



Autologous serum eye drops—sometimes called serum tears—are drops made from a patient’s own blood. First described in 1984 by Fox et al. as a treatment for keratoconjunctivitis sicca and then reintroduced and popularized by Tsubota et al. in 1999 as a treatment for epithelial disorders associated with Sjögren’s syndrome-related dry eye, serum tears have been used in the treatment of ocular surface disease for over 30 years.1-2
Overview of autologous serum eye drops
Blood serum has a similar pH and osmolarity to natural human tears, but includes a higher concentration of the following:
- Epidermal growth factor (EGF)
- Vitamin A
- TGF-β
- Fibronectin
- Cytokines
- Lysozyme
- Nerve growth factor (NGF)
Note: Serum also has a much lower concentration of surface immunoglobulin A (SIgA).3-4
With a similar or higher concentration of growth factors, serum tears are believed to address the lack of epitheliotrophic elements in dysfunctional tears (which contribute to epithelial defects) while promoting wound healing as well as lubrication of the ocular surface.1-4
Specifically, nerve growth factor—which aids in the regeneration of corneal nerves—is present in higher concentrations in serum than in natural tears, and has been shown to support symptom relief and nerve regeneration in patients suffering from neuropathic corneal pain.5,8-9
Producing autologous serum drops
To create autologous serum eye drops, blood must first be collected from the patient and screened for bloodborne pathogens, which might render it incompatible for processing. After the sample is confirmed as suitable, it is permitted to clot for a period of 30 to 120 minutes, then centrifuged for 5 to 15 minutes at 1500 to 3000g until the serum is separated.3-4
The serum is then diluted to 20 to 100% with a saline solution or other diluent and then dispensed to the patient with instructions for storage and application. All processing must be completed in a sterile environment in order to prevent contamination, as the solution is generally devoid of preservatives. For this reason, serum tears must be maintained in a frozen (or at minimum refrigerated) state for a period of no longer than 3 months.
As Geerling et al. noted in a 2004 paper proposing a standard operating procedure (SOP) for the production of autologous serum drops, these ranges in the production process tend to be quite wide compared to other manufacturing processes since there is no existing SOP for the production of autologous serum drops.3
Clinical evidence for autologous serum drops
Several systematic reviews of the literature have identified case-control and cohort studies as well as case series and case reports directed toward the efficacy and safety of serum tears.6,10-12
Geerling et al. found in their review of the literature that serum tears showed efficacy in treating severe dry eye and superior limbal keratoconjunctivitis, with 20 to 100% efficacy for symptomatic relief, 39 to 61% efficacy for reduction of fluorescein staining, and 33 to 68% for improvement in rose bengal positive epitheliopathy.
Additionally, there is some evidence for the use of serum tears in the treatment of recurrent corneal erosion syndrome and persistent epithelial defects, and as an adjunct treatment for ocular surface reconstruction.3
The 2020 Ophthalmic Technology Assessment for the American Academy of Ophthalmology (AAO) found that out of 13 studies, all noted improvement in at least one sign.6 Similarly, other recent systematic reviews have found that serum tears have few adverse effects and perform similarly to artificial tears in practice, although Pan et al. noted that there was inconsistent evidence of improvement after more than 2 weeks of use.10-12
As a blood product, serum tears are not regulated by the US Food and Drug Administration (FDA), but individual states may have separate regulations that could affect production.6
Who is the right candidate for autologous serum drops?
The primary indications for the use of autologous serum tears include:3-4,6
- Moderate to severe dry eye disease, often recalcitrant to other treatments
- Diffuse superficial punctate keratitis with severe inflammation
- Persistent non-healing epithelial defects
- Non-infectious corneal ulceration (e.g., neurotrophic keratitis, chemical injury, etc.)
- Drug or preservative toxicity that prohibits the use of artificial tears or other commercially available therapies
While patients with severe dry eye are traditionally the primary candidates, serum tears can be used for patients with a wide spectrum of dry eye, from those who have failed conventional treatments like artificial tears, topical immunomodulators, lid hygiene, or neuroactive nasal sprays.
