To a patient, the pupil is a window opening them to a view of the world. For optometrists, the
pupil is a window of insights about the autonomic nervous system. Though checking pupillary function is second nature to us in the exam room, it is crucial that we, as healthcare providers, remain watchful of abnormal function.
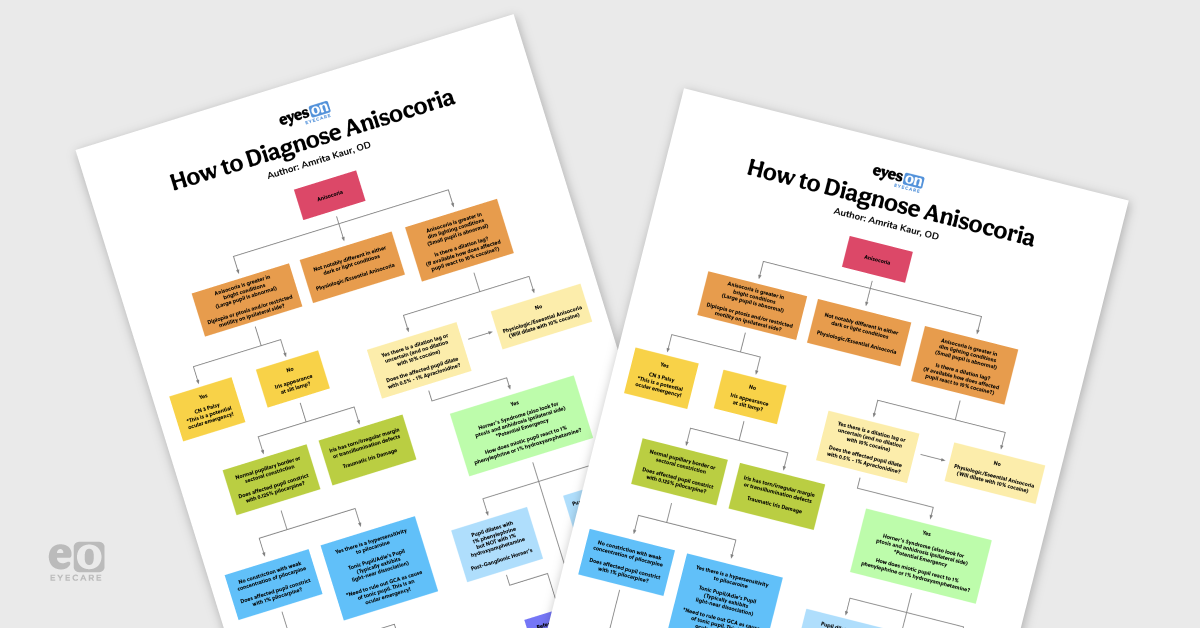
Anisocoria, by definition, is a condition in which the pupils in each eye are different sizes. The etiology is widespread ranging from a normal physiologic variant to potential life-threatening conditions.1 This flowchart and concurrent article aim to help streamline the clinical thinking process when presented with anisocoria in the exam room.
Note that this chart serves merely as a guide for common diagnoses associated with the clinical conditions mentioned. The causes of anisocoria are vast and may present with atypical diagnosis or symptoms. When using this guide, be sure to use your best clinical judgment on a case-by-case basis.
Brief Physiology Review
Recall that pupil function and size change is a tug of war between sympathetic and parasympathetic fibers. The iris dilator muscle has sympathetic innervation and the iris sphincter muscles (as well as oculomotor nerve) have parasympathetic innervation.1-3
When the sympathetics are damaged, the parasympthatically innervated sphincter muscle action becomes dominant which creates a miotic pupil on the affected side. Oppositely, when the parasympathetic function is damaged, the dilator muscle takes over which results in mydriasis on the affected side.1-4 Lesions along either pathway or damage to the iris sphincter itself can lead to anisocoria.1,2
Assessing the Patient
Once you have determined that a patient has unequal pupil sizes, we need to determine the cause of this difference. First note the relative size of the pupils in dim and light conditions. If the pupils are different sizes, but react equally to light-meaning the amount of constriction and dilation change between the two pupils is the same, the presenting patient likely has physiologic, or essential, anisocoria.3,5
Physiologic anisocoria is a benign form of anisocoria that exists in about 20% of the population.5 The difference in pupil diameter between the two eyes is generally small in this case (≤1mm) and exists in both dim and light conditions. These patients should have a strong pupillary light response, no dilation lag, and no associated ptosis.5
Download the flowchart now!
Download the Anisocoria Flowchart!
This colorful and comprehensive flowchart is 100% free!
Pathology Associated with Anisocoria
While the most common type of anisocoria we encounter is physiologic, we have to be very careful to ensure that no further workup is warranted. Pathologic anisocoria has the potential to be an element of a life threatening condition.
As mentioned, pathologic anisocoria can be the result of both an abnormally dilated pupil (parasympathetic damage) or abnormally constricted pupil (sympathetic damage).
Anisocoria Greater in Bright Light Conditions
If the anisocoria is greater in bright conditions or lighting, the large pupil is the abnormal pupil.
