



As a busy, new optometrist, I value having a quick reference guide with everything I need to know all in one place. That’s exactly what our 1,2,3’s series is for. We’ll take a common clinical scenario and break it down to hit all aspects, all at once: how to diagnose, how to manage, and how to bill.
So let’s start with a common clinical condition: Plaquenil (aka hydroxychloroquine) retinopathy.
1. Diagnose the hydroxychloroquine retinopathy
Chances are a patient will present to you from their primary care physician (PCP) or rheumatologist prior to, or just after, starting their new medication: brand name Plaquenil or generically known as hydroxychloroquine (HCQ).
It’s vital that we screen for any associated toxicity. Why? Two reasons: If damage occurs, (1) it is irreversible, and (2) we can do something to stop it.
Prevalence of HCQ retinopathy
First, we need to understand some key principles regarding hydroxychloroquine retinopathy. Let’s start with the prevalence, aka the likelihood, that said condition (HCQ retinopathy) will occur.
When dosed appropriately, HCQ retinopathy is rare. The incidence is <1% within 5 years and <2% within 10 years of use. However, it can rise to almost 20% after 20 years of use.
The mechanism of action of hydroxychloroquine
The hydroxychloroquine molecule binds strongly to melanin and melanocytes. In the RPE, lysosome activity is inhibited, thereby reducing outer segment photoreceptor phagocytosis.1
This results in the accumulation of these toxic photoreceptors leading to RPE degeneration and migration of damaged cells into the outer retinal layers.
Ocular manifestations
Hydroxychloroquine can manifest in corneal limbal stem cells, which can be visualized under slit lamp examination as corneal verticillata or “whorl keratopathy.” Conversely, in the posterior segment within the retinal pigment epithelium, it can be identified by the hallmark “bull’s eye maculopathy.”
Additional bull’s eye maculopathy differentials include rod-cone dystrophy, Stargardt disease, benign concentric annular macular dystrophy (BCAMD), and macular telangiectasia type 2 (MacTel Type 2).
Testing for hydroxychloroquine retinopathy
In 2018, The Royal College of Ophthalmologists (RCOphth) published an expansive review of the literature to suggest best practices for testing and management of HCQ retinopathy.2 Here are some of the key takeaways along with my personal takes on their recommendations.
Baseline testing
According to RCOphth, as well as preferred practice patterns set forth by the American College of Rheumatology (ACR), American Academy of Ophthalmology (AAO), American Academy of Dermatology (AAD), and Rheumatologic Dermatology Society (RDS), there is no recommended “baseline testing.” Rather, routine testing should begin AFTER 5 years of HCQ use.3
Therefore my “baseline exam” includes the imaging and testing modalities listed below.
Medical record review with documentation of:
- Current dose of hydroxychloroquine
- Real body weight (kg)
- Duration of treatment
- Concomitant tamoxifen therapy
- Impaired renal function (eGFR <60mL/min/1.73m2)
- Chloroquine use
Dilated fundus examination:
The primary purpose is to screen for additional retinal pathologies: macular degeneration, diabetic retinopathy, or hereditary disorders of retinal function. Fundus findings won’t occur in early HCQ retinopathy, but if present you’ll see a ringed pigment pattern that spares the central fovea.
Annual testing:
I personally prefer having baseline testing for comparative purposes and have even incidentally found normal tension glaucoma (NTG) in an otherwise unsuspected patient. Otherwise, these are the most essential tests to be performed at annual monitoring.
Figures 1 and 2 are visual field analyses conducted on a patient with hydroxychloroquine retinopathy.

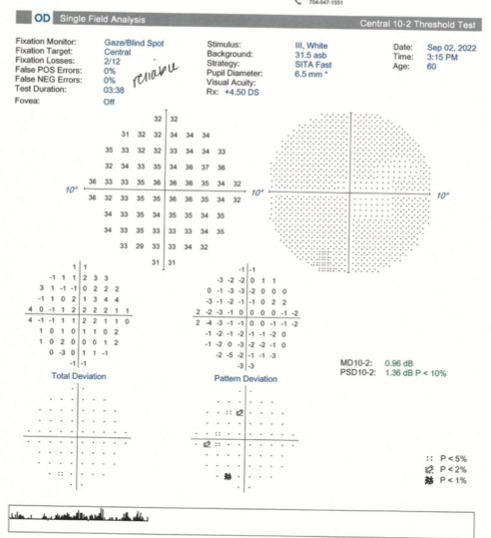
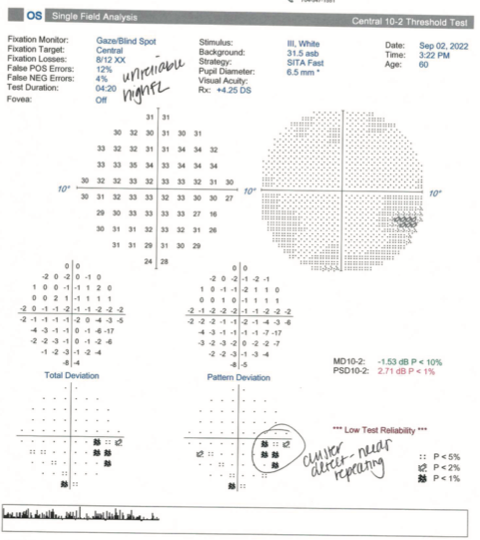
Figures 1 and 2: Courtesy of Emilie Seitz, OD.