Similarly, patients with autoimmune-related ocular surface disease, such as those with Sjögren’s syndrome, rheumatoid arthritis, or those undergoing chemotherapy or treatments with biologic agents and have developed corneal disease as a result of those treatments, are prime candidates for serum tears.2,7
Another group of patients who often benefit from serum tears are those with neurotrophic keratitis, graft versus host disease, limbal stem cell deficiency, and patients with neuropathic corneal pain.5,8-9
Finally, perioperative cataract or corneal surgery patients may benefit from serum tears, particularly in those individuals who have undergone laser-assisted in situ keratomileusis (LASIK)/photorefractive keratectomy (PRK) or corneal crosslinking with non-healing epithelium.13
Contraindications for autologous serum eye drops
There are no documented contraindications for the use of autologous serum. Clinicians may need to consider not using serum tears in patients with poor tolerance of blood draws, poor venous access, or low blood counts.14 For example, in patients with hematologic conditions, clinicians should work with the patient's hematologist/oncologist to help decide if blood draws for serum tears can be performed.
Some settings that prepare serum tears follow blood-donor guidelines that disqualify certain patients from supplying their own blood for serum tears; however, all settings preparing serum tears should practice universal precautions when drawing and processing blood and serum.
When is the right time to initiate treatment?
The 2017 Tear Film & Ocular Surface Dry Eye Workshop II (TFOS DEWS II) report categorizes autologous serum drops as a third-line treatment, to be used when first- and second-line therapies fail.15
However, as dry eye treatment and management turn towards an “interventional” approach, many practitioners are bringing in therapies that were historically considered as “last resorts” much earlier in the treatment protocol.16
In certain cases, a practitioner might consider including serum tears as a first-line treatment rather than waiting for other therapies to fail, particularly when treating a patient with neurotrophic keratitis or keratitis in the setting of autoimmune conditions for whom serum may be especially effective.
Proper dosing of autologous serum tears
The most common concentration of serum tears found in the literature is 20%,3 but concentrations can range from 20 to 100%. However, much depends on the clinician's preference; some like to start at 20% QID or more, while others prefer to start at 40% QID or more and then adjust based on the individual patient’s response. A common dosing schedule is four times per day,4 but some will go as high as eight.3
![Gray box with a headshot of Dr. Venkateswaran next to text that states: "When I see a patient with more symptomatology, I will mention higher concentrations than the initial 20 to 40% dose. For my cataract surgery patients who may only have a few weeks to prep their ocular surface, I will often reach for a higher percentage—say, 50% [concentration]—because I have seen it work more quickly. However, there’s evidence that at higher percentages, the serum contains a higher concentration of TGF-β1, which may inhibit healing."](/_next/image/?url=https%3A%2F%2Fcdn.sanity.io%2Fimages%2F51cpf7jm%2Fproduction%2Fa4fae1171258810e249fab04d96a3ab1a570792e-1200x628.png&w=3840&q=75)
How to access autologous serum drops
In the last 5 years, it has become much easier to access serum drops than it was a decade or more ago. Prior to 2015 or so, the major barrier to utilizing serum tears in dry eye treatment and management was one of simple access.
Serum drops can be prepared by blood banks, eye banks, or any appropriately equipped laboratory (e.g., with a centrifuge and the other necessary equipment) with sterile work areas, such as compounding pharmacies.
But for some patients, the hassle of finding one of these facilities made serum tears a less than appealing option. Exacerbating the problem, many community-based compounding pharmacies do not delve into the area of ophthalmic preparations.
The company Vital Tears is another option, providing services for ordering, producing, billing, and shipping serum tears in various concentrations. While serum tears are rarely covered by insurance—although some plans will reimburse if patients submit a claim—the service offers serum tears in three- and six-month supplies with costs averaging $130 per month. However, the amount of time the supply will last depends on the concentration and dosing of the prescription.
Scheduling follow-ups and when to expect results
As with any dry eye treatment protocol, the efficacy of serum tears for a particular patient’s condition can be assessed on a regular follow-up schedule. For some, this means following up at 3 months, while others may prefer to have patients come in earlier.
On follow-up, the primary things to look for are decreased inflammation, conjunctival injection, corneal staining, and punctate staining—the full dry eye workup. Additionally, we’d like to see improvements in visual acuity and the response to a validated dry eye questionnaire (e.g., Ocular Surface Disease Index [OSDI], Standard Patient Evaluation for Eye Dryness [SPEED], or Dry Eye Questionnaire 5 [DEQ-5]).
Some patients may stay on serum tears for the long term, especially if they were initially prescribed due to autoimmune conditions or neuropathic pain. Patients who were prescribed serum tears for dry eye flares or as a post-operative dry eye regimen may find that they can taper off the serum tears once they have reached a successful outcome.