When a dilated pupil also presents with a ptosis, diplopia, or restricted motility on the ipsilateral side, you must immediately rule out a cranial nerve 3 palsy (CN 3 palsy). This is a potential ocular emergency!
A complete
cranial nerve 3 palsy presents with a dilated pupil, ptosis, and the ipsilateral eye will be positioned downward and outward. However, not all CN 3 palsies are complete. If a patient presents with any of these symptoms, a CN 3 palsy needs to be ruled out.
3,6,7Only a complete CN 3 palsy enables us to use the pupil as a guide. If the pupil is dilated with a complete palsy, this is likely an aneurysm and needs an immediate referral to the ER for imaging and treatment. If the pupil is spared in a complete CN 3 palsy, it is likely due to vasculopathic factors. If the CN III palsy is incomplete, you cannot use the pupil as a guide and must treat it as an aneurysm until proven otherwise. In any cases of uncertainty, always refer for prompt imaging.6-8
If the dilated pupil has no associated ptosis, diplopia, or restricted motility, your next step is to evaluate the patient’s iris appearance in the slit lamp. If there are signs of iris damage such as transillumination defects or an irregular or torn iris border, consider traumatic iris sphincter muscle damage as a cause of the anisocoria. This includes not only blunt trauma, but also ocular surgery. Traumatic iris damage may also exhibit sluggish near constriction.3,9
If the iris is normal or has signs of sectoral iris paralysis (but no other signs of damage), our next step is to examine how the mydriatic pupil will react to the instillation of pilocarpine ophthalmic drops.
In efforts to see if the patient exhibits a denervation hypersensitivity of the iris sphincter, a weaker concentration of pilocarpine (a cholinergic agent) is first instilled (0.125%). A tonic pupil will constrict with the weak concentration of pilocarpine, whereas a normal pupil will not.2,3
Tonic pupils often result from orbital lesions (ciliary ganglion or short posterior ciliary nerves) so they will likely also exhibit light-near dissociation and sectoral iris paralysis. Known causes of tonic pupils include trauma, viral infections, paraneoplastic syndromes, and
giant cell arteritis (GCA).
Most tonic pupils, however, are idiopathic. When there is no known cause, they are referred to as Adie’s tonic pupil.2 Note that for a very acute tonic pupil, there may not yet be hypersensitivity to the weaker concentration of pilocarpine, but there will be constriction with 1% pilocarpine.3 A CN 3 palsy will also dilate with 1% pilocarpine but not 0.125% pilocarpine. If there is no constriction of a dilated pupil with either concentration of pilocarpine, suspect a pharmacologic dilation.2,3
Anisocoria Greater in Dim Lighting Conditions
If the anisocoria is greater in dim or dark conditions, the constricted pupil is the abnormal pupil.
When there appears to be a strong light reaction in both eyes, but the smaller pupil fails to dilate to the extent of the larger pupil, we have to ask is there actually a dilation lag? If there is no dilation lag, and the difference in size between the two pupil diameters remains constant in both dim and light conditions, the patient likely has physiologic anisocoria.
This can be confirmed with pharmacologic testing. If the pupil in question dilates with 10% cocaine drops, it is a normal pupil. Cocaine drops are often not readily available, so more often 0.5%-1% apraclonidine is used. A normal pupil will NOT dilate with apraclonidine.2,3,11
A constricted pupil associated with
Horner’s Syndrome, however, will dilate with apraclonidine, but not with 10% cocaine. Horner’s Syndrome is a neurologic condition that also presents with partial ptosis of the upper lid, and anhidrosis (absence of sweating) on the ipsilateral side of the miotic pupil.
11-13We can further classify a Horner’s pupil with additional pharmacologic testing. To avoid any drug interactions, ample time (at least 24 hours) needs to pass before instilling any other pharmacologic agents once apraclonidine or cocaine drops have been used.3
If the miotic pupil dilates with 1% hydroxyamphetamine, we can classify this as a Horner’s Syndrome with a preganglionic or central lesion. A preganglionic or central lesion will NOT, however, dilate with the instillation of 1% Phenylephrine. A Horner’s syndrome associated with a postganglionic lesion will display the opposite responses. If the Horner’s pupil dilates with 1% Phenylephrine, but NOT with 1% Hydroxyamphetamine, it is a post ganglionic Horner’s syndrome.11-13
While we have the ability to classify a Horner’s pupil into pre vs post-ganglionic, it may not be a priority in our office.
A sudden onset or painful Horner’s has the potential to be another ocular emergency, including but not limited to causes such as carotid artery dissection or aneurysm, thrombosis, malignant tumors or metastasis, Pancoast tumor, intracranial hemorrhage, cerebral vascular events, or encephalitis.12,13
These patients need to be referred for workup and imaging immediately to rule out life threatening conditions.3
Other causes of anisocoria due to miotic pupils include unilateral exposure to a miotic agent, iritis, Argyll Robertson pupils, or longstanding Adie’s Pupil (initially dilated but may constrict when longstanding). Note that Argyll Robertson pupils are bilaterally miotic, but may still present with aniso no coria.3
Hopefully this has been eye opening (and constricting) knowledge for you, and you feel ready to tackle your next case of anisocoria!