Human nature dictates that, often, we learn more from our mistakes than we do from our successes. This is applicable in the realm of surgery as well.
Many times, it is the procedure that does not meet the expectations of either surgeon or patient that offers the most lasting lessons.
In this video from Interventional Mindset, Gary Wörtz, MD, shares an
arcuate incision case from his early career with colleagues Neda Shamie, MD, and Preeya K Gupta, MD, to offer insight into the decision-making process and pearls for success.
Interventional Mindset is an educational series that gives eye physicians the needed knowledge, edge, and confidence in mastering new technology to grow their practices and provide the highest level of patient care. Our focus is to reduce frustrations associated with adopting new technology by building confidence in your skills to drive transformation.
Browse through our videos on a variety of topics within cataract and refractive surgery, glaucoma, and ocular surface disease to learn practical insights into adopting a variety of new surgical techniques and technology.
The case in question
In 2015, shortly after Dr. Wörtz began practicing, he was faced with the case discussed in this video. For background, in residency, he did not have the opportunity to perform a great number of corneal arcuate or
limbal relaxing incisions (LRIs).
Also, at this time, toric lenses were not as advanced as they are now presently, leading to more frequent complications. To add an extra wrinkle to the mix,
pre-operative topography was not standard in all clinics.
A 70-year-old white male presents for a cataract surgery evaluation with the following criteria:
- Wants refractive cataract surgery
- Has moderate astigmatism: 1.42D X 11 OD and 1.80D X 164 OS
- Desires distance correction for reduced dependency on glasses
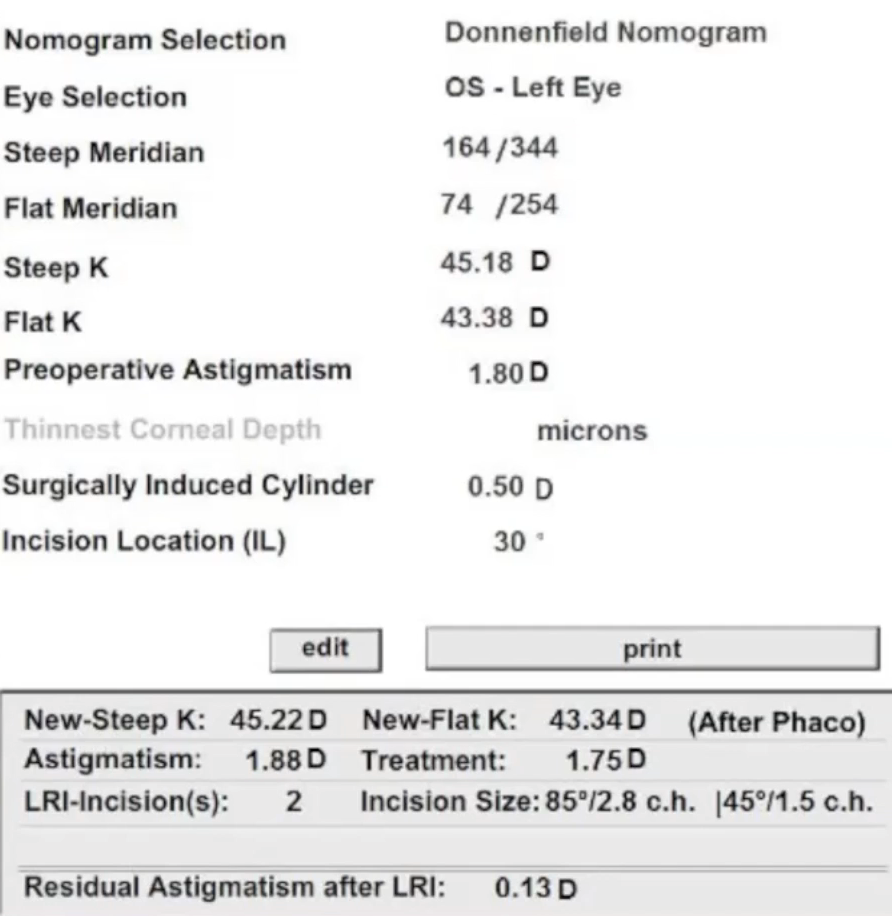
Figure 1 displays the initial findings from the case.
Figure 1: Courtesy of Gary Wörtz, MD.
Treatment with femtolaser arcuate incisions
Basing his decision on the Donnenfeld nomogram, Dr. Wörtz opted to perform a femtolaser arcuate incision to correct the astigmatism.