Case reports on autologous serum eye drops
Case report 1
Patient presentation
From Dr. Venkateswaran: A 70-year-old male presents with blurred vision and pain, saying, “I just can’t open my eyes.” Patient history revealed metastatic cholangiocarcinoma treated with multiple chemotherapeutic agents, including cisplatin, gemcitabine, durvalumab, and tepotinib.
The patient had previously tried:
- Punctal plugs
- Lipiflow
- Intense pulsed light (IPL) therapy
- Topical steroid drops and ointment
- RESTASIS (cyclosporine ophthalmic emulsion 0.05%) TID
- Regener-Eyes TID
- Tears Q1 to 2H
The patient had felt improved when using PO prednisone for cancer.
Ophthalmic examination
- Best-corrected visual acuity (BCVA)
- 20/25-2 OD
- 20/30-1 OS
- Telangiectatic lids
- Rapid tear breakup time (TBUT) and keratopathy
Treatment plan
We initiated treatment with serum tears 40% 6x/day OU, as well as the following:
- Tyrvaya (varenicline solution nasal spray) BID
- XIIDRA (lifitegrast ophthalmic solution 5%) BID OU
The patient was advised to continue the Lotemax (loteprednol etabonate) ophthalmic ointment QHS OU, use the serum tears frequently, and start warm compresses.
Follow-up
