


Effective management of astigmatism is essential to satisfy refractive cataract surgery patients. These seven steps will improve results when implanting a toric monofocal or a toric presbyopia-correcting intraocular lens (IOL).
1. Educate the patient.
Astigmatism doesn’t need to be tricky to explain to patients. Consider using digital patient education programs such as Rendia or TouchMD to educate patients about astigmatism and how it affects their vision.
Using corneal illustrations to show the difference between a basketball or spherical shape vs. a football or toric shape usually makes sense to patients. It is important that they understand that ignoring astigmatism will make vision after surgery out of focus.
Make a clear recommendation and set expectations for what each choice you are offering the patient entails. I find it most effective to offer an outcomes-based package rather than ask the patient to choose a specific technology.
For example, my astigmatism management package is described as “Distance or driving vision without glasses” and includes whatever it takes for me to achieve that goal, including pre-operative testing and planning, use of the femtosecond laser or intra-operative aberrometry, a toric IOL, and/or arcuate incisions.
2. Optimize the ocular surface.
Ocular surface disease (OSD) can alter keratometry values and lead to an incorrect toric IOL power or axis, so it is very important to evaluate the corneal surface and tear film.
If needed, treat with a topical steroid, topical immunomodulator (i.e., lifitegrast, cyclosporine), and/or artificial tears, plus treatment of meibomian gland dysfunction if present, and re-evaluate after 1 month, before obtaining pre-operative measurements.
Personally, I like the new topography-based tear breakup testing available with iTrace Prime (Tracey Technologies). In just 10 seconds, the device provides a tear film quality score that I use to determine if I need to treat OSD prior to biometry measurement.
3. Obtain multiple measurements.
It is simply not sufficient to rely on a single reading for the calculation of refractive IOLs. At a minimum, surgeons should consult two independent measurements of astigmatism pre-operatively, such as a topographer and biometer.
I use the IOLMaster 700 (Carl Zeiss Meditec), iTrace, and Aladdin (Topcon Healthcare). For toric IOLs and a precise total corneal astigmatism (TCA) value, the Cassini Ambient (Cassini Technologies) is awesome.
Consistency in measurements is key, so if you have two or three measurements but the Ks are inconsistent, you need to repeat the measurements or determine why they don’t match, as seen in the image below.
The iTrace topography (left), in Figure 1, accurately shows more than 3 diopters (D) of anterior corneal astigmatism, whereas the Cassini TCA, which includes measured posterior power, shows more than a diopter less, significantly changing the power of the toric IOL chosen for surgery.
Figure 1 features two pre-operative measurements of corneal topography from the iTrace and Cassini TCA devices.

