



Fundus photography involves capturing detailed images of the retina using a specialized fundus camera, and plays a crucial role in diagnosing and managing a wide range of ocular and posterior segment diseases.
In 1886, Jackman and Webster first published photographs of the retina, marking the beginning of advances in retinal imaging, which were further revolutionized by the introduction of the first commercial fundus camera by Carl Zeiss in 1926.1
Significant innovations followed, including:1
- Metzger’s stereoscopic photographs in 1927
- Attachment of an electronic flash tube by Hansell and Beeson in 1953
- Invention of the digital camera by Steven Sasson in 1975
- Development of modern technologies like confocal scanning laser ophthalmoscopy and widefield, non-mydriatic cameras from companies such as ZEISS, Canon, and Topcon
Fundus photography is a powerful diagnostic tool that plays an instrumental role in the detection, monitoring, and management of retinal diseases. Advances in technology in fundus photography have made it indispensable for both routine and complex eyecare.
Optometrists need a solid understanding of image interpretation to identify early signs of retinal pathology and to provide optimal patient care. This guide will cover key retinal pathologies identified on a funduscopic exam, interpretation of relevant biomarkers, and the latest developments in fundus imaging technology.
Fundus photography for retinal disease detection and monitoring
Fundus photography captures detailed images of the retina, allowing clinicians to evaluate the optic nerve head, macula, retinal blood vessels, and the surrounding areas for abnormalities.
These images serve to document the current state of the retina, establishing baseline data for future reference, and can assist with monitoring for progression and assessment of treatment effectiveness.
Fundus photography offers several key advantages in the management of retinal and ocular diseases. Early detection is one of its primary benefits, as subtle retinal changes can often be identified before symptoms manifest, allowing for prompt intervention.
Serial imaging further enhances its utility by enabling the monitoring of disease progression over time, which is particularly critical in chronic conditions such as diabetic retinopathy (DR) and age-related macular degeneration (AMD).
Additionally, fundus photographs provide permanent, high-resolution visual documentation that can be shared with other specialists for collaborative care, as well as with patients for education about their condition and treatment options.
Modalities and special features of fundus photography
Widefield fundus imaging
Widefield fundus imaging offers a much broader view of the retina than traditional fundus photography. By capturing up to 200 to 300° of the retinal surface, this technique is invaluable for assessing the peripheral retina, a region often involved in conditions such as retinal detachment, DR, and retinal vascular occlusions.2
Widefield and ultra-widefield imaging are particularly useful additions to the dilated fundus exam for careful inspection of ischemia and neovascularization in peripheral regions that might be missed with standard imaging.3 These are fast, noninvasive methods that are increasingly used for the management of conditions with retinal pathology.

Widefield Fundus Exams for Retinal Pathology Cheat Sheet
This cheat sheet outlines key retinal pathology and relevant biomarkers that can be imaged with widefield fundus photography.

Fundus autofluorescence (FAF)
Fundus autofluorescence (FAF) is a noninvasive imaging technique that provides detailed information about the retina's health, especially in the macula and peripheral regions.
It works by capturing the natural fluorescence emitted by retinal structures, primarily lipofuscin, when exposed to specific wavelengths of light. This allows for the visualization of retinal abnormalities, such as areas of atrophy, degeneration, or lipid accumulation, which may not be apparent on traditional imaging.4
FAF imaging is particularly valuable in monitoring retinal conditions that affect the retinal pigment epithelium (RPE), such as AMD, DR, and inherited retinal dystrophies. It can detect early changes in the RPE before visible structural changes are seen on other imaging modalities, such as optical coherence tomography (OCT) or fundus photography.
Widefield FAF, similar to widefield fundus photography, extends the visualization to the peripheral retina, helping to identify pathological changes outside the central macula.
This broad coverage is crucial for comprehensive assessment, as many retinal pathologies, including diabetic macular edema, retinal vein occlusions, and inherited retinal disorders, can have peripheral manifestations.