Follow-up occurred at 2 months, and the patient showed significant symptomatic improvement. BCVA was stable, and the patient said that he felt the serum tears had made a big difference.
Case report 2
Patient presentation
From Dr. Dang: A 40-year-old Asian female presented with severe dry eye with a history of filaments OS. Her past medical history included systemic lupus erythematosus, and her ocular history included the aforementioned filamentary keratitis, neurotrophic keratitis, and ongoing keratoconjunctivitis sicca.
She had undergone the following procedures and treatments:
- Lipiflow
- TearCare
- IPL series
- XIIDRA
- Regener-Eyes
- Oxervate (cenegermin-bkbj ophthalmic solution) x 8 weeks
- Alrex (loteprednol etabonate ophthalmic suspension) 0.2%
Her current medications included:
- Hydroxychloroquine 200mg BID
- Tyrvaya BID
- 20% autologous serum QID OU
Ophthalmic examination
Figures 1 and 2 highlight slit lamp images OS before autologous serum (top) and OS with filament before autologous serum (bottom).

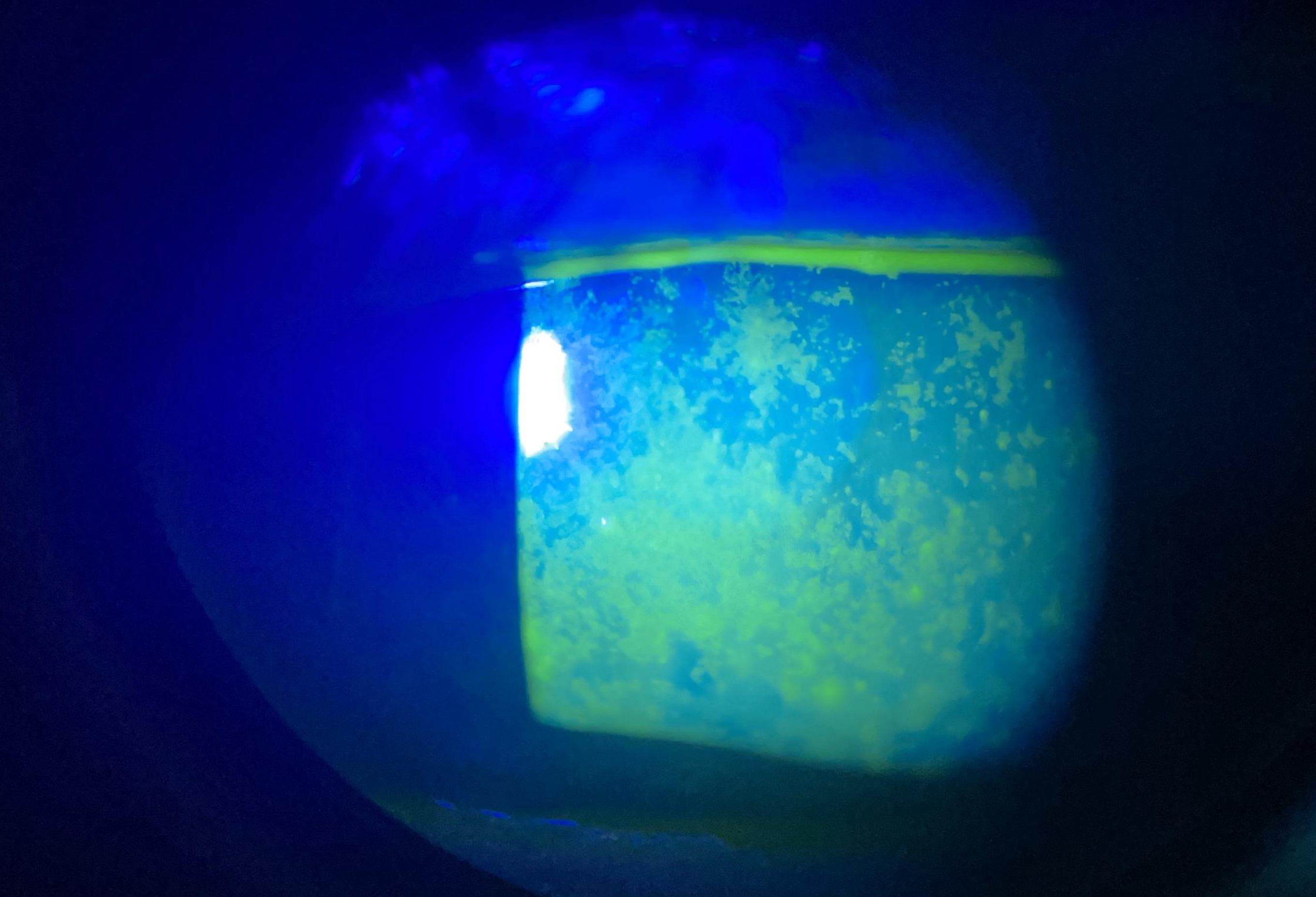

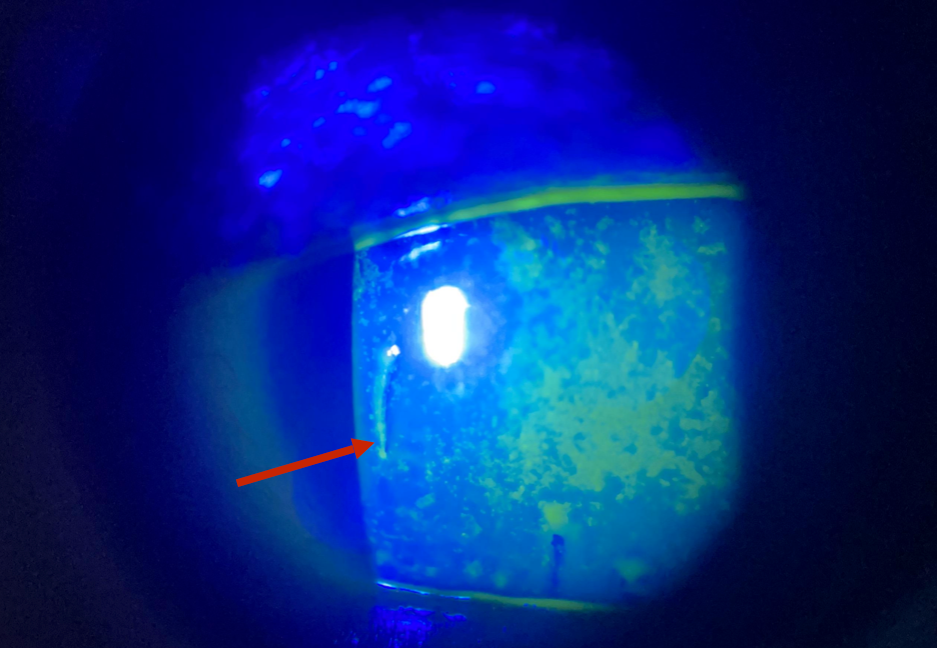
Figures 1 and 2: Courtesy of Vin Dang, OD, FAAO.
Treatment plan
We increased the concentration of her serum tears from 20% to 50% for an improved surface.
Follow up
Figure 3 demonstrates a slit lamp image OS after initiating autologous serum treatment.

