


Various retinal side effects have been noted in patients undergoing oncological treatments, including biologics, small molecule inhibitors, and platinum analogs.
It is essential to monitor patients for retinal changes due to such treatments, as a change in medication regimen may be warranted. Retinal damage must be addressed promptly, as permanent vision loss can occur.
This article will discuss common oncological treatments and their effects on the retina.
Table of agents used for oncological treatments
Table 1 outlines the various drug classes used for oncological treatments, their respective agents, as well as resulting retinal toxicity.
| Drug Class | Agents | Retinal Toxicity |
|---|---|---|
| Biologic agents | Ipilimumab, Nivolumab, Pembrolizumab, Avelumab | Uveitis, exudative retinal detachment |
| Small molecule inhibitors | Imatinib, Vandetanib, Nilotinib | Retinal hemorrhage, optic nerve edema, cystoid macular edema |
| Platinum-based agents | Cisplatin, Carboplatin, Oxaliplatin | Ischemic retinopathy, granular pigmentary deposits, altered color vision, optic nerve edema/hemorrhage, macular edema |
| Retinoids | Fenretinide, Isotretinoin | Night vision impairment |
| Antineoplastic agents | Mitotane | Optic disc edema, retinal hemorrhages |
| Antimicrotubular agents | Vincristine, Vinblastine, Vinorelbine | Toxic optic neuropathy |
Table 1: Courtesy of Farhaad Rasool
Retinal side effects of biologic agents
Biologic agents are a group of recombinant proteins, typically antibodies, designed to disrupt specific immunological processes.1 Most commonly, biologics are used to treat autoimmune diseases and malignancies. One example of a biologic is ipilimumab, which is used to treat metastatic colorectal cancer.
Its mechanism of action includes activation of the immune system by targeting CTLA-4, which downregulates T-cell activation pathways.1 This drug has been associated with bilateral severe uveitis, which may further progress to exudative retinal detachment.1 This detachment is characterized by a rapid loss of vision and may be associated with alopecia, vitiligo, poliosis, and neurological symptoms.1
This condition can cause permanent vision loss; thus, ipilimumab should be discontinued immediately.1 Additionally, Vogt-Kayanagi-Harada (VKH) disease can occur in patients using nivolumab or cemiplimab, both of which may be taken in conjunction with ipilimumab.
Figure 1 is fundus photography showing an exudative retinal detachment.2

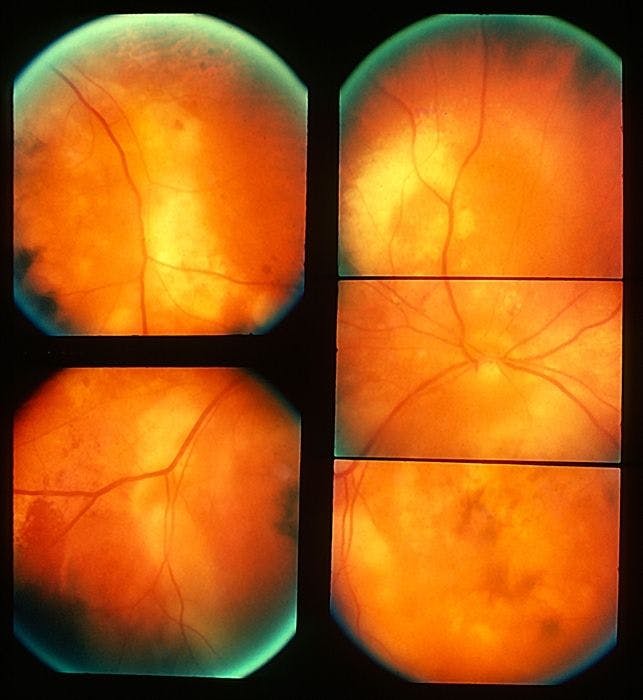
Figure 1: Courtesy of Thomas M Aaberg, MD
Retinal side effects of small molecule inhibitors
Another class of oncologic drugs is small molecule inhibitors, which include tyrosine kinase inhibitors, such as imatinib. Imatinib is an anti-neoplastic agent used in the treatment of chronic myelogenous leukemia (CML) and acute lymphocytic leukemia (ALL).