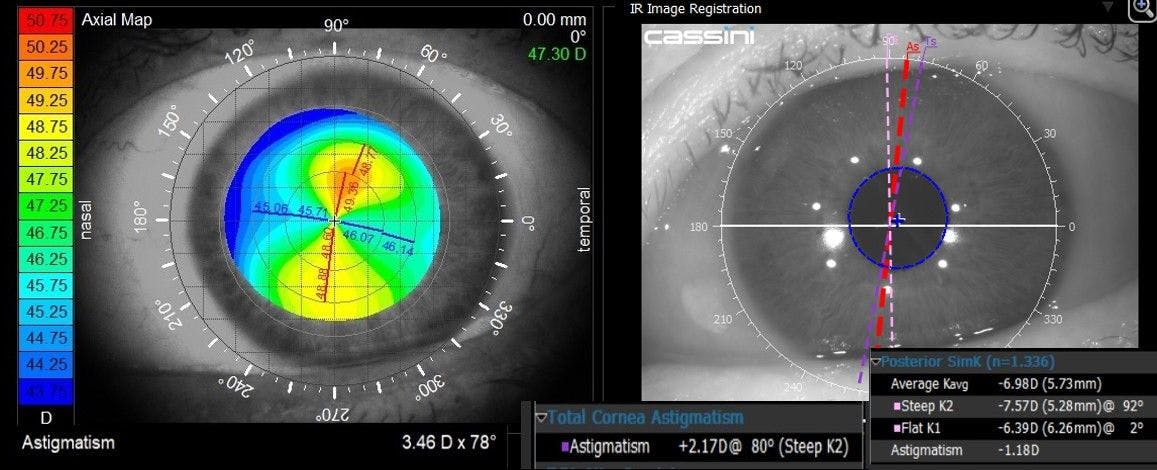
Figure 1: Courtesy of Jared R. Younger, MD, MPH.
4. Remember the back.
Know whether your measurements incorporate posterior corneal astigmatism or if you need to make adjustments to do so. Older IOLMaster devices, along with most biometers and topographers, don’t provide any information about the posterior cornea so if you are using those, you need to check the box on your online calculator to incorporate estimated posterior astigmatism.
Conversely, don’t check that box if you are using more advanced diagnostic tools like Cassini or Pentacam (Oculus) that actually do measure the posterior cornea. Knowing the “total or real” corneal astigmatism is important because this lets you plan accurately for arcuate incisions or toric IOL powers and avoid under- or overcorrection in your refractive results.
5. Mark carefully.
Manual marking can be effective, but I prefer to create femtosecond laser marks with my CATALYS laser (Johnson & Johnson Vision). Because they rely on pre-operative iris registration scans for accuracy, the laser marks are about five times more accurate than manual ink marks.
They eliminate one or more steps in manual marking, won’t fade or run, and make it easier to confirm alignment accuracy intra-operatively and post-operatively.
6. Choose a high-quality toric lens.
We are fortunate in that the toric IOLs on the Acrysof (Alcon), TECNIS (Johnson & Johnson Vision), and enVista (Bausch + Lomb) platforms are all rotationally quite stable.1,2 But it is still important to choose a lens that is well suited to the patient.
A recent patient, a 60-year-old woman with a history of myopic laser in situ keratomileusis (LASIK), has enjoyed spectacle independence prior to presbyopia, but had become slightly hyperopic and more astigmatic with age. She was now unhappily wearing progressive spectacles nearly all the time.
I implanted the Eyhance Toric IOLs (Johnson & Johnson Vision) to offset the positive spherical aberration (SA) of the post-myopic-LASIK cornea, while also providing a slightly broader landing zone for the more challenging post-refractive IOL calculation.
This enhanced monofocal IOL provides the majority of patients with a slightly extended depth of focus while ensuring excellent distance acuity.2
7. Check accuracy post-op.
On post-op day 1, when the pupil is still mildly dilated, I like to confirm that the lens marks are aligned with the corneal marks I made with the laser in a quick check at the slit lamp. If a post-operative manifest refraction is not as good as we would expect it to be, my technicians are empowered to run the iTrace Toric Check.
In 30 seconds through an undilated pupil, it compares the corneal astigmatism to the internal astigmatism power and axis of the lens. When considering a rotation or exchange, tools such as AstigmatismFix.com or the iTrace provide valuable guidance on the degrees and direction of the ideal rotation.
In Figure 2, precise laser marks are shown aligned with IOL axis dots.

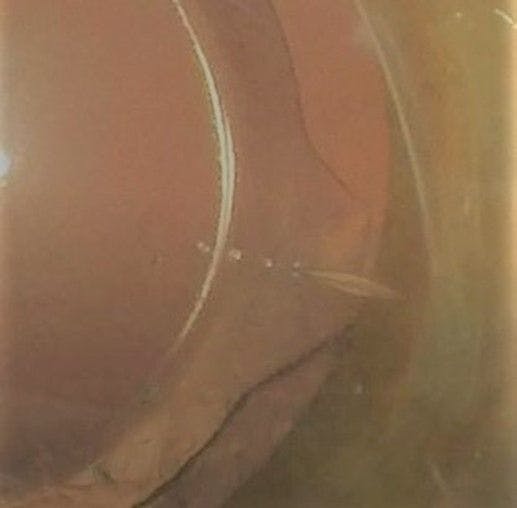
Figure 2: Courtesy of Jared R. Younger, MD, MPH.
Final thoughts
Astigmatism management with toric IOLs and laser arcuate incisions make up most of the cataract surgery procedures in my practice.
Patients who are not good candidates for a presbyopia-correcting IOL or who cannot afford the cost of one still greatly value the ability to see at distance without glasses with a monofocal toric IOL. By managing astigmatism appropriately, we can deliver on that promise.
Disclosure: Jared Younger, MD, MPH, is a consultant for Johnson & Johnson Vision and Cassini Technologies.