Furthermore, FAF is helpful in monitoring disease progression and response to treatment, providing clinicians with essential information for managing retinal conditions effectively.
Like widefield imaging, FAF is a rapid, noninvasive technique that enhances the ability to detect subtle changes across the entire retina, aiding in early diagnosis and timely intervention. As such, it is increasingly incorporated into routine clinical practice for the management of a variety of retinal diseases.
An overview of fundus findings
Table 1: Key landmarks found in a normal fundus exam of a healthy retina.
| Structure | Typical Findings | Common Pathologies |
|---|---|---|
| Optic Disc | Round or slightly oval, neuroretinal rim respecting the ISNT rule, symmetric cup-to-disc ratio in both eyes | Glaucoma: Optic disc cupping, asymmetry in cup-to-disc ratio, breaking ISNT rule |
| Macula (Macula lutea + fovea centralis) | Small, dark, circular area in the central retina, free of lesions, hemorrhages, or abnormalities; central depression reflects light, flat and free of pigment, blood, or lesions, foveal reflex present in younger patients | Macular degeneration: Drusen, geographic atrophy, macular edema; Macular edema: Thickening, cystoid spaces |
| Retinal vasculature | Arteries lighter than veins, A/V ratio 2:3, vessels uniformly small with no arteriolar narrowing or vascular nicking | Diabetic retinopathy: Microaneurysms, hemorrhages, cotton wool spots, neovascularization; Hypertensive retinopathy: Widening of arteriolar light reflex, copper-wiring of arterioles, hemorrhaging, cotton wool spots, hard exudates, retinal edema |
| Retinal background / posterior pole | Smooth, even coloration; absence of hemorrhages, exudates, or pigmentary changes in the macular region and periphery | Diabetic retinopathy: Hard exudates, hemorrhages; Hypertensive retinopathy: Flame-shaped hemorrhages, cotton wool spots, arterial narrowing |
| Retinal periphery | Tapered vessels with less density, vitreous base meets ora serrata, visible dentate processes at retinal periphery | Retinal detachment: Retinal tears, peripheral ischemia, subretinal fluid |
Figure 1: Labeled fundus photograph of key landmarks outlined in Table 1.


Figure 1: Courtesy of Inrava Khasnabish, OD, FAAO.
Clinical application of fundus photography
The management of a variety of retinal pathologies is enhanced with retinal photography, as it is used for documentation of a condition in its current state, detecting subtle changes over time, and in some cases, confirmation of a diagnosis.
Common key conditions in which fundus photography is a critical aspect of clinical management are outlined below, along with characteristic clinical biomarkers and clinical pearls that assist in both diagnosis and management.
Diabetic retinopathy (DR)
Diabetic retinopathy is the most common cause of vision loss in working-age adults in the US, and is characterized by vascular damage leading to ischemia, swelling, and eventually vasoproliferation in the retina.5 Early stages often do not exhibit symptoms, while pathologic changes are visible on fundus photography.6,7
As DR progresses from non-proliferative to proliferative, and as diabetic macular edema (DME) may ensue, fundus photography can be instrumental in noticing subtle changes as well as confirming the stage and making proper referral decisions.
In addition, DR is a particularly poignant example of when to use fundus photos to assist in patient education. Visualizing retinal bleeding can often have a meaningful impact on patients who have not yet fully recognized their risk of vision loss with continued medication or diet noncompliance, for example.