Widefield fundus autofluorescence (FAF):
Hyperautofluorescence is a sign of excess lipofuscin from abnormal metabolism of outer segment photoreceptors and inadequate phagocytosis. Increased signals of hyperautofluorescence is indicative of early stages of HCQ retinopathy.1 Decreased signals of hypoautofluorescence is indicative of RPE cell death, more correlated in advanced stages of HCQ retinopathy.5
Spectral-domain optical coherence tomography (SD-OCT):
- Radial scan or HD Raster: The foveal sparing, degradation of outer photoreceptors and RPE, and migration of cells account for the appearance of the parafoveal “flying saucer sign” seen on OCT. Studies have found that Asian populations have a higher propensity of pericentral retinopathy (50%) than Caucasian patients (2%), which may support wider screening methods, like a 21-line Raster.4
- Ganglion cell analysis (GCA): There are some studies that suggest selective thinning to the inner ganglion cell layer (GCL) and inner plexiform layer (IPL) may precede structural change to the outer retinal layers or RPE in patients with chronic HCQ use (>6 years).6
Figures 3 and 4 are a GCA OU and 5-line raster optical coherence tomography (OCT) scan, respectively, on a patient with HCQ retinopathy.
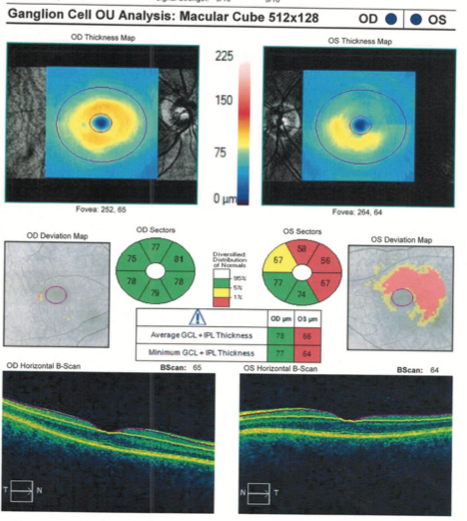
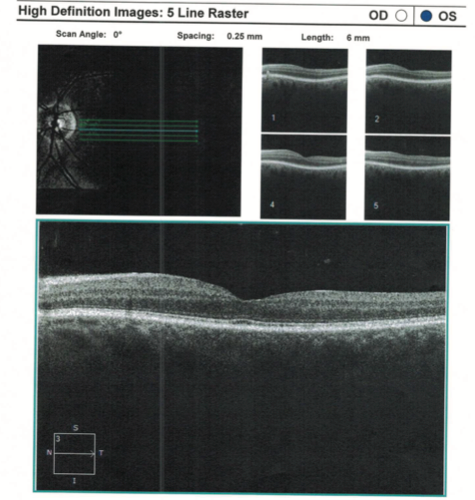
Figures 3 and 4: Courtesy of Emilie Seitz, OD.
Additional testing:
- Visual field testing: Most clinicians will incorporate visual field testing into their annual protocol; however, most guidelines recommend deferring due to the poor reliability of visual fields, taking into consideration OCT’s high specificity for detecting toxicity.
- The following visual field tests can be valuable if abnormalities are detected in complementary imaging studies from OCT/FAF1,7:
- 10-2 central visual field: Focusing on the central 10 degrees of retina and looking for ring scotomas.
- 24-2 or 30-2 pericentral: In East Asian patients, focusing on broader visual fields to match pericentral defects.
- The following visual field tests can be valuable if abnormalities are detected in complementary imaging studies from OCT/FAF1,7:
- Multifocal electroretinogram (ERG): Demonstrate decreased signal centrally and paracentrally.
Figures 5 and 6 are an optic nerve head (ONH) and retinal nerve fiber layer (RNFL) analysis OU and a visual field analysis OS, respectively, of a patient with HCQ retinopathy. Follow-up testing reveals a defect more consistent with normal tension glaucoma (NTG).
