


On this episode of Pressure Points Glaucoma, Justin Schweitzer, OD, FAAO, is joined by Derek Cunningham, OD, FAAO, to review how to weigh the benefits and risks of different topical glaucoma medications for a patient who requires aggressive intraocular pressure (IOP) control.
Dr. Cunningham is the director of the Dry Eye Institute at Dell Laser Consultants in Austin, Texas, and has conducted research on a vast spectrum of eyecare and neuroscience, such as dry eye treatments, glaucoma medications and surgeries, retinal disease, and cataract and refractive surgery.
Case report
A 74-year-old Caucasian male patient presented to the clinic after undergoing combined cataract and glaucoma surgery with two stents who had recently been diagnosed with glaucoma. His best-corrected visual acuity (BCVA) was 20/20-1 OU, and he was using a generic prostaglandin analog (PGA) qd OU.
The clinical examination revealed:
- T-Max: 28mmHg OU
- IOP: 24mmHg OD, 20mmHg OS
- C/D: 0.70/0.70 OD, 0.60/0.60 OS
- Gonioscopy: Open to ciliary body (CB) OU with trace pigment in the trabecular meshwork (TM)
- Slit lamp examination (SLE): Well-centered IOLs OU
As shown below, the patient’s optical coherence tomography (OCT) and visual field testing (VFT) showed structural and functional signs of progression OD. Conversely, the patient’s left eye remained stable.
Figures 1 and 2: OCT imaging OD showing temporal superior and temporal inferior quadrant progression and a ganglion cell defect.


Figure 1: Courtesy of Justin Schweitzer, OD, FAAO.

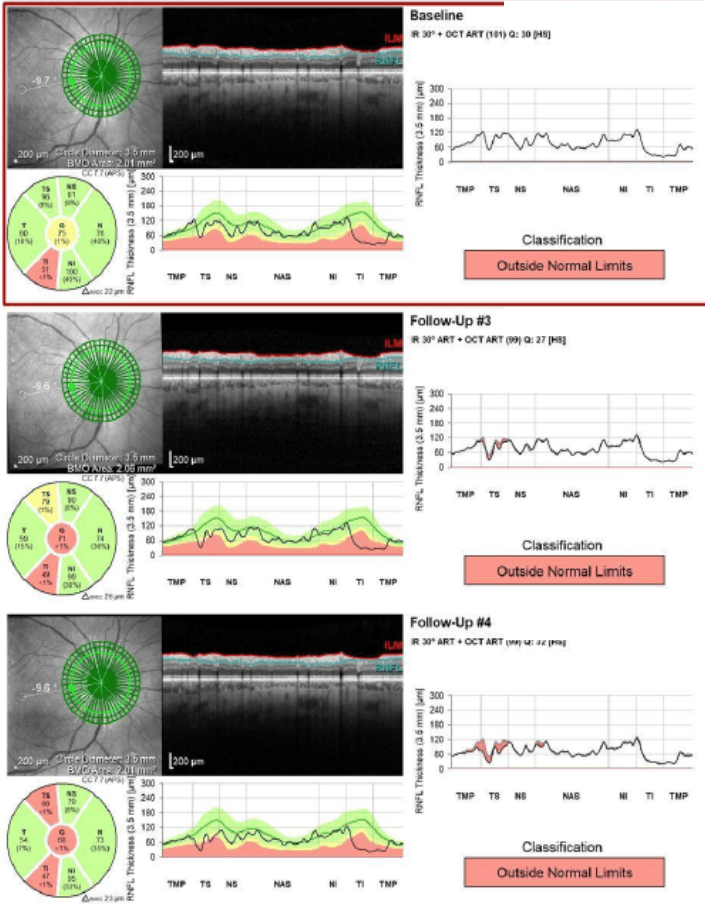
Figure 2: Courtesy of Justin Schweitzer, OD, FAAO.
Figure 3: VFT OD demonstrating an increase in the pattern standard deviation (PSD) from 4.96 to 5.51 to 6.82, and a slowly worsening localized defect.


