



A 51-year-old male was referred to the eye clinic for a diabetic ocular exam. He was diagnosed with diabetes 1 month ago and promptly started on metformin 500mg BID. His A1C was 7.9% and his morning fast blood glucose ranged 150-180mg/dl. His medical history was otherwise unremarkable. He reported good distance vision but mild near blur which resolved with his over-the-counter reading glasses.
His best corrected visual acuity was 20/20-2 OD, OS for distance and near with a small astigmatic prescription. Externals, IOP, and anterior segment were unremarkable. He had large cupping, 0.7 OD and 0.8 OS. The macula was unremarkable on first examination but after a second assessment, I was able to visualize two pinpoint dark foveal disruptions in the right eye and one in the left eye.
If the visual acuity wasn’t slightly reduced, I would have probably considered this to be normal variation of the foveal pigments. The remainder of the dilated examination was unremarkable.
In Figure 1, fundus photography reveals difficult to visualize, isolated focal hyperpigmented foveal lesions in each eye.

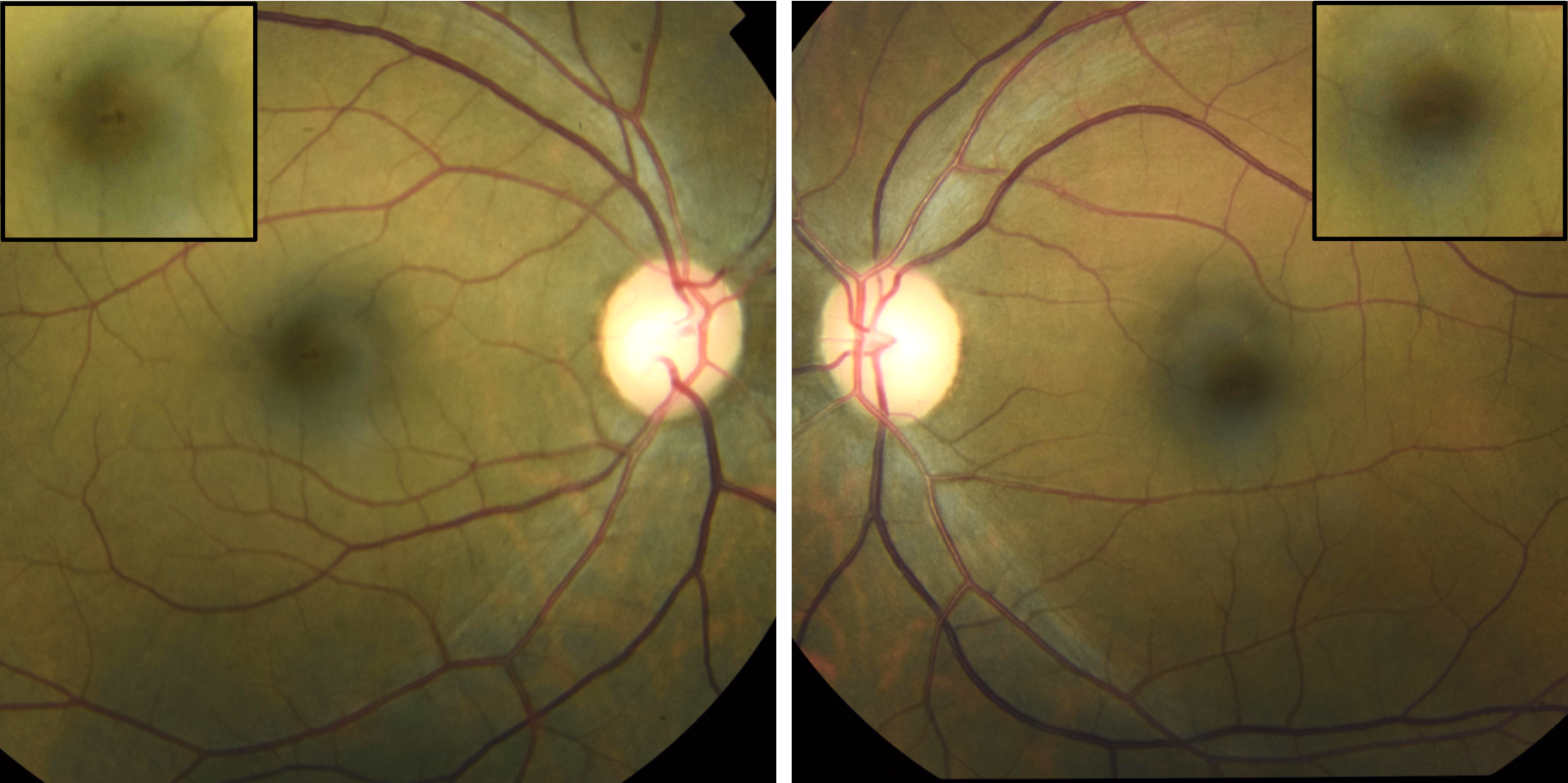
Figure 1
Considering the mildly reduced vision and the foveal lesions, I ordered macular OCT imaging. My standard OCT protocol for unknown macular lesions is a macular cube scan and a HD 5-line raster of each eye. The macular cube scan provides volumetric quantifiable data while the HD 5-line raster scan provides high resolution imaging of the retinal anatomy. OCT imaging of the optic nerve head was also completed as part of a glaucoma suspect evaluation.
