





Herpes simplex viruses (HSV) are large double-stranded DNA viruses. HSV is divided into HSV-1 and HSV-2. While HSV-1 is typically associated with oral lesions, HSV-2 is primarily associated with genital lesions. However, both viruses may cross-infect different areas of the body depending upon opportunities for direct physical contact.1
Up to 80% of adults in the US have HSV-1.2 This typically causes cold sores or blisters inside or around the mouth; however, ocular complications can also occur. Although ocular manifestations are most commonly caused by HSV-1, they can be associated with HSV-2 when acquired by neonates during the birthing process via an infected birth canal.3
Prevalence of ocular manifestations of HSV
The impact of ocular herpes is substantial, as it can lead to recurrent episodes of inflammation, scarring, and possible vision loss. In rare cases, HSV can cause neurological complications, including encephalitis or meningitis.
Herpes simplex keratitis is both the most common cause of infectious keratitis and the leading cause of corneal blindness in the US.4 There are approximately 20,000 new cases and 28,000 recurrent cases annually.5
Due to the potential for recurrence and the risk of complications, the proper understanding, diagnosis, and management of ocular herpes is crucial.
Primary HSV infection
Typically, the primary herpes simplex virus infection occurs in the pediatric population. The primary outbreak is often mild or subclinical (90% of people are asymptomatic) and can go unrecognized.
It is spread by direct contact of skin or mucous membranes with infectious secretions. Fever and lymphadenopathy may be associated, manifesting as a nonspecific upper respiratory tract infection.6
Primary ocular HSV-1 occurs most commonly on the skin and mucosal conjunctival surfaces innervated by cranial nerve V. Of note, 90% of the cases are unilateral and result in preauricular lymphadenopathy with cutaneous vesicles on eyelid skin or margin.
Primary HSV infection presentation
It mainly presents as blepharitis and/or follicular conjunctivitis. It less commonly causes keratitis, and when it does, it typically presents as punctate epithelial lesions or epithelial dendrites.
Stromal keratitis develops in <10% of patients with primary infection. Blepharoconjunctivitis is typically self-limiting; however, treating it can reduce the severity, duration, and possible spread.
Blepharoconjunctivitis and keratitis treatment options can include topical or oral antiviral medications.7 To treat external lid lesions, an antibiotic ointment BID to QID (used for prophylaxis) or a topical antiviral agent such as ganciclovir 0.15% gel can be used.
Reactivation of the virus
After the primary infection, the virus travels to the trigeminal ganglion, where it replicates and becomes latent. It later reactivates and travels to the cornea. HSV can cause episodic ocular disease, but it will remain in the trigeminal ganglion for life.
Most clinical ocular infections are manifestations of virus reactivation. Most cases are unilateral, with recurrences affecting the same eye. Bilateral disease, which is not necessarily concurrent, occurs in 1 to 12% of cases and is more common in patients with atopy or other immune-related conditions.8
Environmental and physiologic events may trigger reactivations. These may include UV radiation, hormonal changes, fevers, corneal trauma, and immunocompromised states.
Making the HSV diagnosis
The diagnosis of ocular herpes is primarily a clinical one. In some cases, polymerase chain reaction (PCR) testing may be done via a sample from the affected area. Additionally, serologic tests may be done to detect rising antibody (Ab) levels during primary infection; however, they are of no assistance for recurrent disease.
The absence of HSV-Ab may help to serve as a negative predictive value to rule out HSV as the cause of disease. Therefore, a detailed ocular examination, including corneal sensitivity testing, is crucial for appropriate diagnosis and management.9
Is it HSV or HZV?
To differentiate an HSV infection from the herpes zoster virus (HZV) infection, consider presentation, distribution, progression, and patient age.
