


Currently an estimated 30.3 million people in the United States are diagnosed with diabetes and 84.1 million more with prediabetes.1 Due to the increasing age and rate of obesity of the US population, the number of adults with diabetes has more than tripled within the last 20 years.1 As a result, diabetic related care has become a staple of the US healthcare system. Our understanding of diabetes and its ability to affect vision continues to grow rapidly, but our vigilance to detect and treat these patients much keep pace to prevent ocular complications.
Diabetes is a complex multisystem disorder with numerous effects on ocular health. The clinical signs noted during a clinical exam can be traced to biochemical and cellular changes secondary to hyperglycemia. Proper examination of the diabetic patient requires a thorough clinical examination which can be aided in many cases with auxiliary testing. The same technologies that help researchers decipher the pathogenesis of diabetic eye disease are also helping clinicians provide elevated care within their practices. With a trend towards integrated diagnostics, where technologies such as optical coherence tomography (OCT) and fundus photography are used in tandem, software like ZEISS FORUM is improving care and decreasing workflow issues while improving the assessment of the ever-increasing amount of data that we collect from our patients.
What Is Diabetes Mellitus?
Diabetes mellitus is a group of endocrine disorders characterized by hyperglycemia resulting from defects in insulin secretion and/or insulin action. Insulin is a hormone with multiple actions, the most notable of which is the stimulation of blood glucose absorption into peripheral tissues such as skeletal muscle. The duration and severity of chronic hyperglycemia is directly associated with microvascular (diabetic retinopathy, nephropathy, neuropathy) and macrovascular complications (stroke, coronary artery disease, peripheral artery disease).
The American Diabetes Association classifies diabetes into four clinical classes:
- Type 1 diabetes (formerly known as insulin dependent or juvenile onset diabetes): Characterized by eventual absolute insulin deficiency from the autoimmune destruction of pancreatic beta cells. Primarily diagnosed before the age of 40, with peak diagnosis during the years of puberty. The destruction of beta cells is variable with some individuals exhibiting quick destruction (and earlier onset of symptoms/pathology) and others slow destruction (and later onset of symptoms/pathology).2
- Type 2 diabetes (formerly known as non-insulin dependent or adult onset diabetes): Characterized by relative insulin deficiency caused by a variable combination of insulin resistance and inadequate insulin secretion. This form of diabetes accounts for over 90% of all diabetic patients. Primarily diagnosed in middle age and older, though recent trends toward earlier adulthood are increasing.2
- Gestational diabetes: Diabetes diagnosed during pregnancy. This designation does not make distinctions between type 2 diabetes diagnosed during pregnancy from diabetes originating secondary to physiological changes associated with pregnancy.2
- Other: Includes rarer etiologies of diabetes such as genetic, exocrine disease, and drug/chemical induced.2
Criteria for the diagnosis of diabetes mellitus requires one of the following:2
- Hemoglobin A1c ≥ 6.5%
- Fasting (no caloric intake for > 8 hours) blood glucose of ≥ 126mg/dl
- Random blood glucose level ≥ 200mg/dl in a patient with classic symptoms of hyperglycemia
- 2 hour blood glucose level ≥ 200 mg/dl during an oral glucose tolerance test
What Are Non-Retinal Ocular Complications of Diabetes?
Diabetes is a systemic condition with numerous manifestations on the ocular system. Though diabetic retinopathy (DR) is the most common cause of vision loss in diabetic patients, other non-retinal complications must also be considered when evaluating the diabetic patient.
Changes in refractive error correlating to hyperglycemia or hypoglycemia are thought to be caused by altered fluid dynamics within the crystalline lens and possibly the cornea. Fluid absorption within the lens leads to changes in thickness, index of refraction, and radius of curvature. Similar changes can occur in the cornea as well, though no great evidence has illuminated the exact mechanism for refractive shifts in diabetic patients. These changes in refractive error are most evident in patients with acute blood glucose fluctuations such as the newly diagnosed (and medicated) diabetic or the undiagnosed diabetic. Though these changes are transient, normalizing within weeks after blood glucose levels are stabilized, patients may feel like their vision is permanently changed since they may become accustomed to the previous refractive error.
Diabetic neuropathy of the third, fourth, or sixth cranial nerve can produce extraocular motility deficits that are generally self-limiting within three to six months. Third nerve palsies are more common than fourth or sixth nerve palsies.
The increased prevalence of dry eye disease in diabetics is well documented with multiple possible disease contributing mechanisms. Diabetic neuropathy of the fifth nerve can lead to decreased corneal sensation, altering the blink reflex and tear secretion. Decreased innervation to the various ocular glands and trigeminal nerve leads to altered tear production and corneal sensation, respectively. These changes to the lacrimal functional unit are exacerbated by poor corneal wound healing, which can make treatment more difficult in this population.