Two small adjacent disruptions of the ellipsoid zone and the interdigitation zone were noted in the fovea of the right eye. A single similar lesion was noted in the left eye. The presence of two focal lesions in the right eye and one in the left eye was consistent with the funduscopic exam. No inner retinal disease or vitreomacular traction was appreciated. The optic nerve head OCT scan was essentially unremarkable, with mild scattered borderline defects on the deviation map only.
In Figure 2, focal foveal outer retinal and RPE degeneration is noted in each eye with OCT. Borderline macular thinning is noted on the retinal thickness map.

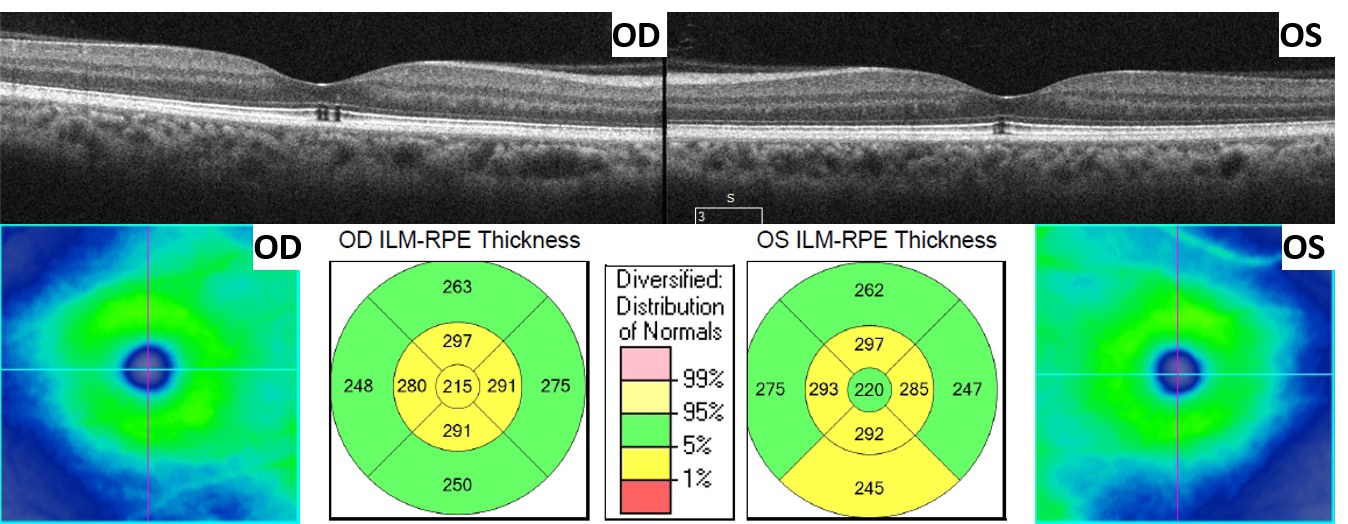
Figure 2
After acquiring the OCT images, I went back to the patient to perform a more guided history. In isolation, the OCT findings were consistent with solar retinopathy but the patient denied any sungazing, eclipse viewing, laser exposure, or welding. The patient denied any recreational drug use or alcohol abuse that may have led to forgetfulness of the aforementioned activities. He denied color vision issues, metamorphopsia, blur, or any history of acute vision loss.
Due to the discordance between the patient’s history and the OCT findings, I ordered a 10-2 visual field to ensure that there was no extrafoveal functional loss. Macular visual field testing with the 10-2 protocol and more peripheral 30-2 testing were essentially full in both eyes. Color vision testing with Ishihara plates were full in each eye.