Its mechanism of action is characterized by competitive inhibition of the tyrosine kinase that results from the abnormal BCR-ABL and c-KIT gene.1 In rare instances, imatinib has been shown to cause retinal hemorrhages within the first few months of initiating treatment.1
“These retinal hemorrhages will typically resolve without additional management.”
There have also been reported cases of optic nerve edema and cystoid macular edema, which generally require management from a retinal specialist.1 The medication may need to be discontinued, as there are no current treatment options.1
Figure 2 displays intraretinal cystoid spaces present in cystoid macular edema.3

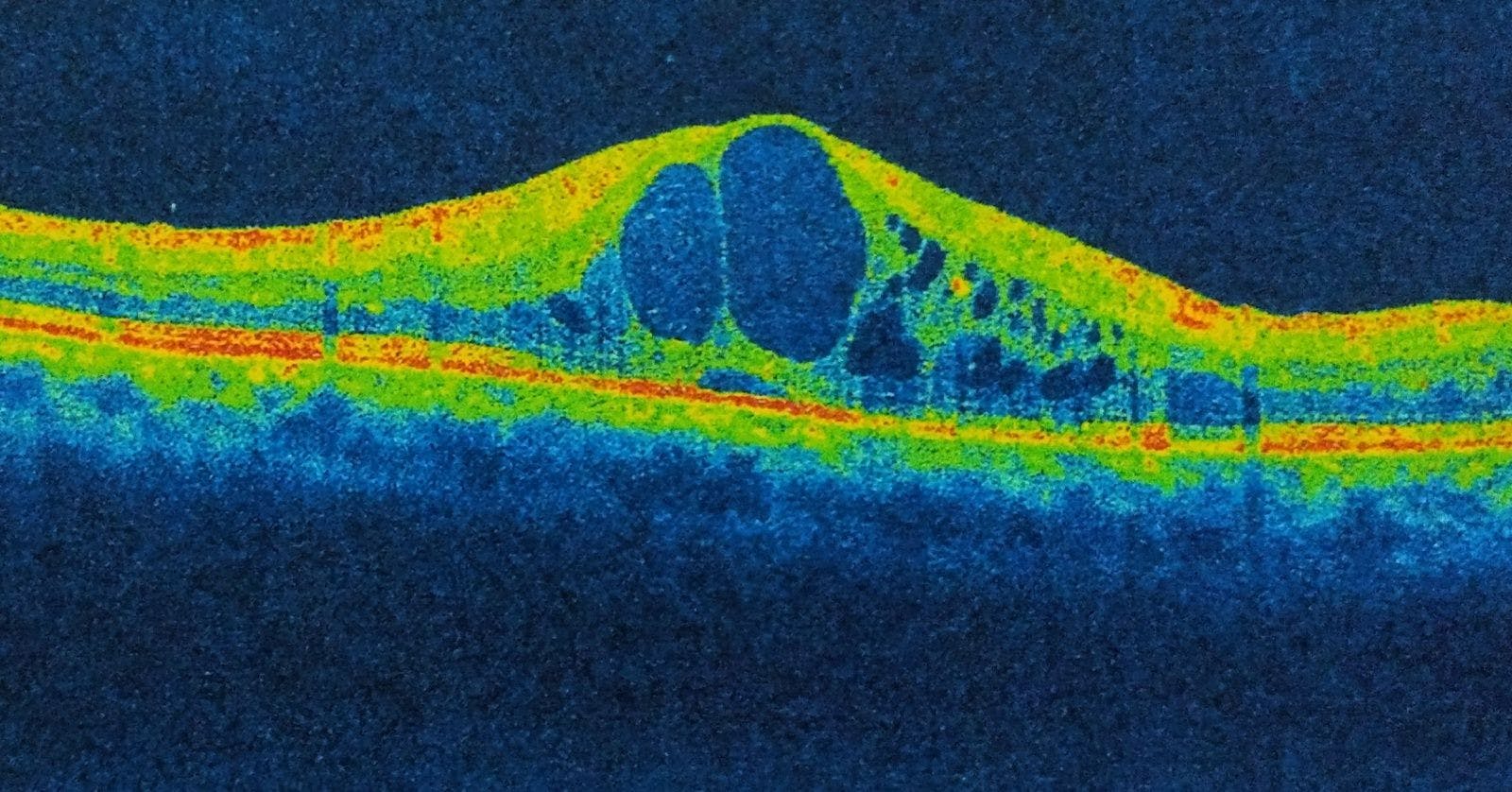
Figure 2: Courtesy of Diana V Do, MD
Retinal side effects of platinum-based agents
Platinum-based agents are another group of chemotherapeutic agents that work by cross-linking DNA strands, which decreases DNA replication. Cisplatin, carboplatin, and oxaliplatin are common agents used in the treatment of lymphomas and solid tumors, including bladder, testicular, and ovarian cancer. There have been reports of retinal toxicity with cisplatin, including ischemic retinopathy.1
Additionally, systemic cisplatin can cause granular pigmentary deposits and altered color vision, which can take anywhere from months to years to return to normal.1 The use of carboplatin may result in optic nerve edema with hemorrhages and macular edema.1 Even if the drug is discontinued at first, signs of retinal damage, irreversible vision loss, and optic atrophy have been reported.1
Retinal side effects of retinoids
Retinoic acid derivatives, otherwise known as retinoids, are vitamin A derivatives used in the treatment of cancers such as breast, prostate, and lung cancer.
“Retinoic acid normally plays a role in cell development and differentiation.”
Its mechanism in cancer treatment includes impairing estrogen signaling in breast cancer cells by disrupting the activation of LSD1 via protein kinase A.4 Certain synthetic retinoids, such as fenretinide and isotretinoin, have been associated with night vision impairment.5
Various studies have confirmed this and show the resolution of impairment once discontinuing the drug.5 Thus, it is essential to ask patients if they have been experiencing difficulties seeing at night and advise against particular activities, like operating a vehicle.