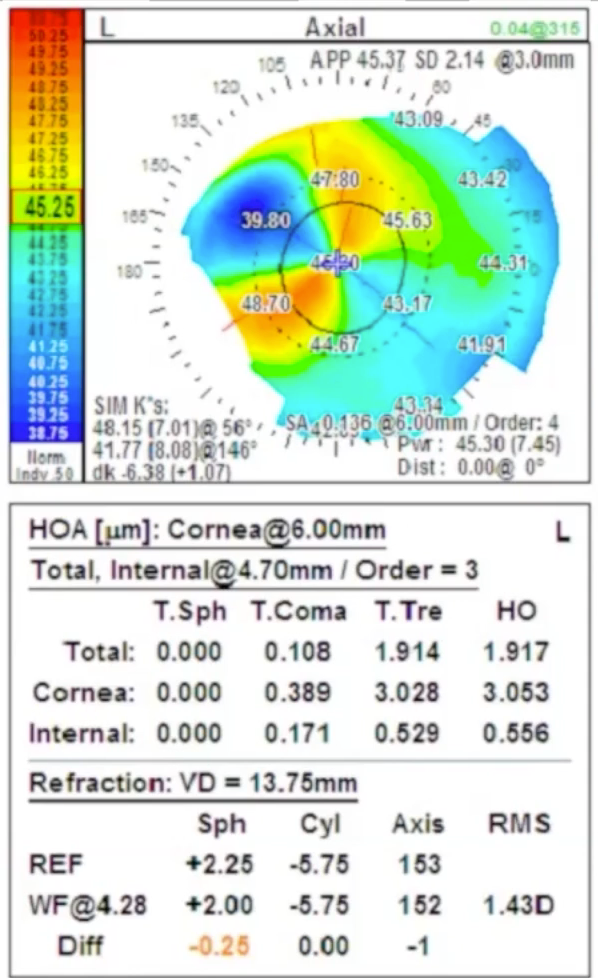
Figure 2: Courtesy of Gary Wörtz, MD.
Based on these findings, Dr. Wörtz decided to proceed with a pair of large arcuate incisions.
Of note, he has since found a single arc to be more effective. Dr. Gupta concurs that single arcs are preferable for against-the-rule (ATR) astigmatism to maintain wound integrity.
Following surgery, on Day 1, the patient had a complete flip of their axis, as seen in Figure 3 below.
Figure 3: Courtesy of Gary Wörtz, MD.
At this point, Dr. Wörtz's options were:
- Wait
- Excimer laser ablation
- Top-guided photorefractive keratectomy (PRK)
- Exchange the monofocal intraocular lens (IOL) for a toric one
- Suture the arcs
Treatment outcome and follow-up
Dr. Wörtz chose the final option and decided to suture the arc, which resulted in a reasonable reduction in the astigmatism. This, unfortunately, did not last. At approximately 6 months post-suture, the patient still had 4.75D of astigmatism.
To correct this, Dr. Wörtz exchanged the monofocal lens with the ZCT600 TECNIS toric IOL (
Johnson & Johnson Vision), which was the highest power toric available at the time.
Acknowledging that
toric lenses in 2015 were not nearly as reliable as they are today and that LRIs were the more common treatment at the time, both Dr. Shamie and Dr. Gupta understood Dr. Wörtz’s inclination to elect LRI for this case. Fortunately, today’s toric lenses are vastly improved with a more favorable safety profile.
Hindsight is 20/20
This case was instrumental in forming Dr. Wörtz’s approach to toric lenses. Looking at the case retrospectively, the surgeons share their opinions on how this patient would be treated today. First, they acknowledge the importance of attaining pre-operative topography whenever surgically correcting astigmatism to reveal nonuniform steepening and patterns.
For
moderate corneal astigmatism, Dr. Shamie’s approach for a patient with 0.75D against the rule or 1.00D with the rule (WTR) is to utilize a toric lens. If the individual’s astigmatism is less, she feels comfortable opting for an LRI.
Dr. Gupta always errs on the side of caution by choosing the procedure that will most reliably correct astigmatism and, along with a thorough exam and appropriate diagnostic tests and measurements, looks to the
Barrett Toric Calculator as an adjunct tool.
Parameters for arcuate incisions
Initially, Dr. Wörtz admits he was a “cowboy” when it came to arc length, going as high as 60°. However, now, taking into consideration the risk of iatrogenic corneal ectasia and
neurotrophic keratopathy (NK), both he and Dr. Gupta agree that a 50° arc length is the maximum.
Dr. Shamie is slightly more conservative within her practice and prefers not to go above 30° to 40°, although she notes that with select patients, she has gone as high as 45°.
