


Age-related macular degeneration (AMD) is the leading cause of blindness in the developed world in people over 50 years old.1 AMD can be subcategorized into nonexudative or “dry” AMD and neovascular or exudative/“wet” AMD.
As of 2020 in North America, it was estimated that 11 million (80 to 90% of all AMD patients) had dry AMD and 1.5 million (10 to 15% of all AMD patients) had exudative AMD.1
Overview of age-related macular degeneration
Risk factors for the development of AMD include increasing age, smoking, genetic susceptibility, female sex, light irides, hypertension, hyperlipidemia, cardiovascular disease, higher waist-to-hip ratio in men, elevated CRP, and hyperopia.
Additionally, two major susceptibility genes include CFH (1q31), which codes for complement factor H, and ARMS2 (10q26), whose function is poorly understood.1 The 10-year Multi-Ethnic Study of Atherosclerosis demonstrated a higher prevalence of AMD in white patients, intermediate prevalence in Hispanic and Asian patients, and lowest prevalence in African American patients.2
Dry atrophic AMD
Drusen in the macula are pathognomonic for non-neovascular AMD, and these areas correspond to abnormal thickening of Bruch's membrane. Drusen can be categorized by their appearance on the exam and can be called “soft” (amorphous/poorly demarcated) or “hard" (discrete/well demarcated).1
Figure 1 shows an optical coherence tomography (OCT) scan of subretinal soft drusen deposits in dry AMD.

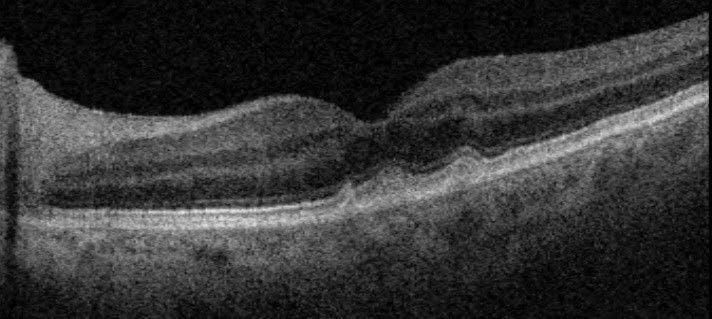
Figure 1: Courtesy of Kevin Cornwell, OD.
Soft drusen in the macula are more likely to progress to retinal atrophy or choroidal neovascularization (CNV) than hard drusen.1 Additionally, the thickening of the Bruch's membrane, along with retinal pigment epithelium (RPE), may cause a separation leading to a pigment epithelial detachment (PED). When large, these PEDs can be categorized or described as a “drusenoid PED,” which helps stage the degree of macular degeneration.
An additional finding in dry AMD is changes to the RPE. These changes include focal hyperpigmentation, focal atrophy, and geographic atrophy.1 Focal hyperpigmentation appears as increased pigmentation at the outer retina. Focal atrophy appears as areas of RPE mottling or frank depigmentation. When such lesions are confluent and have a diameter greater than 175μm, this is termed geographic atrophy.1
Figure 2 demonstrates the clinical states of AMD.

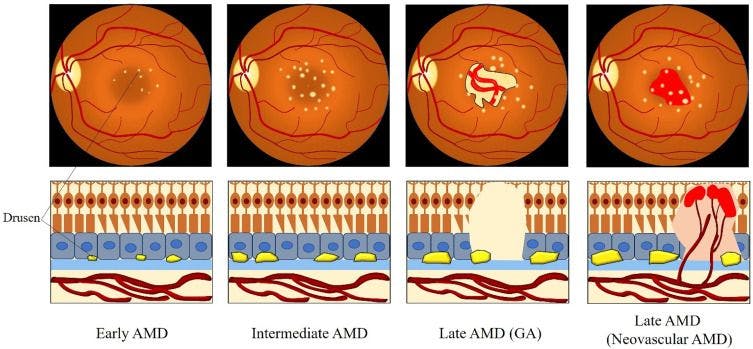
Figure 2: Courtesy of Ruan et al.
According to the Age-Related Eye Disease Study (AREDS), the risk of progression to stage 4 AMD for patients with early AMD was ~1.3%.5 The risk for progression for patients with many intermediate drusen or even one large druse (stage 3) was 18%.4
Drusen are categorized by size according to the AREDS study:4
- Small drusen: <63μm
- Intermediate drusen: 63 to 124μm
- Large: >125μm
- Drusenoid PED: >350μm (confluent large drusen that coalesce)
The AREDS/AREDS2 studies additionally demonstrated a benefit to starting AREDS vitamins in patients with intermediate or advanced AMD to help reduce the rate of vision loss and helping to slow the progression of AMD.5 Because of this potential benefit with starting AREDS2 vitamins, sizing the drusen is important for discussing when to start AREDS2 vitamins.
Figure 3 illustrates areas of geographic atrophy seen on different imaging modalities.5