Table 1 outlines different factors to consider in the differential diagnosis between HSV and HZV.
| Trait | HSV | HZV (Shingles) |
|---|---|---|
| Anterior Segment Presentation | Herpetic keratitis: Redness, tearing, and discomfort. The classic dendritic corneal ulcer has terminal end bulbs. | Herpes zoster ophthalmicus: Painful skin rash with periocular involvement. May occur with a pseudo-dendrite on the cornea (with no terminal end bulbs). |
| Distribution | Can affect any part of the eye, but corneal involvement is most common. | Primarily involves dermatomal distribution of the ophthalmic division of the trigeminal nerve, affecting the lids, cornea, and conjunctiva. It is unilateral and does not cross the midline. |
| Disease Progression | After the primary infection is acquired via direct contact, the virus stays dormant in the ganglia, leading to reactivation. Recurrent episodes of keratitis are possible. | Primary infection (chickenpox) acquired through the respiratory tract, remains latent in the dorsal root ganglia and may become reactivated. |
| Age | Commonly affects individuals of all ages. | More common in older adults. |
Table 1: Courtesy of the authors.
Figure 1 highlights a clinical photo of herpetic keratitis that demonstrates an epithelial dendrite with associated stromal edema.

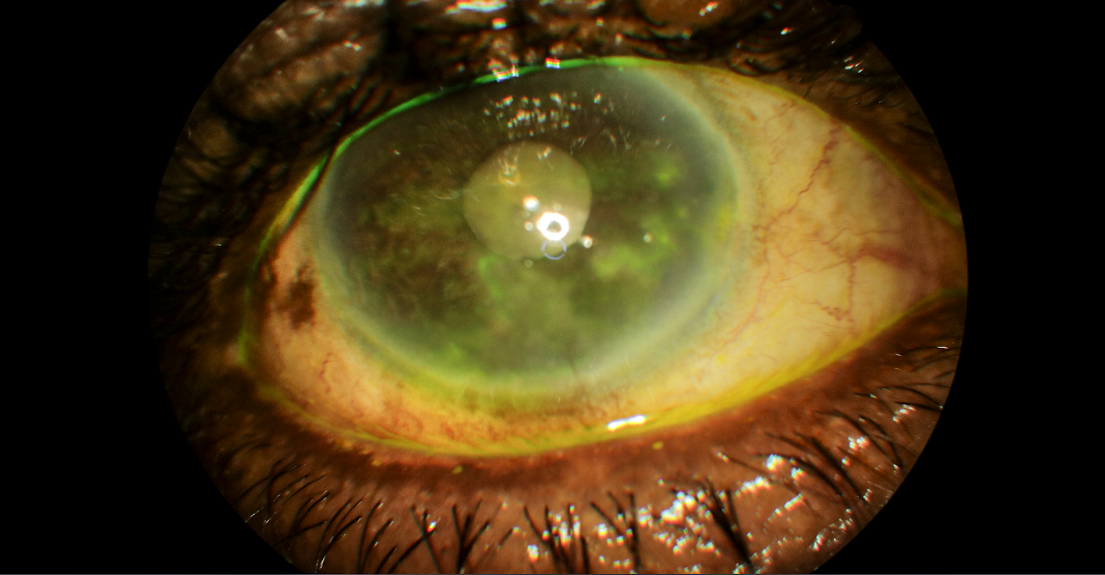
Figure 1: Courtesy of Evan Canellos, OD, FAAO, Dipl ABO.
Ocular findings and treatments for HSV
Ocular manifestations of HSV reactivation include blepharitis, keratitis, conjunctivitis, iridocyclitis, trabeculitis, secondary glaucoma, corneal scarring, and potential vision loss. Posterior segment disease, such as retinal necrosis, is possible but not common.
We will focus on the most common ocular manifestations of HSV reactivation, which involve epithelial keratitis (37%) and stromal keratitis (46%), as seen in Figure 1.
Evidence-based medicine: The Herpetic Eye Disease Studies
The Herpetic Eye Disease Study (HEDS I) was a multi-armed, double-blind, randomized, placebo-controlled study designed to determine the efficacy of oral acyclovir and topical steroids to treat herpetic stromal keratitis and iridocyclitis.
Similarly, HEDS II is known as the Herpetic Eye Disease Study Acyclovir Prevention Trial. This study was designed to determine the efficacy of a prophylactic dose of 400mg of acyclovir twice daily on the rate of recurrence.10 Both of these studies were instrumental in guiding our treatment protocols for anterior segment HSV-related disease.