When determining the arcuate length (whether aggressive or conservative), an important watch out to keep in mind would be to avoid corneal decompensation. In either case, according to Dr. Gupta, “The bigger the incision, the less stability.” Dr. Shamie added that one of the dangers in larger arcs is the loss of tissue that occurs when the epithelium migrates in the crevice and the edges “melt.”
For femto arcuate decision-making, Dr. Gupta stresses the value of utilizing an LRI calculator.1 In 2020, Dr. Gupta and Dr. Wörtz founded Arcuate Innovations with its revolutionary Wörtz-Gupta Formula and associated LRI Calculator, which helps surgeons obtain precise, individualized measurements and placement for LRI.
A note on nomograms
It must be stated that the DONO (Donnenfeld) and NAPA (Nichamin) nomograms were developed to guide manually performed LRIs, not those performed using
femtosecond laser surgery.
Manual blades create very different incisions with potentially variable depths compared to the ablation of tissue with a femtosecond laser, which creates the arcuate; consequently, these incisions behave differently.
Insights into intrastromal arcs
With intrastromal arcuate incisions, since the corneal integrity is not impacted, an 80° arcuate is deemed acceptable; however, Dr. Gupta cautions that there has not been enough evidence showing a predictable effect.
Dr. Wörtz quoted Jim Loden, MD, who had warned that intrastromal arcs were often a “gift that keeps on giving,” causing a destabilized cornea during follow-up femto
laser in situ keratomileusis (LASIK) procedures.
Patience is a virtue
Through her practice, Dr. Shamie has found that for suturing to have a lasting effect, it is imperative to do two things. First, scoop out the epithelium to get raw stromal edges that will bond and thicken, forming a strong, near fibrosis. Secondly, leave the sutures in longer than you would anticipate.
Amniotic membranes can be helpful in this instance for tissue support.
Dr. Gupta also believes in “the power of the suture” and draws a parallel to a full-thickness corneal transplant patient who returns 6 months post-surgery with 20/40 uncorrected acuity only to have it drop to 20/200 once a stitch is removed. She suggests the time frame can be 6 to even 9 months.
Practical pearls for surgical success
Dr. Shamie offers three pearls that apply to not only LRI but all surgical procedures.
Pearl 1: Seek out and take advantage of mentoring opportunities.
When multifocal toric lenses first became available, none of the colleagues in Dr. Shamie’s practice were implanting
advanced technology lenses.
However, she knew these were something she wanted to add to her armamentarium, so she took it upon herself to reach out to an Alcon representative and later Samuel Masket, MD, who was one of the most experienced surgeons with torics at the time.
In the spirit of the interventional mindset, she flew to Los Angeles and spent 2 days learning the technique, asking questions, and taking notes. She returned home to perform the first multifocal toric implant in the Northwest.
Dr. Shamie urges ophthalmologists to take advantage of all opportunities to be mentored, whether it be in-person one-on-one, through virtual education, by utilizing online
American Academy of Ophthalmology (AAO) resources, or at conferences and classes.
Pearl 2: Educate yourself on the available technology and techniques prior to presenting it to patients.
Be fully equipped with the necessary knowledge and skills before introducing an option to a patient. This requires diligence in maintaining an ongoing awareness of the latest breakthroughs in the field and a commitment to continuing education.
Pearl 3: Commit to remaining with patients from surgery to satisfaction.
One of the biggest takeaways for Dr. Shamie from this case was Dr. Wörtz’s unwavering dedication to stay the course and see the case through to the end.
She emphasizes how important it is for doctors to offer patients the reassurance that they will remain with them throughout their entire journey and will continue to seek solutions until they are satisfied or have achieved the best outcome possible.
Final thoughts
In a nutshell, Dr. Shamie feels that to serve their patients in 2023 adequately, all
cataract surgeons should be treating astigmatism or taking the steps and receiving the training that will allow them to do so.
Dr. Wörtz goes a step further, saying that not only should ophthalmologists be actively adding “skills to their toolbelt,” but should be encouraging colleagues to do the same to address astigmatism surgically.
Dr. Gupta adds that the joy of ophthalmology is the ever-advancing technology and the multitude of tools that surgeons have at their fingertips. She encourages surgeons to take full advantage of the devices/techniques as well as the expertise of those who are more experienced and can guide the early journey into new procedures and surgical success.
Disclaimer: The Wörtz-Gupta Formula (Patent Pending) femtosecond laser arcuate incision calculator is meant to serve as an adjunct tool to assist physicians in the correction of astigmatism in conjunction with the intraocular lens (IOL) placement.
The information contained herein is derived from the work and nomogram(s) of Gary Wörtz, MD, and Preeya Gupta, MD. The medical opinions and views expressed in the Calculator are those of Drs. Wörtz and Gupta and not those of any manufacturer of femtosecond lasers.