Figure 3: Courtesy of Justin Schweitzer, OD, FAAO.
Initial reflections on the case
Dr. Cunningham’s key takeaways from the case:
- The structural analysis demonstrated concerning signs of glaucoma progression that require aggressive treatment
- The patient had notably high IOP despite topical therapy and microinvasive glaucoma surgery (MIGS)
- The use of a generic PGA is a potential red flag, as the efficacy of ophthalmic generic medications may vary depending on the inactive ingredients, pH, viscosity, levels of particulate matter, degradation, and who manufactured the medication1
- Of note, generic formulations can be brought to the market quickly at a low cost because manufacturers are not required to repeat the rigorous animal or clinical research required of brand-name drugs1
He also recommends that glaucoma patients and suspects undergo cataract extraction as soon as it is indicated because studies have demonstrated that it can cause significant post-operative IOP and medication reductions as well as improved visual field and retinal nerve fiber layer (RNFL) exam parameters.2
Treatment approaches for this patient
In Dr. Cunningham’s experience, switching topical glaucoma medications is a relatively easy way with minimal risk to adjust the treatment approach. As such, he considers which drop will most likely address the root cause of glaucoma—trabecular meshwork outflow.
While latanoprost is the most commonly prescribed PGA, it does not directly affect TM outflow; instead, it has a complementary mechanism of action to lower IOP by increasing uveoscleral outflow.3 Fortunately, innovations in glaucoma medications have led to the FDA approval of drops with additive mechanisms of action that combine the effect of latanoprost (i.e., uveoscleral outflow) with nitric oxide (NO) and rho-kinase inhibitors to increase aqueous outflow.3,4
These are namely VYZULTA (latanoprostene bunod ophthalmic solution 0.024%, Bausch + Lomb) and ROCKLATAN (netarsudil and latanoprost ophthalmic solution 0.02% / 0.005%, Alcon), respectively. Because these medications directly address TM outflow, Dr. Cunningham explained that his next step for this patient would be to prescribe one of these two drops.
Clinical trial data on latanoprostene bunod
The long-term efficacy and safety of latanoprostene bunod (LBN) 0.024% was demonstrated in the JUPITER Study, in which 130 Japanese participants (mean age 62.5 years) with open-angle glaucoma (OAG) or ocular hypertension (OHT) instilled LBN 0.024% in one eye qPM for 1 year.3 The mean baseline IOP of the participants was 19.6mmHg and 18.7mmHg in study and treated fellow eyes.
By week 4, patients achieved mean IOP reductions from baseline of 22.0% and 19.5% in study and fellow eyes, respectively, and these reductions were maintained through week 52.3 Dr. Cunningham noted that the JUPITER Study determined that LBN could significantly lower IOP even in glaucoma patients with moderate IOP levels—which is much more difficult than lowering high IOP to medium-low levels.
To learn more about the NO-donating PGAs, check out The Role of Nitric Oxide in Glaucoma Treatment!
Clinical trial data on netarsudil/latanoprost
In the MERCURY-1 and -2 studies, patients with OAG and OHT instilled one drop of netarsudil 0.02% / latanoprost 0.005% fixed-dose combination (FDC, n=483), netarsudil 0.02% (n=499), or latanoprost 0.005% (n=486) into each eye once daily in the evening.4 The baseline mean diurnal IOP was 23.6, 23.6, and 23.5mmHg in the cohorts, respectively.
The mean diurnal IOP levels in each group during the study period were as follows:4
- Netarsudil 0.02% / latanoprost 0.005%
- Week 2: 15.2mmHg
- Week 6: 15.7mmHg
- Week 12: 15.8mmHg
- Netarsudil 0.02%
- Week 2: 18.1mmHg
- Week 6: 18.4mmHg
- Week 12: 18.4mmHg
- Latanoprost 0.005%
- Week 2: 17.5mmHg
- Week 6: 17.4mmHg
- Week 12: 17.3mmHg
At month 3, among patient randomized to netarsudil/latanaprost FDC or latanoprost, 58.4% vs. 37.3% achieved IOP ≤16mmHg.4 For patients randomized to netarsudil/latanoprost FDC or netarsudil or latanoprost, 30.9% vs. 5.9% vs. 8.5% achieved at least a 40% reduction from baseline in mean diurnal IOP, respectively.
Ultimately, once-daily netarsudil/latanoprost FDA produced statistically significant and clinically relevant reductions in mean IOP that were statistically superior to IOP reductions achieved by netarsudil and latanoprost monotherapy.4
Conclusion
Additional considerations for topical glaucoma medications include:
- Prescribing fixed-combination agents can help to minimize the number of drops patients need to instill daily while maintaining comparable side effects and outcomes5
- Dr. Cunningham cautioned clinicians on the efficacy of compounded glaucoma medications, as more data is required to compare their efficacy to manufactured products and guide clinical care6
Preservative-free formulations are a good option for patients struggling with medication adherence due to the cytotoxic effects of ophthalmic preservatives on the corneal and conjunctival epithelium