High intraocular pressure induced by diabetic eye disease tends to occur secondary to neovascularization of the iris/angle or obstruction of the trabecular meshwork by blood and blood degradation products. Neovascular glaucoma is associated with proliferative diabetic retinopathy and believed to be caused by angiogenic factors, such as vascular endothelial growth factor (VEGF), diffusing from the ischemic posterior segment to the vasculature of the anterior uvea. Aside from direct occlusion of the angle, neovascularization of the iris and angle can hemorrhage, leading to hyphema related elevated intraocular pressure. Ghost cell glaucoma occurs when blood products from a degrading vitreous hemorrhage block aqueous outflow within the trabecular meshwork. Ghost cell glaucoma usually occurs 1-3 months after an acute vitreous bleed and is more likely to occur in patients with a disrupted anterior hyaloid face such as those with previous cataract surgery or pars plana vitrectomy.
Cataracts are a common comorbidity in diabetic patients. Lenticular changes tend to occur earlier and progress more quickly in diabetic patients and are associated with the duration of diabetes and level of hyperglycemia.
Posterior Segment Complications of Diabetes
Evaluation of the posterior segment is quite possibly the most scrutinized portion of the diabetic eye examination because the posterior retina is the primary site of damage in most diabetic patients. Microvascular changes secondary to chronic hyperglycemia lead to pericyte loss, increased vascular permeability, vascular occlusion, and fibroglial proliferation. In the advanced stages, these complications manifest as diabetic macular edema, vitreous hemorrhage, and tractional retinal detachment; the most common cause of vision loss in diabetic patients.
What Is the Mechanism of Diabetic Retinopathy?
Diabetic retinopathy is the manifestation of chronic hyperglycemia mediated microvascular damage. Though the exact pathophysiology of diabetic retinopathy has not been elucidated, numerous studies have associated worsening retinopathy with the severity and duration of hyperglycemia. Comorbidities such as hypertension and hyperlipidemia have been recognized to worsen diabetic retinopathy. It is theorized that the underlying biochemical process that fuels diabetic retinopathy formation is the creation of reactive oxygen species via individual and interrelated processes. Below are a few of the main biochemical changes implicated in the development of diabetic retinopathy.
- Activation of the polyol pathway: Increased levels of glucose cause excessive activation of the polyol pathway. This eventually leads to sorbitol accumulation, NADPH depletion, decreased nitric oxide concentrations, and the creation of reactive oxygen species.
- Creation of advanced glycation end products (AGEs): Formed during a hyperglycemic state, AGEs can alter extra-cellular matrix components resulting in increased oxidative stress, vascular permeability, and basement membrane remodeling.
- Activation of protein kinase C: Hyperglycemia directly and indirectly activates protein kinase C which in turn downregulates nitric oxide production, upregulates VEGF production, and increased oxidative stress.
- Activation of the hexoasmine pathway: Increased levels of glucose cause excessive activation of the hexoasmine pathway altering gene expression leading to vascular endothelial dysfunction.
The above biochemical processes along with concurrent inflammation and blood flow alterations eventually lead to the clinical signs noted during ophthalmoscopy. The earliest signs of diabetic retinal alterations cannot be visualized with funduscopy and are considered the preclinical signs of diabetic retinopathy. These changes mostly relate to pericyte loss and vascular basement membrane thickening. Pericytes are contractile cells that regulate blood flow vascular permeability and endothelial maintenance. Thickening of the vascular basement membrane also leads to increased vascular permeability.
The earliest clinical sign of diabetic retinopathy is the formation of focal dilations of the vascular wall of capillaries, small arterioles, or small venules called microaneurysms. Microaneurysms form in areas of pericyte loss via hemodynamic changes and vascular endothelial proliferation. Clinically, microaneurysms appear as small red dots 25 to 100 μm in diameter within the posterior pole. Early on, microaneurysms are most often noted perifoveally and may have considerable turnover, with cycles of resolution and formation.
Further microvascular changes can lead to the formation of shunt vessels and neovascularization within the retina (not to be confused with choroidal neovascularization or neovascularization of the vitreo-retinal interface). Because these changes cannot be distinguished clinically and do not seem to confer different risks of vision loss, they were combined under the umbrella term intraretinal microvascular abnormalities. Clinically, intraretinal microvascular abnormalities are noted as small tortuous vessels usually within areas of retinal nonperfusion.
Intraretinal hemorrhages are often the result of ruptured microaneurysms or leaking intraretinal microvascular abnormalities and capillaries. Most hemorrhages associated with diabetic retinopathy are of the dot/blot configuration because they lie within the perpendicularly organized retinal architecture of the middle retina. Flame hemorrhages, which can also be associated with diabetic retinopathy, take on their characteristic shape because they are found within the retinal nerve fiber layer which runs parallel to the retinal surface.

