




As an eyecare professional, you constantly rely on retinal imaging as an indispensable tool to help establish a diagnosis. Since 2018, the advancement in ultra-widefield imaging (UWFI) has allowed for a wider fundus view—up to 200°—approximately 82% of the total retinal surface area.
One of the most commonly used devices to achieve this is the Optos ultra-wide camera (Optos PLC), which is a significant improvement compared to the traditional 30° to 60° devices. Using a scanning laser ophthalmoscope, the Optos provides single capture, non-mydriatic imaging of the retinal periphery without the need for a contact lens.
Advantages of ultra-widefield imaging
UWFI has revolutionized the diagnostic and therapeutic landscape of retinal diseases in a myriad of manners.
1) Most of the peripheral retina can be visualized using Optos UWFI. There is growing confirmation that UWFI provides information not readily available with traditional imaging techniques, including identifying peripheral retinal pathology that might otherwise be missed. Since many eye conditions first appear on the outer periphery and influence disease progression, UWFI can allow their early identification and timely management.
2) UWF images are characterized by an enhanced resolution (up to 2000 by 2000 pixels), a short processing time, and fast acquisition (within 0.25 seconds). This is particularly advantageous in your non-compliant patients who are unable to focus on multiple photographs, as seen in Figure 1A, below. It can also help with clinical efficiency, with less time needed to examine each patient.
Figure 1A illustrates exudative retinopathy in the left eye of a 19-year-old boy diagnosed with Coats disease, while in Figure 1B, UWF fluorescein angiography shows peripheral leakage requiring treatment.

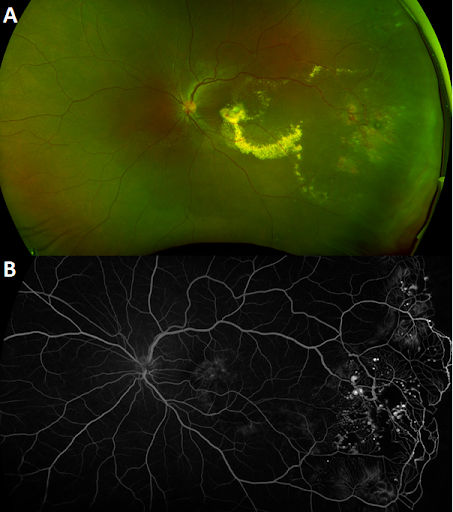
Figure 1
3) Easier examination of patients with small pupils or vitreous opacities.
4) UWFI provides a tangible source for patient education (e.g., demonstrating a retinal tear while discussing treatment options, such as laser retinopexy). Refer to Figure 2, below, which demonstrates a retinal hole in the periphery left eye of a 16-year-old asymptomatic boy.

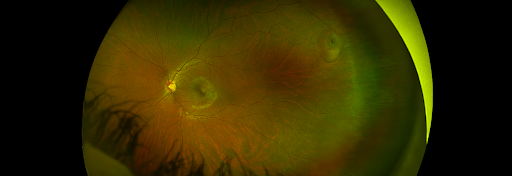
Figure 2
5) Many patients have some degree of lens opacification, and images in these cases can be better acquired with Optos camera than a traditional fundus camera.
UWFI with fluorescein angiography
Fluorescein angiography (FA) remains the gold standard for detecting retinal vascular abnormalities in ophthalmic practice. However, traditional cameras limit the visualization of capillaries and the deep retinal vasculature.
Nowadays, you can use UWF FA to identify pathologies that otherwise would not be detectable by standard angiography fields in many cases. Additionally, you will be able to image the central and peripheral retina simultaneously. This allows for a complete evaluation of peripheral retinal ischemia in patients with diabetic macular edema and other vascular complications in the central macula.
Furthermore, UWF FA has become a mainstay in diagnosing and monitoring uveitis. It offers visualization of subtle pathologic changes and can help determine treatment, including the need for immunosuppressive therapy or scatter laser photocoagulation. It reveals more vascular leakage than conventional FA or OCTA; a finding considered a sensitive surrogate indicator of clinical inflammation.
This technique is especially suited to retinal conditions such as sickle cell retinopathy, familial exudative vitreoretinopathy, retinopathy of prematurity, and Coats disease, showing leakage and/or peripheral avascularity, as seen again in Figure 1B.


Figure 1B: revisited.
UWFI with optical coherence tomography angiography
Optical coherence tomography angiography (OCTA) is an emerging non-invasive modality that provides fast structural and functional information about retinal and choroidal vascularization through laser light reflectance of the surface of moving red blood cells. With the advance of a UWF montaging technique, swept-source OCTA (SS-OCTA) has allowed the acquisition of a larger field of view with high-resolution and depth-resolved images compared to spectral-domain OCTA (SD-OCTA) systems.
This SS-OCTA imaging method has the potential to reveal retinal microvascular alterations in the superficial and deep retinal capillary plexus as well as in choriocapillaris.
When ordering images from many available tests for patients, you must prioritize accuracy, invasiveness, and rapidity. Imaging with the UWF SS-OCTA helps detect subtle pre-clinical changes without the need for an intravenous line, nurse, or crash cart and provides rapid imaging results. Studies have suggested that over 95% of neovascularization in diabetic retinopathy can be detected on widefield OCTA using a montage of scans.
In Figure 3, montage optical coherence tomography angiography of the total retina shows neovascularization in the superior temporal arcade.