As seen in Figure 3, visual field testing with the 10-2 macular protocol is unremarkable in both eyes. The small foveal defects noted with OCT and funduscopy are not appreciated with visual field testing.


Figure 3
Solar retinopathy
Solar retinopathy is a specific type of photic retinopathy caused by solar radiation. Similar conditions such as laser maculopathy, welder’s maculopathy, and eclipse maculopathy also fall under the photic retinopathy umbrella. Damage to the macula is thought to occur through photochemical retinal injury and not due to thermal injury.1
Excessive light energy incident on the retina leads to free radical formation which damages surrounding retinal and RPE tissue. Higher energy light such as ultraviolet tends to be more destructive due to the greater generation of free radicals.
Patients with solar retinopathy tend to be young, male, with clear ocular media, and a history of sungazing.2 If no history of sungazing can be elicited, it is important to probe for psychiatric conditions or illicit drug use that may lead to forgetfulness or alteration of behavior. It is important to consider other types of photic retinopathy that can be caused by occupational dangers such as welding or laser exposure.
Patients will often present complaining of bilateral central or paracentral scotomas with mildly reduced vision in the 20/25 to 20/100 range. The visual deficits tend to correlate with the duration of photic exposure and the intensity of the light source.
Upon dilation, patients can have a variety of findings such as a foveal yellow/red spot, granular pigmentation, or macular hole depending on the intensity of light exposure and length of time since exposure. Likewise, OCT findings will vary with outer retinal hyper-reflectivity, outer retinal disruption, RPE disruption, outer retinal cavitation/hole, and macular hole all being reported in the literature.
In the first 1-8 weeks, the OCT and funduscopic findings tend to change quite rapidly as the retina heals. After the initial healing phase, patients will typically present with outer retinal and/or RPE disruption/cavitation as noted in the case above.
Unfortunately, no standardized management guidelines for solar retinopathy exist and no treatment has been shown to be particularly helpful in improving long term vision. Visual deficits are self-limiting, often times returning to near pre-injury levels. Central scotomas may persist even if visual acuity improves. Patients with mild initial visual deficits (better than 20/30) tend to have better and quicker visual recovery.3
The mainstay of management should focus on patient education to prevent initial or subsequent episodes of solar retinopathy.
Back to the patient
This case of solar retinopathy was unusual because the patient was asymptomatic, the funduscopic/OCT findings incidental, and he denied sun gazing. Probing for other possible forms of light exposure, psychiatric issues, forgetfulness, or illicit drug use was also negative. Though his OCT findings seemed classic for solar retinopathy, I also considered cone dystrophy and retinal pigment epithelitis as possibilities. Considering that the patient was asymptomatic with unremarkable color vision and 10-2 visual field testing, I decided to follow the patient as chronic solar retinopathy.
As with all unknown retinal conditions that I do not think require intervention, I decided to follow up with the patient in 1 month. VA, funduscopy, and OCT were all stable. The patient was still asymptomatic. I then followed the patient in 2, 3, and 6 months and all findings continued to be stable. I now follow the patient yearly and he is still asymptomatic with stable funduscopic and OCT findings.
The OCT Progression analysis in Figures 4 and 5 reveals stability of both maculae 1 year after initial presentation.