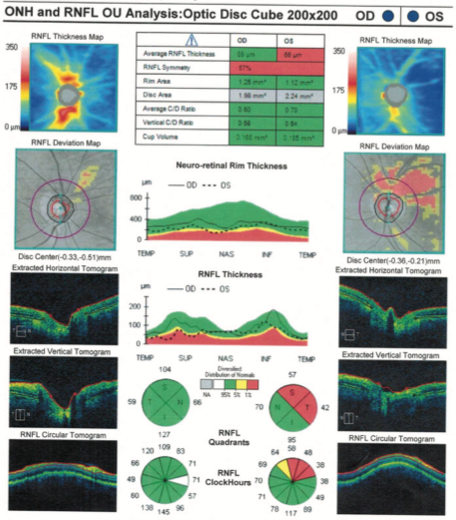

Figures 5 and 6: Courtesy of Emilie Seitz, OD.
Not to test:
According to AAO clinical guidelines, fundus photography, Amsler grid, and color vision testing are no longer recommended due to their inability to detect early changes.
However, if FAF is inaccessible, a weak case could be made for fundus photography (92250) at the patient’s baseline exam to screen for pre-existing retinal disease with poorer support for inclusion in annual testing.8
2. Manage the HCQ retinopathy
We talked in depth about how to screen, let’s review WHEN to do it. Co-management should include letters back to the referring provider.
- Remember the 5x5 rule: Start annual testing after 5 years, 5mg/kg of real body weight
- Monitor annually right away if additional high-risk factors are in play:
- Current dose of hydroxychloroquine exceeds >5mg/kg/day
- Patient presents with a duration of treatment >5 years
- Concomitant tamoxifen therapy
- Impaired renal function (eGFR <60mL/min/1.73m2)
- Chloroquine use
Download the referral letter template to a rheumatologist or PCP here!
How would I approach a change?
If a patient exceeds the daily dose WITH retinopathy I would request the patient stop immediately. A small multicenter, retrospective study of older patients (>55 years old) with systemic lupus erythematosus (SLE) supported that HCQ discontinuation did not significantly increase flares.9
If a patient exceeds the recommended daily dose (>5mg/kg) WITHOUT retinopathy, the patient and referring provider should be informed that there is statistically a 10% risk of retinopathy in 10 years and 40% risk after 20 years. I do not stop their medication but typically call the referring provider along with sending a summarized report.
3. Bill hydroxychloroquine retinopathy (screening)
Diagnosis codes for HCQ retinopathy:
There are two key parts to billing for your screening services. It is necessary to have both components and link your testing to both ICD-10s when applicable.
- Medical diagnosis associated with their disease state:
- Systemic lupus erythematosus, organ or system involvement unspecified (M32.10)
- Rheumatoid arthritis, unspecified (M06.9)
- Sjögren syndrome (M35.0)
- Plaquenil use: Other Long Term (Current) Drug Therapy (Z79.899)
If a patient is determined to have HCQ retinopathy, documentation should include: Adverse effect of antimalarials and drugs acting on other blood protozoa, initial encounter (T37.2x5A). In our clinic, we have patients return back for testing with our technicians, which provides additional opportunities for maximizing revenue. At their comprehensive exam, I’ll typically bill for their medical exam (992x4), refraction (92015), and FAF photos (92250) with ICD-10 diagnosis codes for their disease state (ie., M06.9), AND Plaquenil use (Z79.899).
Most insurance companies deny billing photos and OCT on the same day. Therefore to finish our testing I’ll have the patient return for testing with our technician in 1 month to perform: OCT of the retina (92134) and Humphrey 10-2 central visual field (92083 – visual field examination, unilateral or bilateral, with interpretation and report, extended examination).
I then interpret the testing, fill out my report to send back to their provider, and return the testing to my technicians to call the patient with the findings.
Takehomes for managing HCQ retinopathy
In summary, the development of hydroxychloroquine retinopathy is rare (<1% under 5 years) when dosed appropriately (<5mg/kg/real body weight), but risk can increase with prolonged use (~20% at 20 years). Baseline testing should be performed 6 to 12 months after starting hydroxychloroquine or annually if additional risk factors (pre-existing retinal disease, above the maximum recommended dose, tamoxifen therapy, impaired renal function, chloroquine use) are present. FAF and SD-OCT are going to be the most sensitive and reliable tests.
To maximize revenue, you can bill your comprehensive exam as a medical encounter (992x4) with FAF (92250) and have patients return for retina OCT (92134) and optional Humphrey 10-2 central or 24-2/30-2 visual field (92083). Coordination of care is important, with letters sent back to their PCP or rheumatologist with documentation indicating whether the findings illustrate the presence or absence of high-risk factors.
The bottom line is that proper screening is essential to minimize potential vision loss and concomitant retinal impairment in patients who are actively taking hydroxychloroquine.