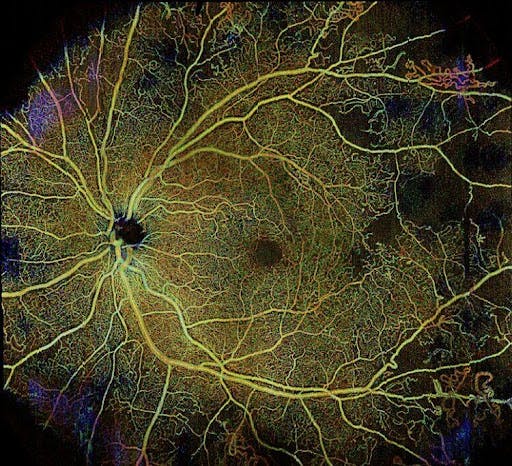
Figure 3
Limitations of ultra-widefield imaging
Despite the significant progress of this imaging modality, there remain some limitations inherent to UWFI, namely:
- It can be affected by image artifacts from cataracts or corneal pathology.
- In asymptomatic patients, incidental and non-threatening findings such as peripheral retinal hemorrhages, as seen in Figure 4, can prompt an unnecessary workup.
Figure 4 reveals an incidental finding of pinpoint retina hemorrhages from vitreous traction in the temporal periphery of a 36-year-old asymptomatic female with 20/20 vision.
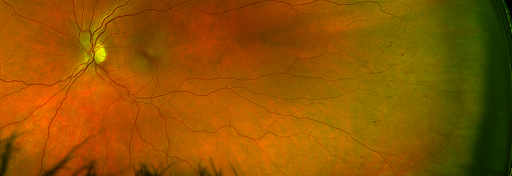
Figure 4
- It can be difficult to precisely measure the retinal surface area to estimate the size and dimensions of lesions.
- Conversion of a rounded, three-dimensional surface to a two-dimensional image is still an issue. This leads to areas of nonlinearity such that a line near the posterior pole will be very different in actual size from one drawn in the periphery.
- True color is lacking, as this technology uses a scanning laser ophthalmoscopy (SLO).
Implementation of UWFI
Implementation of UWFI in clinical practice requires an initial significant cost to purchase the device. Additionally, training photographers are needed to acquire high-quality images.
Vital practice note: UWFI fundus photo (CPT code 92250) and OCT (CPT code 92134) cannot be billed on the same day for the diagnosis.
Ultra-widefield imaging cases
Case 1
A 55-year-old female presented with decreased vision for 3 months. Her past medical history was notable for including body myositis, Isaac’s syndrome, and myocardial infarction at age 48. Her visual acuity was 20/20 in the right eye and 20/40 in the left eye (Snellen).
Ultra-widefield fundus imaging showed temporal intraretinal hemorrhage in the right eye (Figure 5A), inferotemporal subhyaloid hemorrhage, peripheral intraretinal hemorrhages, a macular epiretinal membrane, and a cyst with dehemoglobinized blood in the left eye (Figure 5B).
Ultra-widefield fluorescein angiography revealed temporal peripheral leakage and capillary dropout in both eyes (Figure 5C and 5D). She was treated with scatter laser photocoagulation to the peripheral ischemic retina, with improved vision to 20/15 and resolved leakage after 4 months.

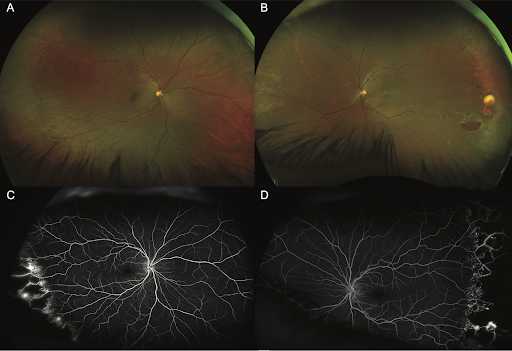
Figure 5
Case 2
A 31-year-old female without a history of prematurity or visual complaints presented for routine evaluation. Her visual acuity was 20/20 in both eyes (Snellen). UWFI revealed inferotemporal vessel tortuosity, ischemia past a ridge of traction and neovascularization in the left eye (Figure 6A).
Ultra-widefield fluorescein angiography demonstrated inferotemporal leakage and avascularity in the left eye (Figure 6B). She was treated with laser photocoagulation to the peripheral retina. She underwent genetic testing and was diagnosed with familial exudative vitreoretinopathy.

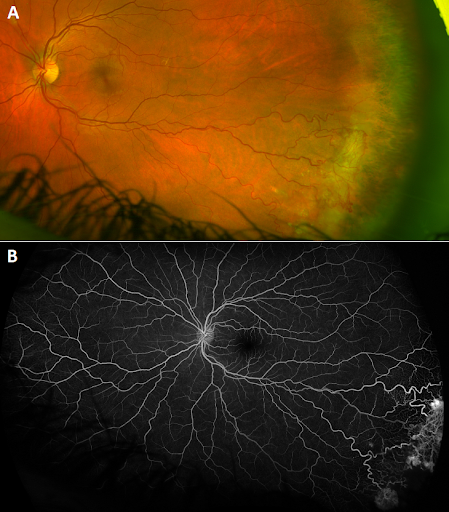
Figure 6
Conclusions
There are clear benefits to using ultra-widefield imaging in your eye clinic: dramatically improved peripheral retinal view, high-resolution images with fast acquisition times, facile examination through a small pupil, and tangible proof of findings to counsel patients and foster disease education. Adopting this new technology is critical for optometrists and ophthalmologists alike to boost clinical efficiency and accuracy.