Table 2: Breakdown of DR stages with corresponding descriptions of clinical characteristics on fundus imaging.8,9
| DR Stage | Fundus Appearance | Description |
|---|---|---|
| Mild non-proliferative diabetic retinopathy (NPDR) | Retinal microaneurysms | Tiny, round, red spots appearing on the retina, often seen in the peripheral retina |
| Retinal hemorrhages | Dot or blot-shaped hemorrhages, typically in the outer plexiform and inner nuclear layers, visible as small red dots | |
| Exudates | Yellowish, well-defined deposits in the retina, often around the macula, indicating lipid and protein accumulation | |
| Moderate NPDR | Cotton wool spots | White, fluffy patches in the retina, usually near the optic disc or in the posterior pole, signifying nerve fiber layer infarctions |
| Venous beading | Bead-like dilations and tortuosity of retinal veins, seen as irregular, dilated veins in the mid-peripheral retina | |
| Severe NPDR | Intraretinal microvascular abnormalities (IRMAs) | Abnormal, dilated, tortuous vessels in the retina, often visible as abnormal, branching blood vessels in the mid-peripheral retina, indicating ischemia |
| Proliferative diabetic retinopathy (PDR) | Vitreous hemorrhage | Presence of blood in the vitreous cavity, visible as hazy or clouded areas obscuring the retinal view |
| Retinal neovascularization | New, abnormal blood vessels, often seen at the optic disc or on the retinal surface, appear as fine, fragile, irregular vessels that may be in the process of growing or bleeding | |
| Diabetic macular edema (DME) | DME | Swelling of the macula, often accompanied by lipid exudates, is visible as thickening in the macular region, which may cause loss of the normal foveal reflex |
Fundus photography pearls for DR:
- Using an image swap or overlay feature in photography software can assist in identifying subtle changes. Early detection is crucial for preventing progression to severe stages.
- Using a red-free filter on most fundus cameras (emitting green light at 570nm) assists in viewing blood vessels and aids in evaluating their caliber, crossing changes, or the presence of pathology.10
- Patients with mobility issues, for whom sitting through dilated fundus exams can be challenging, may benefit from photography-guided dilated fundus exams.
- This type of exam relies on both a fundus photo in addition to a dilated fundus exam to closely evaluate retinal health and screen for diabetic changes.
- Widefield photography offers increased visibility for evaluating retinal changes pertaining to diabetic retinopathy outside of the posterior pole, which may not be as easily visualized during a dilated fundus exam alone
- Widefield swept-source OCT angiography provides a non-invasive, high-resolution alternative to fluorescein angiography and ultra-widefield fundus photography for detecting diabetic retinopathy lesions, bleeding, and edema.11
- Photography allows for time-consuming comparison and analysis that fundus examination often does not.
- Simple zoom features, as well as enhancement filters or tools, can be used to inspect high-risk areas for early neovascularization. For example, cotton-wool spots will often predict the future location of IRMA and retinal neovascularization.
- Photography can be used in addition to OCT in the close monitoring of mild center-involving (CI)-DME when acuity is 20/30 or better, as seen in Figure 2 below.
Figure 2: Fundus photograph of moderate NPDR with center-involving macular edema.


Figure 2: Courtesy of Inrava Khasnabish, OD, FAAO.
Age-related macular degeneration (AMD)
A leading cause of central vision loss in the elderly, AMD occurs as either dry (nonexudative) or wet (exudative or neovascular). Dry AMD is most common, occurring in 90% of affected individuals, while 10% progress to wet AMD.8,9
Table 3: Breakdown of AMD stages with corresponding descriptions of clinical characteristics on fundus imaging.8,9
| AMD Stage | Fundus Appearance | Description |
|---|---|---|
| Dry AMD (nonexudative) | Drusen | Small, yellowish deposits under the retina, often clustered near the macula; drusen are a hallmark of early dry AMD |
| Geographic atrophy | Well-defined areas of retinal thinning and atrophy, particularly in the macular region, leading to visible tissue loss | |
| Wet AMD (exudative / neovascular) | Pigment epithelial detachments (PEDs) | Elevated areas of the retina, often with a “tear-drop” shape, caused by fluid accumulation beneath the RPE |
| Subretinal hemorrhages | Red or dark patches on the retina, often around the macula, indicating bleeding from abnormal blood vessels | |
| Choroidal neovascular membrane (CNVM) | Irregular, abnormal blood vessels beneath the retina, often seen in the macula with red / green / brown hue, which may leak fluid or blood, causing retinal distortion |
Fundus photography pearls for AMD:
- Use the green-free filter to enhance the visibility of drusen. This filter increases contrast between the yellowish drusen deposits and the surrounding retina, making them stand out, especially in the early stages of dry AMD.10
- Fundus photography is essential for detecting early signs of AMD, such as drusen and pigment epithelial detachments. Early identification allows for monitoring progression, especially in dry AMD, before it progresses to the wet form.