Figure 3: Courtesy of Fleckenstein et al.
Neovascular AMD
The presence of choroidal neovascularization is the defining characteristic of neovascular AMD.1 Degenerative changes in the Bruch’s membrane lead to an angiogenic environment (an environment that helps new bad blood vessels to grow) which can lead to neovascularization from the choriocapillaris. This neovascularization can perforate Bruch’s membrane (which will look like heme in the fovea on the exam) and will lead to a hypertrophic, fibrotic disciform scar.1
5 pearls for monitoring the clinical progression of AMD
1. Visual acuity changes
First and most importantly, monitoring for clinical signs comes from setting up strict return precautions with patients regarding changes in visual acuity. Patients with mild to moderate macular degeneration may have slight worsening of vision, decreased contrast sensitivity, decreased color vision, and impaired dark adaptation (takes longer for their vision to adjust after being exposed to a bright light).1
Patients with wet AMD can have acute worsening vision with a worsening scotoma. These patients need to be seen urgently for evaluation with clinical exam, OCT evaluation, and possible intravitreal injection.
2. Amsler grid monitoring
Discussion, as well as providing a patient with an Amsler grid, is helpful in surveying AMD progression. An Amsler grid is a test card with white grid lines on a black background a white background with black grid lines and a central dot for fixation. A patient is recommended to place the Amsler grid on their fridge or their bathroom mirror and test each eye individually with glasses as needed.
The patient is checking for new scotoma, distortion (metamorphopsia), or significant change in central vision. If a patient develops vision changes, it is important to discuss that they follow up promptly for evaluation. New distortion could mean conversion to wet AMD or the development of new subretinal or intraretinal fluid in wet AMD, leading to scarring and permanent vision loss.
Figure 4 demonstrates an Amsler grid, while Figure 5 demonstrates the wavy lines/distortion that can be a sign of worsening wet AMD and would need prompt evaluation for possible intravitreal injection.6

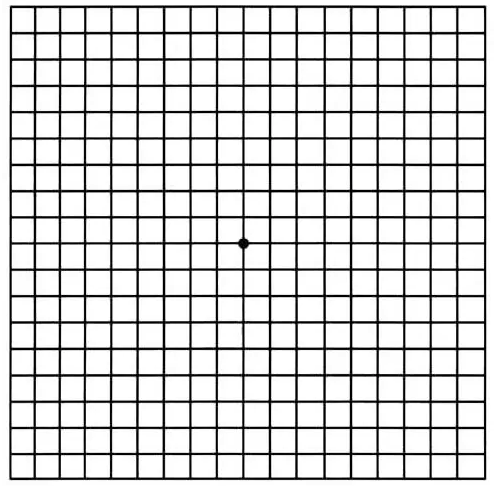
Figure 4: Courtesy of the American Academy of Ophthalmology.

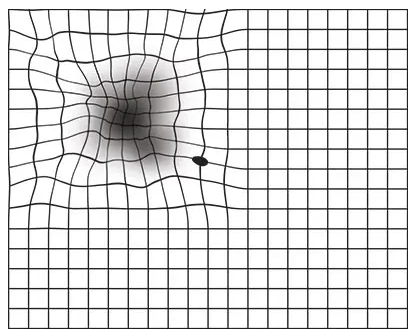
Figure 5: Courtesy of the American Academy of Ophthalmology.
3. Spectral-domain OCT (SD-OCT) of the macula
Changes of small and large drusen on an OCT macula for nonexudative AMD can show sub-RPE nodular elevation, small RPE detachments, and absence of intraretinal and subretinal fluid. Signs of worsening nonexudative AMD can be an increasing number of drusen, an increase in drusen size, or the development of confluent drusen, indicating the patient may need shorter follow-up periods compared to annual screening.
SD-OCT macula helps aid the diagnosis of conversion to exudative AMD as well as monitoring response to treatment. Elevation of the RPE and PEDs can be seen in Type 1 CNV. Serous PEDs can be sharply elevated, dome-shaped lesions with hollow internal reflectivity, typically without subretinal or intraretinal fluid.1
Fibrovascular PEDs tend to have hyperreflective lesions at the RPE. Chronic fibrovascular PEDs often have a multilayered appearance.1 Type 2 CNV appears as a hyperreflective band with associated subretinal and/or intraretinal fluid.1
In Figure 6, we see exudative macular neovascularization with subretinal fluid, intraretinal fluid, and lipid exudation.