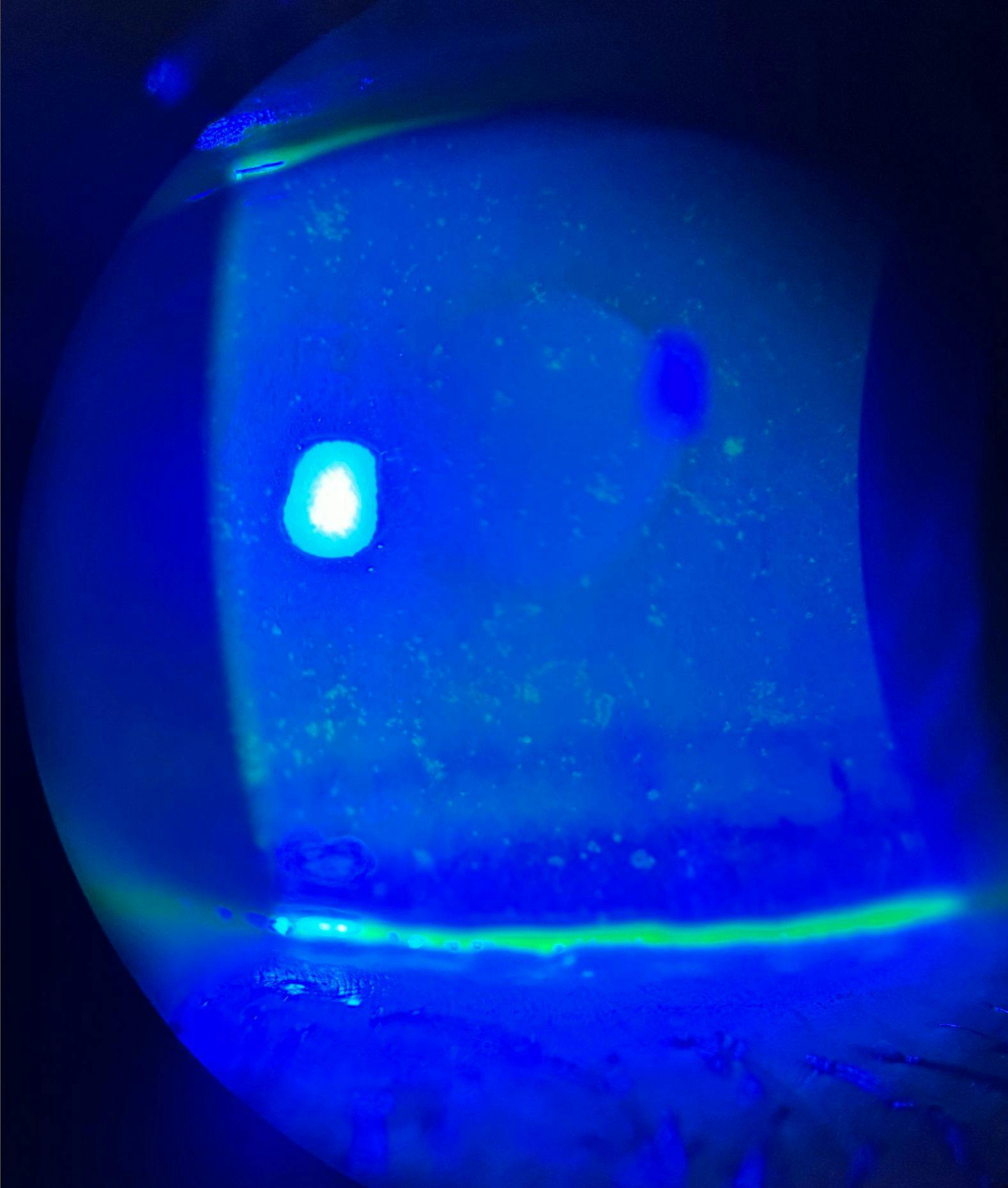
Figure 3: Courtesy of Vin Dang, OD, FAAO.
Patient communication
Because serum tears are rarely covered by insurance, some patients may be unsure about the benefits versus the cost of the treatment. Patients also require being informed of the experimental nature of this treatment along with the FDA approval and insurance status in order to receive informed consent to the treatment.
The conversation in this case might go something like this:
“Ocular surface disease is chronic, and there’s no magic bullet. What we’re looking for right now is something that can help you have more good days than bad ones, and I think that, in your case, this treatment is worth trying. It’s made from your own blood, so it’s designed to mimic what is present in your own natural tears.
I’d like you to try your best to use it daily. Since it’s made out of your blood, the FDA can’t approve it, so insurance won’t cover it—but think of it as an investment in your eyes. If you try it for a few months and don’t feel like it’s working, we’ll try something else—but give it a shot and we’ll see how it goes.”
Conclusion
Accessing serum tears is no longer the barrier to entry that it used to be a few decades ago—for patients or practitioners.
With few adverse effects or contraindications, serum tears are a useful tool for eyecare practitioners seeking to offer customized dry eye treatment and management.