- Regular fundus photography is key for monitoring geographic atrophy, a late-stage manifestation of dry AMD. It helps clinicians observe the extent of retinal tissue loss and plan for intervention if needed.
- The leading edge of progressing geographic atrophy often shows hyperfluorescence on FAF. This hyperfluorescence indicates metabolic activity at the outer retina, and its appearance is useful for assessing disease progression.2
- This can help identify areas of active degeneration and predict the potential expansion of atrophic regions.
- Widefield imaging provides a broader view of the retina, which is useful for detecting AMD-related changes, particularly in areas that might not be visible with a standard fundus exam. This is especially helpful for detecting peripheral lesions or early-stage changes.
- Fundus photography can help identify CNVMs, abnormal blood vessels that form under the retina in wet AMD. Detecting CNVM early is crucial for preventing further vision loss and guiding treatment options.
- Fundus photography is an effective tool for educating patients about the progression of AMD. Visualizing changes such as drusen, geographic atrophy, or hemorrhages can help patients understand the severity of the condition and the importance of adhering to treatment and follow-up visits.
Figures 3 and 4: Fundus images of intermediate AMD with large drusen and advanced dry AMD (i.e., geographic atrophy), respectively.

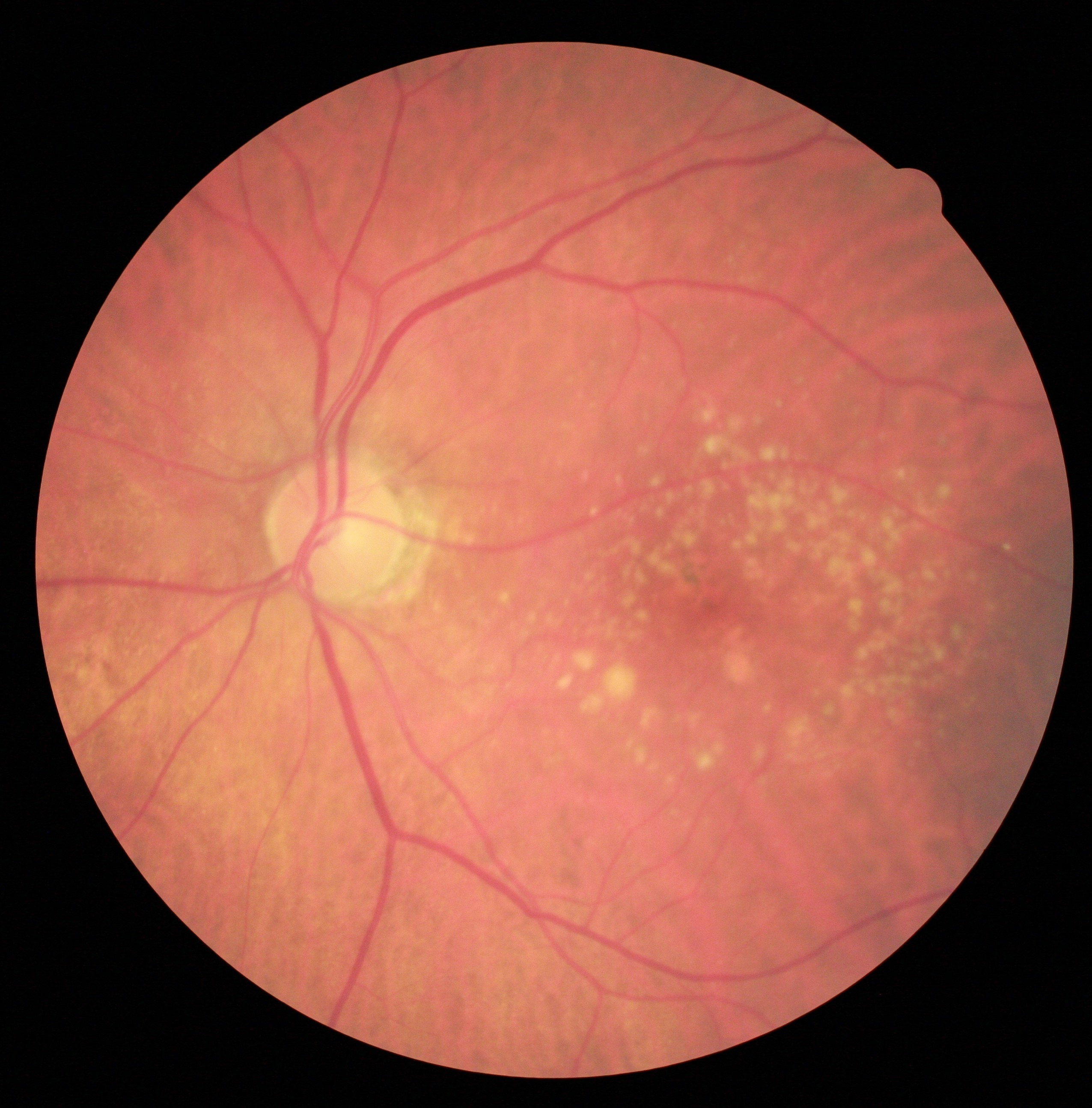
Figure 3: Courtesy of Julie Rodman, OD, MSc, FAAO.

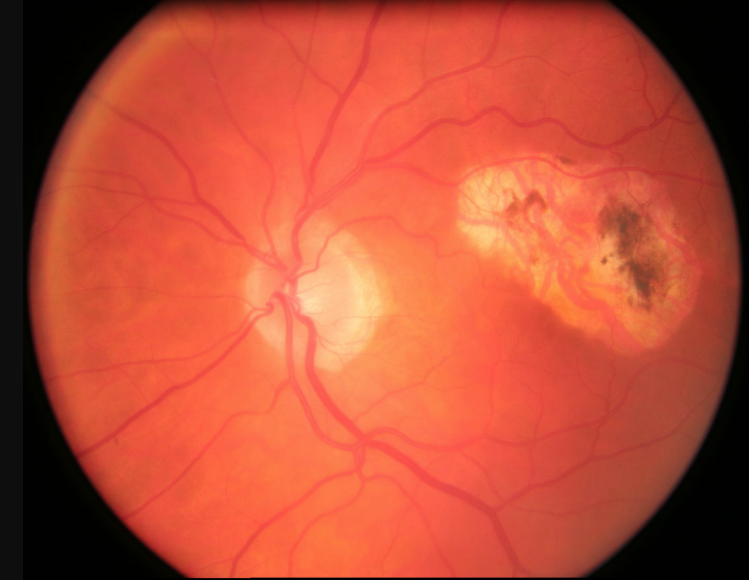
Figure 4: Courtesy of Julie Rodman, OD, MSc, FAAO.
Retinitis pigmentosa
Retinitis pigmentosa (RP) is a hereditary condition that leads to progressive retinal degeneration, initially affecting night vision and peripheral vision, followed by central vision loss.8,9 Patients often present with night blindness and reduced peripheral vision.
Table 4: List of clinical characteristics of retinitis pigmentosa that can be identified on fundus imaging.8,9
| Clinical Findings | Description |
|---|---|
| Bone spicule-like pigment | Scattered pigment deposits in the peripheral retina |
| Attenuated retinal vessels | Narrowing of the retinal vessels |
| Optic nerve pallor | Seen in advanced stages of retinitis pigmentosa |
Fundus photography pearls for RP:
- FAF can assist with early diagnosis, which is key for genetic counseling. Active areas of progression will demonstrate hyperfluorescence due to lipofuscin deposits, while atrophy will be hypofluorescent
Figure 5: Fundus images of bone spicules in the periphery, attenuated blood vessels, and waxy pallor of the optic disc due to retinitis pigmentosa.


