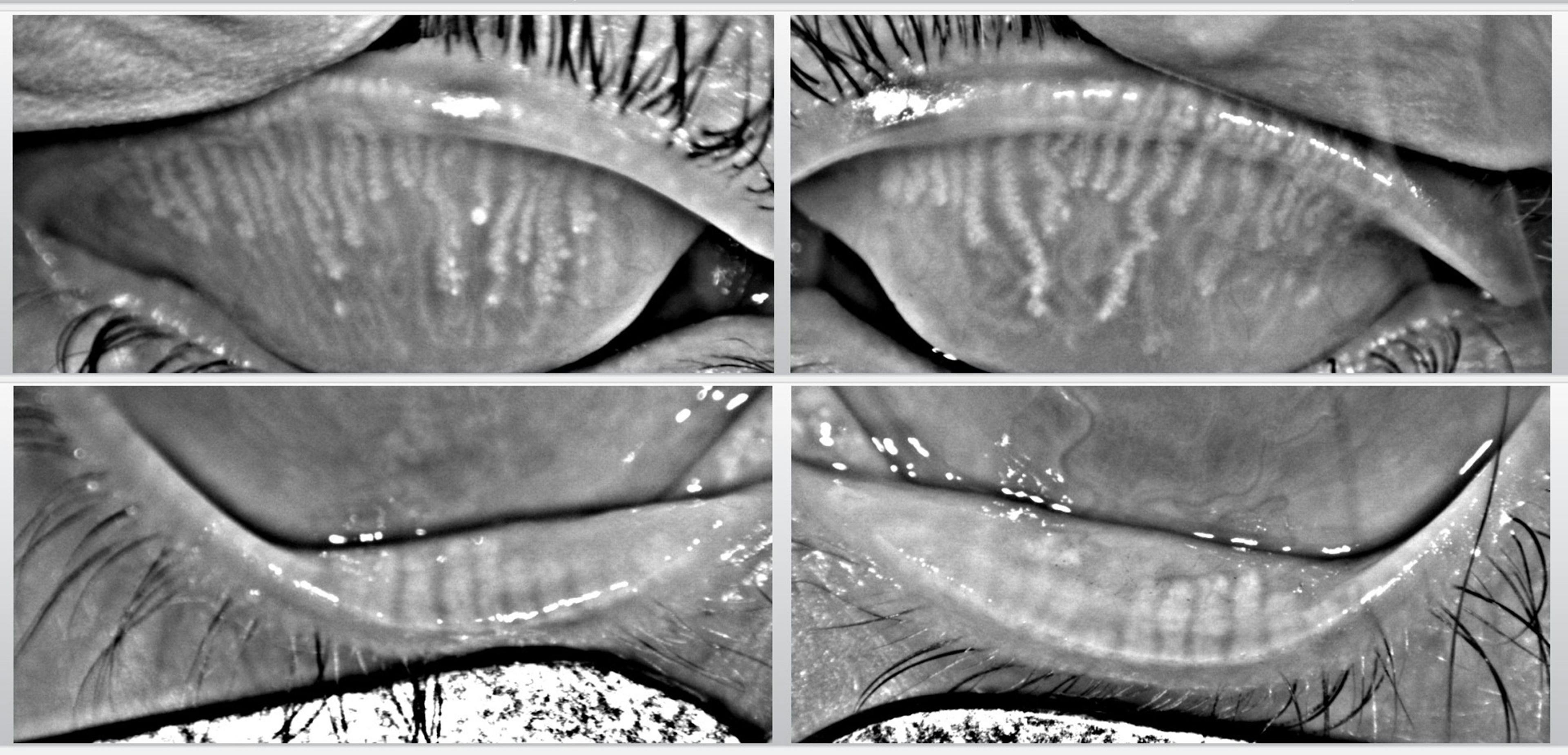
Figure 2: Courtesy of Cory Lappin, OD, MS, FAAO.
Assessing meibomian gland function
Gland function can be assessed through diagnostic gland expression by applying gentle, sustained digital pressure to the eyelid to determine the number of meibomian glands that remain active or expressible.16,23
The clarity of expressed meibum shows meibum quality and distinguishes between healthy glands (which produce clear, easily expressed secretions) and abnormal glands (which produce turbid, thickened oil or opaque, toothpaste-like secretions, such as in Figure 3).16
The Meibomian Gland Evaluator (Johnson & Johnson) can be a helpful tool when assessing meibomian gland function and meibum quality, as the device is calibrated to apply pressure that is equivalent to that of a deliberate physiologic blink, providing a consistent method to evaluate meibomian gland expressibility.42
Additionally, lipid layer interferometry can provide an objective measurement of the tear film’s lipid layer thickness (LLT). A reduction in LLT has been associated with MGD,24,25 and may therefore act as a proxy for meibum production and meibomian gland function.
Figure 3: Toothpaste-like meibum secretion in a patient with MGD.


Figure 3: Courtesy of Cory Lappin, OD, MS, FAAO.
