The global prevalence of
cataract surgery is estimated to be 17.2% across all age groups, and cataract surgery is a cost-effective treatment with substantial positive socioeconomic effects.
1 Nonetheless, the material risk for vision loss exists with an annual pseudophakic retinal detachment (PRD) incidence between 0.04 and 0.25%.
2 Investigators have identified numerous risk factors for PRD, including
posterior capsular rupture, patients younger than 65 (compared to older age groups over 75 years), male gender, and
high myopia.
3Spotlight on the age-related risk factor for PRD
The PRD risk factor related to younger age has been challenging to elucidate fully despite it conferring a relatively high risk in these patients. However, the literature reveals an incidence of 3.55% in patients less than 62 years of age.4
Risk stratification by age reveals a PRD incidence of 2.44% when considering patients aged 55 to 60; this PRD risk is significantly higher at 5.39% in patients 50 to 54 years of age.4,5 In this younger cohort, axial length and myopia significantly modulate PRD risk, but the pathogenic mechanism remains unresolved.
This article will highlight the importance of risk mitigation in younger patients undergoing cataract surgery; we will report on an atypical PRD involving posterior insertion of the vitreous base (PIVB) with subsequent zipper-like retinal tears.
Case report
A 59-year-old healthy male presented with a macula-off rhegmatogenous
retinal detachment after early cataract surgery OD. Best-corrected visual acuity (BCVA) measured 20/400 OD and 20/25 OS, and intraocular pressures were within normal limits OU.
Dilated fundus examination of the right eye revealed a posterior vitreous detachment and zipper-like retinal breaks in the periphery associated with PIVB. Note the patient had no posterior vitreous detachment before
cataract surgery.
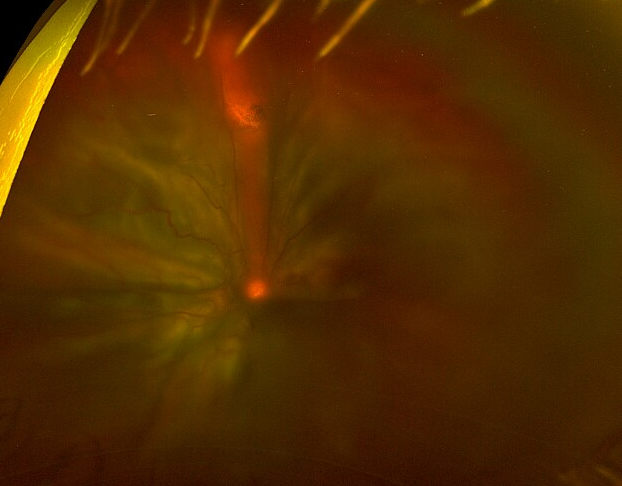
As seen in Figure 1, the right eye demonstrated pseudophakic retinal detachment associated with posterior insertion of the vitreous base and numerous retinal tears in a zipper configuration. The patient had subsequent retinal re-attachment surgery using primary pars plana vitrectomy with intraocular gas tamponade; the resultant visual acuity was 20/50 in the operative eye OD.
Figure 1 is a widefield color fundus photograph of the patient who presented with a pseudophakic macula-off rhegmatogenous retinal detachment after early cataract surgery.
Figure 1: Image courtesy of David RP Almeida, MD, MBA, PhD
Figure 2 is a widefield color fundus photograph demonstrating the posterior insertion of the vitreous base and numerous retinal tears in a zipper configuration.
Figure 2: Image courtesy of David RP Almeida, MD, MBA, PhD
Discussion of PRD with zipper syndrome
Though cataract surgery techniques continue to improve with reduced incision sizes,
femtosecond laser-assisted phacoemulsification, and improved refractive outcomes, the rising numbers of cataract operations in younger patients contribute to an increase in PRD.
The relationship between a posterior vitreous detachment and PRD
Indeed, younger age is a well-known risk factor for PRD, and informed consent documentation of PRD is necessary.
Our case illustrates the need to recognize two critical aspects that may have an outsized effect on the risk of PRD in young patients: the absence of a posterior vitreous detachment (PVD), i.e., the presence of vitreomacular adhesion, and PIVB appear to contribute to PRD significantly.