Table 2 compares the objectives and results of HEDS I and HEDS II.13
| HEDS I | HEDS II | |
|---|---|---|
| Objectives | Assess the efficacy of topical corticosteroids with topical trifluridine in treating simplex stromal keratitis. | Evaluate whether early treatment of oral acyclovir in simplex epithelial keratitis prevents progression to stromal keratitis or iridocyclitis. |
| Measure the efficacy of oral acyclovir with topical trifluridine and topical steroid in simplex stromal keratitis. | Evaluate the efficacy of low-dose oral acyclovir in preventing herpetic recurrences in patients with previous episodes of herpetic eye disease. | |
| Evaluate the efficacy of oral acyclovir with topical trifluridine and topical steroids in simplex iridocyclitis. | ||
| Results | For stromal keratitis: Topical steroids with topical trifluridine provided faster resolution than trifluridine alone. There was no benefit to adding oral acyclovir to topical trifluridine (and topical steroid). | For the efficacy of low-dose oral acyclovir in preventing herpetic recurrences: Oral acyclovir (400mg BID x 1 year) reduced the chance of recurrence for any type of herpetic eye disease by 41%. |
| For iridocyclitis: Stopped prematurely due to recruitment difficulties. However, data suggested there is a benefit of adding oral acyclovir with a treatment regimen of topical steroids. | Oral acyclovir (400mg BID x1 year) decreased the risk of HSV stromal keratitis recurrence by 50% over 1 year post-infection. |
Table 2: Courtesy of the authors.
Notable ocular symptoms of HSV
Symptoms may include decreased vision, irritation, redness, tearing, and photophobia. Epithelial disease is usually caused by actively replicating viruses, while stromal disease is typically caused by the secondary immunologic response.
Stromal keratitis may occur in a patient with a prior history of epithelial disease. It may also occur as a primary presentation or concurrently with epithelial disease. Stromal keratitis may present with or without ulceration and may be associated with uveitis, keratic precipitates, and changes in intraocular pressure (IOP).11
Creating a distinction between actively replicating virus and the immunologic response is important because the manifestations of each etiology are treated differently.
Treating ocular manifestations of HSV
Treatment for epithelial disease includes consideration of epithelial debridement and topical or oral antiviral therapy. Topical steroids should be initially avoided on an active epithelial dendrite.
Cycloplegics can be added if there is pain, photophobia, and an anterior chamber reaction. Treatment recommendations for stromal and endothelial keratitis include topical corticosteroids and oral antivirals to prevent the reactivation of live viral particles.
Further, the treatment of iridocyclitis is similar to that of stromal keratitis, keeping in mind it is important to dilate, check for vitritis, and evaluate the retina. Aqueous suppressant IOP-lowering medications are added when treating high IOP associated with trabeculitis.