Why upper eyelid meibomian gland evaluation is essential
The common trend of failing to routinely assess the meibomian glands of the upper eyelids in clinical DED and MGD evaluations was spotlighted in a 2025 review by Preeya K. Gupta, MD and Paul Karpecki, OD.6 This review highlighted that the upper glands typically show earlier morphologic changes, including gland tortuosity, dropout, and thickening when compared to the lower glands.6
The upper glands are also longer and slimmer, resulting in greater susceptibility to early structural changes that may precede symptomatic disease, which supports the view that upper lid evaluation is necessary for early disease detection.6
It is also important to note that the structure of the lower glands and upper glands does not always directly correlate, so observation of the lower glands alone cannot be used to make assumptions about the structural status of the upper glands.6
Additionally, the morphological appearance of the upper glands appears to provide critical insight for key patient populations:6
- Contact lens wearers: Increased meibomian gland tortuosity in the upper lid significantly increases the risk of contact lens dropout, with a 1.74x greater risk.26,27
- Worsening gland plugging in the upper lids also increases the risk of contact lens dropout, with up to nearly a 5x greater risk depending on severity.26 Additionally, contact lens wearers with worsening upper lid meibum quality are more likely to discontinue lens use due to discomfort.26,27
- Post-cataract surgery patients: Pre-operative meibomian gland loss of the upper lid significantly predicts post-operative dry eye symptoms, whereas lower lid gland loss may not correlate.28
- Patients with Sjögren's syndrome (SS): Upper eyelid gland dropout is significantly greater in patients with SS compared to non-SS patients with dry eye.29,30
- Morphological changes in the upper lid likely contribute to differences in ocular signs and symptoms between SS and non-SS patients.6 These changes may be considered critical for diagnostic purposes.6
- Thyroid eye disease (TED): Meibomian gland loss of the upper lids is greater in patients with TED than in those with traditional DED.31 This finding may result from factors observed in patients with TED, including incomplete blinking, proptosis, and eyelid retraction.31
- Patients with TED also have upper glands displaying higher degrees of gland loss with greater central gland dropout than other patients with DED, which correlates with increased ocular surface inflammation and oxidative stress.32 Therefore, assessment of both upper and lower glands can assist in accurately diagnosing TED-related dry eye.6
- Postmenopausal women with primary acquired nasolacrimal duct obstruction (PANDO): Postmenopausal women with PANDO displayed a greater degree of gland loss in the upper lid along with worse meibum quality compared to the lower glands.33
The upper gland changes observed in these groups demonstrate the vital importance of upper eyelid assessment as part of a comprehensive evaluation of DED and MGD, as its omission can result in missing clinically relevant pathology.
Top tools for meibomian gland evaluation
Modern meibomian gland evaluation increasingly incorporates specialized mechanical tools and artificial intelligence to enhance visualization, consistency, and longitudinal assessment of gland health.
Eyelid everters
Eyelid eversion is necessary for visualizing the meibomian glands whether performed manually with a transilluminator or via meibography, but practicing clinicians and technicians recognize that it can be more challenging to evert the upper eyelids compared to the lowers.34,35 However, the key to obtaining high-quality meibography images is complete lid eversion.
Fortunately, tools now exist to minimize or eliminate the challenges associated with lid eversion. Devices such as the Epstein Lid Everter (Medirix LLC), LidVue Eyelid Everter (VisuScience Meditech), and the Meivertor Everter (Mazado Inc.) make performing lid eversion more efficient, consistent, and successful.
The curved design of the Epstein Lid Everter better fits the contour of the lids, allowing for easier placement and eversion.36 The LidVue Eyelid Everter can help with lower lid eversion by improving handling and patient comfort with its smooth edges.37
The Meivertor was designed to assist in everting both upper and lower lids with a single hand, keeping the other hand free to obtain imaging, all while maintaining patient hygiene and comfort via single-use, disposable silicone tips.38
From a diagnostic standpoint, an important function of meibography is to track gland changes over time, but the appearance of the glands is highly reliant upon consistent lid eversions so comparisons can be made uniformly across images. Therefore, consistent lid eversion is essential because variations in technique significantly alter the meibography image and perceived gland structure.
Tip: The use of lid everters can make lid eversion more uniform resulting in more consistent imaging—and therefore provide more reliable tracking of disease progression.
Artificial intelligence (AI)
Deep learning approaches have shown great promise in automatic image segmentation of meibomian glands for a complete assessment of their morphology. This technology may improve clinicians’ understanding of MGD and enhance diagnostic accuracy.39-41
Takeaways
When conducting a comprehensive dry eye evaluation, meibography should include imaging of both the upper and lower meibomian glands—otherwise, you’re only getting half the story. Meibomian gland dysfunction is now recognized as a leading driver of dry eye disease, particularly in today’s screen-dependent environment.
As a result, diagnostic imaging has become essential to understanding gland structure and identifying early changes. Yet many clinicians still limit their assessment to the lower eyelid glands, often because everting the upper lid can be more technically challenging.
Despite these challenges, evaluating the glands of both eyelids is critical. Early structural changes in MGD frequently appear in the upper glands, and upper lid findings can correlate with a range of clinical conditions—including contact lens discomfort and dropout, post-cataract surgery dry eye, Sjögren’s syndrome, thyroid eye disease, and postmenopausal patients with PANDO.6,33
Fortunately, several tools now help facilitate lid eversion, making upper lid imaging more accessible for both clinicians and technicians.
Bottom line: Comprehensive meibomian gland assessment is essential for early detection and timely intervention. Relying solely on lower lid imaging risks overlooking meaningful early gland changes.6 Therefore, when performing a complete DED and MGD evaluation, imaging the glands of both the upper and lower lids should be considered the standard of care.