In younger patients, native vitreous with vitreomacular adhesion can cause a forceful PVD, which occurs after
cataract surgery. The PVD proceeds in a temporal symmetric fashion in this scenario with pathogenic vitreoretinal traction. Counseling these patients on the symptoms and signs of PVD—and possible retinal tear and detachment—is of utmost importance to ensure early triage and assessment when warranted.
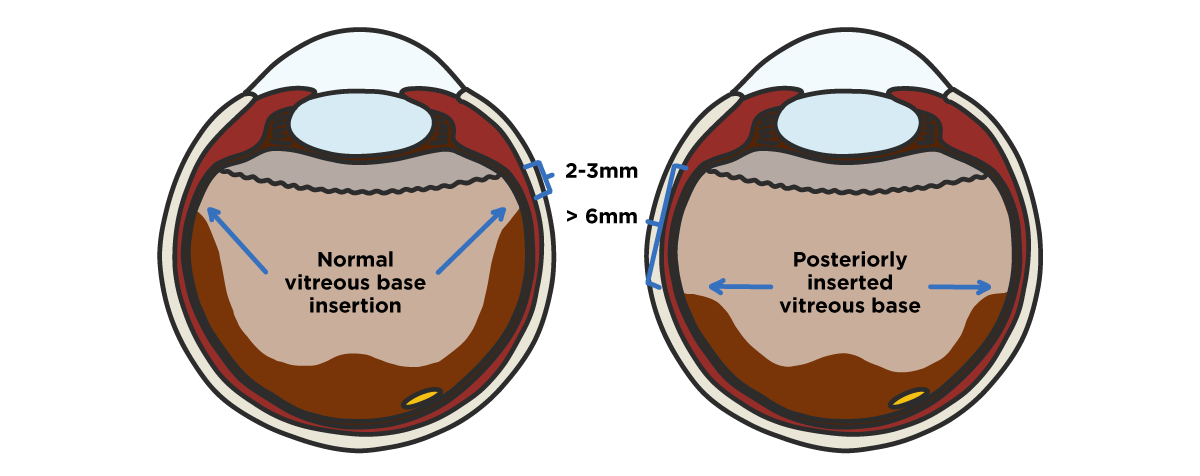
Figure 3 is a schematic diagram that shows regular and posterior insertion of the vitreous base anatomy. The left eye depicts normal vitreous base insertion 2 to 3mm posterior to the ora serrata. The right eye represents a vitreous base inserted posteriorly, over 6mm posterior to the ora serrata.
Figure 3: Image courtesy of authors
The relationship between posterior insertion of the vitreous base and PRD
PIVB is defined as the insertion of the posterior hyaloid membrane located posterior to the vortex veins.
6 Any eye undergoing
cataract surgery or vitrectomy may have PIVB. Still, those with a high number of retinal breaks and lattice degeneration near the equator may be at the highest risk.
6 In eyes with PIVB and pathogenic (i.e., vitreoretinal traction) PVD, observable vitreoretinal interface abnormalities predispose to numerous retinal breaks along the vitreous base.
This can result in the rapid evolution of PRD, namely progression from macula-on to macula-off status, with a greater likelihood of irreversible vision loss despite successful retinal re-attachment surgery.
Our case exemplifies the risks of PRD in younger patients undergoing
cataract surgery, particularly given the propensity of zipper retinal breaks and detachments in younger patients. When identifying these younger patients at the highest risk for PRD, the ophthalmologist must consider the complicating clinical features of PIVB in the setting of no previous posterior vitreous detachment.
Key takeaways
It is essential to acknowledge the material risk of PRD in younger patients undergoing cataract surgery to mitigate vision loss in this population and realistically detail the
benefits and risks of surgery. Moreover, with increasing rates of cataract surgery in younger patients in the setting of refractive surgery, there is a need for clear and facile communication when co-managing these patients.
Dialogue between eyecare professionals, including
optometrists,
comprehensive ophthalmologists, anterior segment ophthalmologists, and vitreoretinal subspecialists, allows for the appropriate counseling on these relevant risks before cataract surgery.