Figure 5: Courtesy of Inrava Khasnabish, OD, FAAO.
Retinopathy of prematurity (ROP)
Advancements in retinal imaging for pediatric and premature populations have led to the development of specialized tools such as handheld fundus imaging systems.12 These technologies enable clinicians to perform effective retinal screenings in infants and young children who may be unable to cooperate with traditional imaging methods.
In particular, early detection of retinopathy of prematurity (ROP), a leading cause of childhood blindness, has been greatly improved with these innovations, allowing for more timely interventions. ROP affects premature infants, characterized by abnormal retinal blood vessel growth. If untreated, it can lead to retinal detachment and blindness.8,9
Table 5: Breakdown of ROP stages with corresponding descriptions of clinical characteristics on fundus imaging.8,9
| ROP Stage | Fundus Appearance | Description |
|---|---|---|
| Stage 1 | Line of demarcation | A white line that separates the vascularized retina from the avascular retina, indicating the boundary of retinal development |
| Stage 2 | Ridge formation | A raised, white ridge at the junction of vascular and avascular retina, signifying more advanced retinal neovascular activity |
| Extraretinal neovascularization | Fine, frond-like vessels growing outward from the retina, marking the onset of neovascular changes | |
| Stage 3 | Exuberant neovascularization | Prominent, fragile blood vessels extend into the vitreous, leading to increased risk of hemorrhage and traction |
| Plus disease | Dilated and tortuous blood vessels, typically seen in the posterior retina, indicating worsening vascular pathology | |
| Retinal edema | Swelling of the retina, often causing blurred margins of the optic disc, indicative of worsening retinal pathology | |
| Stage 4 | Retinal folds | Wrinkling of the retina caused by fibrous tissue traction, leading to deformation of the retinal structure |
| Vitreous hemorrhage | Presence of blood in the vitreous cavity, often resulting from ruptured neovascular vessels | |
| Stage 5 | Complete retinal detachment | Presence of blood in the vitreous cavity, often resulting from ruptured neovascular vessels |
| Severe vitreous hemorrhage | Complete obscuration of the retina due to massive blood accumulation in the vitreous, hindering vision |
Fundus photography pearls for ROP:
- Retinopathy of prematurity is a leading cause of blindness in premature infants.
- Regular screening in preterm infants is essential for early intervention.
- Capturing fundus photography on the pediatric population can be challenging, external fixation (sometimes with toys) assist tremendously with capturing fundus photos
Figures 6 and 7: Fundus images of stage 1 and stage 3 ROP, respectively.


Figure 6: ROP fundus images© Xinyu Zhao, et al. Image cropped and used under CC BY 4.0.


Figure 3: ROP fundus images© Xinyu Zhao, et al. Image cropped and used under CC BY 4.0.
Other technologies and developments enhancing fundus examination
Advancements in fundus imaging techniques have substantially improved the ability to diagnose, monitor, and manage retinal diseases.
These innovations offer optometrists and ophthalmologists enhanced diagnostic tools to detect early signs of retinal conditions, track disease progression, and guide treatment decisions.
OCT angiography (OCTA)
OCTA is a groundbreaking, non-invasive imaging technique that visualizes retinal and choroidal blood flow without the need for dye injection.
By detecting variations in the light reflection from blood vessels, OCTA produces high-resolution images of retinal vasculature. This makes it particularly valuable for identifying early microvascular changes in conditions such as diabetic retinopathy, AMD, and retinal vein occlusions.13
OCTA allows for the visualization of both superficial and deep capillary networks, helping to detect early pathologic change such as capillary drop-out or neovascularization, prior to structural manifestations becoming apparent.14
This technology can be meaningful for the optometrist in order to make proper referrals for proliferative retinopathy, and is likewise useful for a retinal specialist in monitoring responses to anti-VEGF therapy.