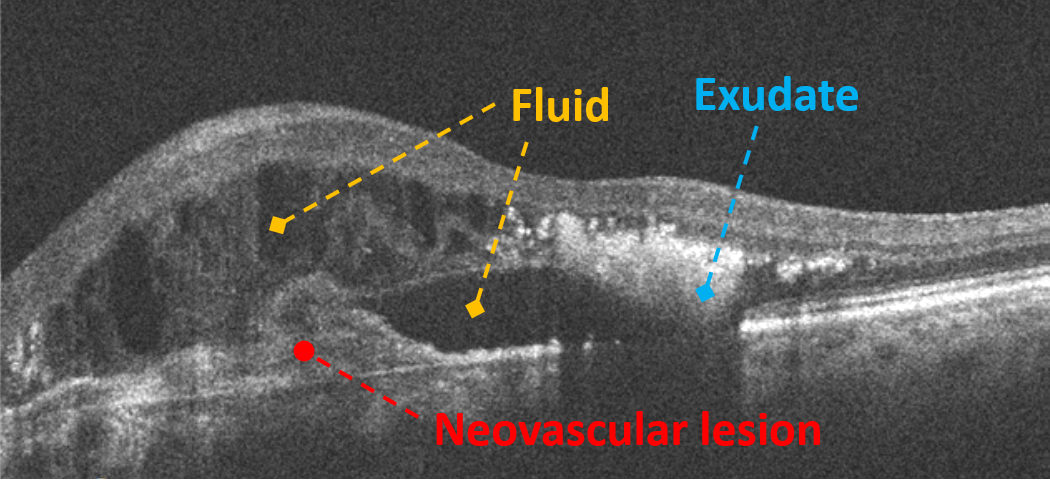
Figure 6: Courtesy of Daniel Epshtein, OD, FAAO.
4. Fluorescein angiography (FA)
Drusen appearance on fluorescein angiography can vary depending on the size and the number of drusen. Typically, hard drusen hyperfluoresce early in FA studies due to window defects (defect in RPE allows transillumination of choroidal hyperfluorescence) are seen on FA.1 Larger soft drusen, confluent drusen, and drusenoid PEDs stain later in the sequence of an FA because of pooling of fluorescein dye.1
FA patterns for wet AMD can be categorized as classic or occult, or a combination of both. Classic CNV typically has a well-defined hyperfluorescent lesion that appears in the early phase and progressively leaks by the later phases.1
Occult CNV refers to diffuse hyperfluorescence that can have either:
- Fibrovascular PED
- Vascularized serous PED, which can either have slow leakage or pooling
- Late leakage from an undetermined source.
5. Hyperacuity testing
Hyperacuity, also known as Vernier acuity, measures the ability to detect a deviation in the alignment of visual objects.1 Hyperacuity helps patients to tell minute deviations on a single line. In the Vernier acuity test, two parallel lines are presented, with one slightly offset from the other. For people with intact hyperacuity, they can detect which line is misaligned or shifted.
Hyperacuity is sensitive to shifts in the outer retinal morphology (where the changes occur in AMD), producing a perception of distortion.1 The preferential hyperacuity perimetry (PHP) can be used to detect recent onset CNV in intermediate AMD with high sensitivity and specificity preferential.8
Figure 7 demonstrates this through an animated Vernier scale.9

Figure 7: Courtesy of Wikipedia.
In conclusion
Age-related macular degeneration is the leading cause of blindness in patients over 50 in developed countries.1 Discussion with the patients of risk factors (especially cessation of smoking), the subtypes of AMD, and the need for continual lifelong monitoring are important.
Visual acuity, Amsler grid monitoring, spectral domain OCT, fluorescein angiography, and hyperacuity testing are key to helping monitor the progression of AMD. Treatments for macular degeneration are ongoing, and using these tools to help monitor clinical progress can save vision when caught early in the disease course.