Of note, prostaglandin analogs are not recommended due to their ability to worsen inflammation and reactivate the virus.12
Table 3 lists clinical findings and treatment details for HSV keratitis.15
| Ocular Manifestation | Types | Presentation | Management |
|---|---|---|---|
| Epithelial Keratitis | Punctate, dendritic, amoeboid, and geographic ulcers | The classic dendritic ulcer: The dendrite can be central or peripheral and appears as swollen, opaque epithelial cells arranged in a tree-branching pattern with central ulceration and terminal end bulbs. | Topical antivirals: 1% trifluridine ophthalmic solution (Q2H until epithelium heals [up to 7 days]), then 4 to 5x/day, max: 9x/day, up to 21 days) or 0.15% ganciclovir ophthalmic gel (5x/day x 5 day until epithelium heals, then TID up to 7 days). |
| The edges of the ulcer (terminal end bulbs) stain with rose bengal or lissamine green, and the base stains with fluorescein. There is typically decreased corneal sensitivity. | Oral antivirals: Acyclovir (400mg 5x/day x 7 to 10 days) or valacyclovir (500mg BID to TID x 7 to 10 days) or famciclovir (250mg BID to TID x 7 to 10 days). | ||
| Note: Geographic ulcers require more aggressive treatment: Acyclovir 800mg 5x/day, valacyclovir 1g TID, or famciclovir 500mg BID x 14 to 21 days. | |||
| Stromal Keratitis | Without ulceration | Without ulceration: The epithelium is intact. Also known as interstitial or immune keratitis. Signs include stromal edema, vascularization, and scarring. | Topical steroids q1 to 2, h to QID >10 weeks, with a slow taper. |
| Disciform: Disc-shaped stromal edema due to localized endothelial dysfunction, often associated with focal keratic precipitates. | Oral antiviral cover as long as topical steroids are in use: Acyclovir 400mg BID, valacyclovir 500mg QD, or famciclovir 250mg BID. | ||
| With ulceration | With ulceration (less common): Tissue necrosis resulting in ulceration and stromal destruction with risk of melt and perforation. | Oral antiviral treatment (all x 7 to 10 days): Acyclovir 800mg 3 to 5x/day, valacyclovir 1000mg TID, or famciclovir 500mg BID. | |
| The oral antiviral is then reduced to a prophylactic dose and maintained as long as topical steroids are in use. Plus: Topical steroids BID. | |||
| Endotheliitis | Edema and folds: Edema can be disciform, diffuse, or linear and may have associated keratic precipitates and uveitis. IOP may be elevated due to secondary trabeculitis. | Topical corticosteroid agent (6 to 8 x day) with taper and oral antiviral agent: Acyclovir 400mg 3 to 5x/day, valacyclovir 500mg BID, or famciclovir 250mg BID. |
Table 3: Courtesy of authors.
Neurotrophic keratitis
A long-term complication of herpetic eye disease is neurotrophic keratitis, which is characterized by decreased corneal sensitivity and poor corneal healing. Epithelial compromise may result in infection, ulceration, and corneal perforation.
Treatment options include preservative-free lubrication, bandage contact lenses, amniotic membrane or drop derivatives, autologous serum, cenegermin 0.002%, tarsorrhaphy, conjunctival flap, keratoplasty (lamellar/penetrating) and neurotization.16
Further treatment considerations
Long-term topical antivirals may have toxic effects such as follicular conjunctivitis, cicatricial conjunctivitis, epithelial toxicity, punctal stenosis, and contact dermatitis. Oral antiviral agents have good ocular penetration, reduce corneal toxicity of topical medications, and may offer better compliance than topical medications.
Oral agents can be considered especially in patients with preexisting ocular surface disease, poor manual dexterity with drops, and for those who are immunocompromised.
To minimize recurrences, prophylactic treatment should be considered for at least 1 year. Patients who have had more than one episode of HSV keratitis and those with HSV stromal keratitis are good candidates for a maintenance course of oral antivirals. The prophylactic dosage is as follows: Acyclovir 400mg BID, valacyclovir 500mg QD, or famciclovir 250mg BID.17
Steroid treatment pearls
It is important to avoid or minimize steroids in the active replicating virus phase of a herpetic infection. Additionally, in patients using steroids, antiviral coverage is often used to prevent the recurrence of epithelial disease.
For patients with stromal disease, prolonged steroid treatment of greater than 10 weeks may be necessary. Once steroids are started, it can be difficult to wean them off. Steroids should be tapered gradually to minimize the risk of rebound inflammation.18
Final thoughts
HSV often imitates other conditions and may not always present with a classic appearance. There are many differentials to consider, such as other types of viral keratitis (varicella-zoster virus, Epstein-Barr), other forms of infectious keratitis (acanthamoeba, bacterial, fungal), immune mediated, contact lens related, and toxicity to topical medications.
Co-management with a cornea specialist is warranted in certain cases, such as in impending corneal perforation. Retinal consultation is crucial when viral retinitis is suspected from HSV, HZV, or cytomegalovirus.
It is important to consider herpes if a patient is in less pain than what the clinical findings reveal. Suspect herpes if a patient is photophobic or has uveitis and high IOP. Finally, it is important to suspect a recurrent herpes infection when a patient has a prior history of herpetic eye disease.