Artificial intelligence (AI)
AI has made significant strides in retinal imaging, enhancing the diagnostic process with machine learning algorithms capable of analyzing retinal images with remarkable accuracy.
AI systems can automatically detect and classify retinal diseases, including diabetic retinopathy, AMD, and glaucoma, by identifying key features such as microaneurysms, hemorrhages, and drusen.
These AI tools can also quantify biomarkers—such as the size of drusen or the extent of hemorrhages—which is crucial for tracking disease progression and determining treatment effectiveness.14
With the ability to predict disease progression based on historical data, AI is enhancing early detection, streamlining screening processes, and enabling more personalized treatment plans.
Fusion of OCT and OCTA
This emerging technique combines structural imaging with functional vascular information.2,14 This integrated approach provides a more comprehensive view of retinal diseases, particularly those with both structural and vascular components, such as DME and wet AMD.
The combination of OCT’s detailed imaging of retinal thickness and OCTA’s visualization of blood flow enhances the ability to track disease progression and evaluate responses to therapy, making it an essential tool for managing complex retinal conditions.2
Billing considerations for fundus photography
As of 2025, there are significant updates in the billing and reimbursement landscape for fundus photography and related imaging technologies, particularly with the Centers for Medicaid and Medicare Services' new fee schedule.15
One of the most notable changes is the introduction of a new CPT code for OCTA. This advanced imaging technique, which allows for noninvasive visualization of retinal blood vessels without dye injection, has been increasingly adopted in ophthalmic practices.
The new CPT code 92137 for OCTA, effective January 1, 2025, combines traditional OCT of the retina with OCTA in a single procedure, offering a more accurate representation of the service. However, practitioners should note that OCTA cannot be billed in the same visit as other OCT codes (92133 or 92134), so careful attention to coding is necessary.
Approximate national average reimbursement for 92137 per the Medicare Physician Fee Schedule is $56.93, compared to its counterparts 92134 (OCT retina) $31.38 and 92235 (fluorescein angiography) $152.68.15
Using modifier 52 for coding fundus photography
In addition to the new OCTA code, another important consideration for fundus photography is the proper use of modifier 52. This modifier is used when a reduced service is performed, such as testing only one eye rather than both in a bilateral procedure like fundus photography (CPT code 92250).
Fundus photography is generally a bilateral service, meaning that it is expected to be performed on both eyes. If only one eye is imaged, the service is considered reduced, and modifier 52 should be applied to indicate that a partial service was provided.
This helps ensure that the practice is paid appropriately for the reduced service while avoiding claim denials. It's also important to remember that OCTA and fundus photography are mutually exclusive for billing, so when both are performed on the same day, they must be billed separately, with proper justification.
Managing the workflow for fundus photography, along with staying on top of coding changes, is key to maximizing efficiency and revenue. For example, some payors may reimburse for screening fundus photos in diabetic patients (92250 CPT code + E11.9 ICD-10 code), providing a valuable opportunity for practices that manage a large diabetic population.
Keeping up with these billing nuances and educating both staff and patients about the importance of retinal imaging, especially for those at risk of retinal diseases, will help ensure practices not only remain compliant but also improve patient outcomes and financial health.15
Tip: Always verify insurance coverage for diabetic screenings before performing the service to ensure proper reimbursement.
Conclusion
Fundus photography is a critical tool for optometrists in the diagnosis and monitoring of various retinal diseases. Understanding the biomarkers associated with these conditions, such as hemorrhages, exudates, and neovascularization, is essential for early detection and timely intervention.
With ongoing advancements in imaging technology, optometrists are equipped with the ability to identify subtle retinal changes that may have significant clinical implications. Keep honing your skills in fundus imaging interpretation, as it is one of the most powerful ways to safeguard and preserve your patients' vision.