Retinal side effects of mitotane
Mitotane is a drug that directly inhibits the synthetic function of the adrenal cortex and is used to treat advanced adrenal cancer.1 The maximum dosage ranges from 8 to 10 grams per day and has been associated with toxic retinopathy; this is characterized by optic disc swelling and retinal hemorrhages.1 Information regarding the reversibility of the side effects is unknown at this time.1
Figure 3 is a fundoscopy demonstrating pigmentary clumping and macular edema secondary to mitotane usage.6


Figure 3: Courtesy of Ng et al.
Retinal side effects of antimicrotubular agents
Antimicrotubular agents are a type of mitotic inhibitor and include the vinca alkaloids, vincristine, vinblastine, and vinorelbine.1 These drugs act by binding beta-tubulin, leading to the inhibition of beta-tubulin polymerization into microtubules and thus causing the mitotic arrest of cells in metaphase.
Antimicrotubular agents are used to treat neuroblastoma, rhabdomyosarcoma, and nephroblastoma. Vincristine can cause toxic optic neuropathy, resulting in vision loss.1 One histological study showed the loss of ganglion cells of the retina and optic nerve fiber atrophy.1 Because optic nerve damage due to vincristine may be reversible, it is recommended that the drug be discontinued, but this decision is made on an individual basis.
Conclusions
Although retinal side effects of oncology treatments are rare, they can be severe and lead to permanent damage if not managed appropriately. Ophthalmologists should converse with their patients regarding vision changes, especially when a patient is following a chemotherapeutic regimen. If a patient presents with an ocular sign or symptom, it should be established whether or not this is due to the patient’s malignancy or an effect of their chemotherapy.1
“A dilated fundus examination helps differentiate whether a side effect is due to a metastasis or drug.”
Following this delineation, there should be a discussion of whether symptoms are manageable or if the best course of action is discontinuing the agent.1 The risk-benefit profile, and any relevant effects on quality-of-life, need to be considered when evaluating these adverse events.