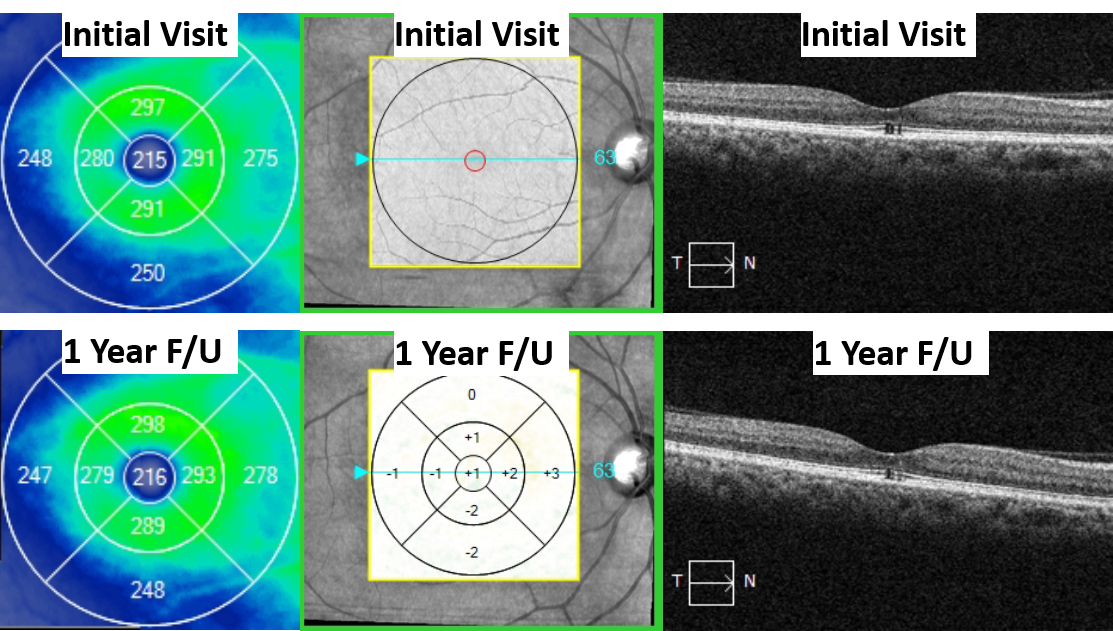
Figure 4: Left macula

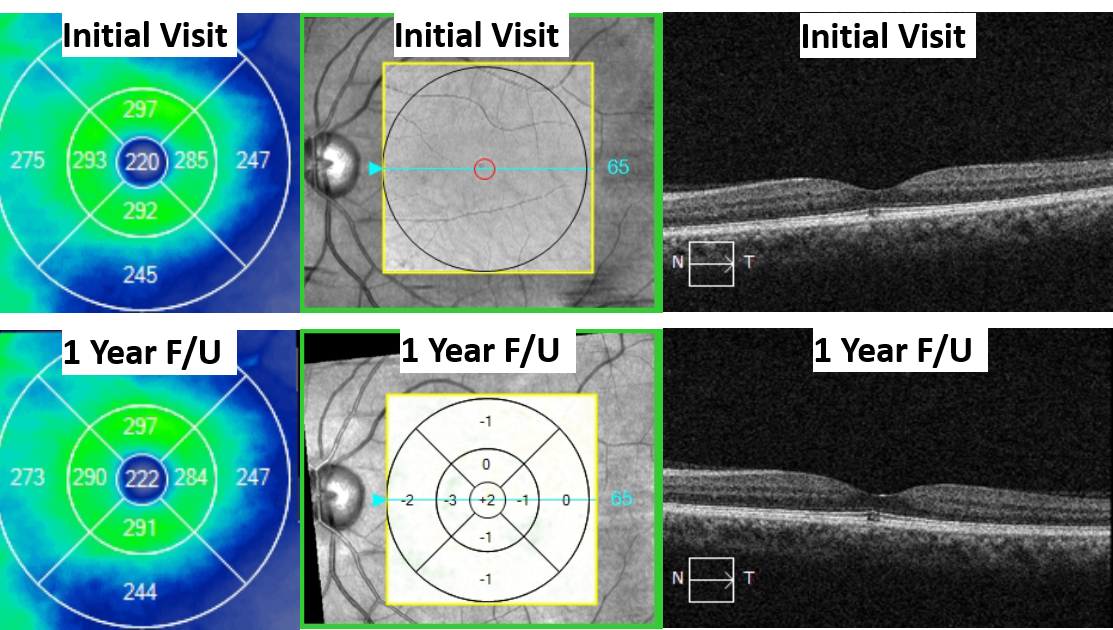
Figure 5: Right macula
Solar retinopathy and the other entities that fall under photic retinopathy are an interesting group of maculopathies that are quite rare but can often be diagnosed through history alone. The amount of vision loss and retinal damage will vary with the duration and intensity of light exposure. Though no treatment for solar retinopathy exists, visual recovery is spontaneous with most patients achieving good post-injury vision.
References
- Youssef, P. N., N. Sheibani, and D. M. Albert. "Retinal light toxicity." Eye 25.1 (2011): 1-14.
- MacFaul, P. A. "Visual prognosis after solar retinopathy." The British Journal of Ophthalmology 53.8 (1969): 534.
- Atmaca, Leyla S., Aysun Idil, and Deniz Can. "Early and late visual prognosis in solar retinopathy." Graefe's archive for clinical and experimental ophthalmology 233.12 (1995): 801-804.