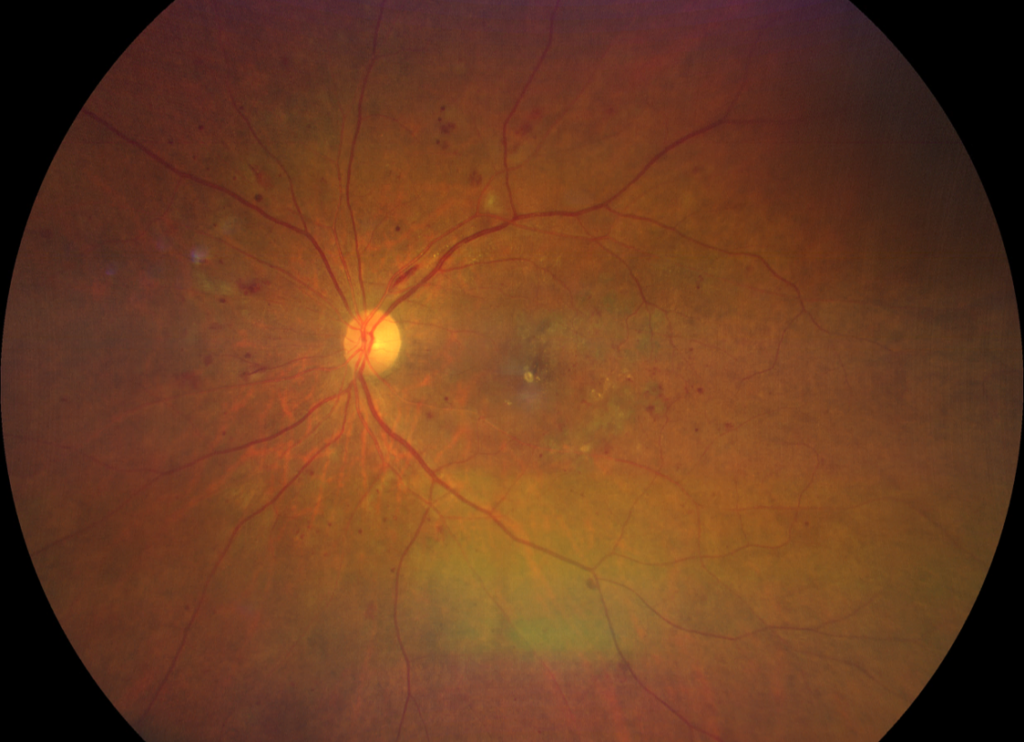
Figure 1: CLARUS 500 widefield image of blot hemorrhages (green) and a flame hemorrhage (blue).
Vascular disruption via hemorrhage or hemodynamic changes can lead to local alterations in axoplasmic flow of the retinal nerve fiber layer, resulting in cotton wool spots (soft exudates). Cotton wool spots are indistinct white to gray lesions within the retinal nerve fiber layer that can create relative scotoma. Though self-limiting, these lesions can leave lasting microscotoma and focal inner retinal atrophy.

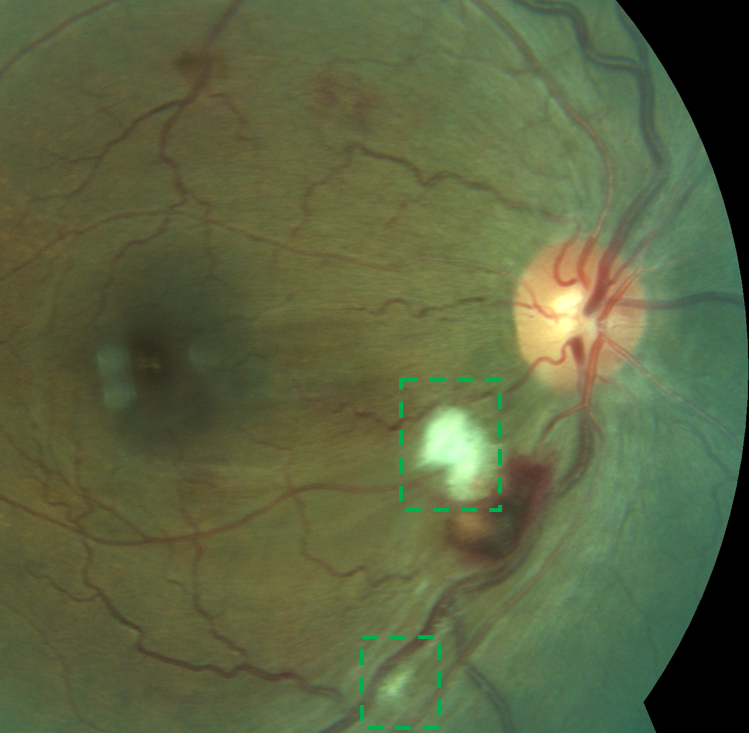
Figure 2: Standard fundus photography of cotton wool spots.
Venous caliber abnormalities associated with diabetic retinopathy range from common venous dilation to venous beading and venous loop (Omega loop) formation. Diffuse venous dilation is a response to retinal blood flow changes and loss of autoregulation secondary to chronic hyperglycemia whereas venous beading is a focal venous dilation usually found adjacent to areas of retinal nonperfusion. A venous loop is a more advanced venous abnormality where the dilated venule takes on a loop appearance and slightly protrudes into the vitreous; like venous beading this is usually found adjacent to areas of retinal nonperfusion.
As the retinal vasculature becomes further compromised and vascular permeability increases, lipid, water, and proteins leak into the extra-cellular space. Lipid extravasation within the retina is known clinically as hard exudates and is most commonly found within the posterior pole. These lesions are yellow with distinct borders and found within or adjacent to the outer plexiform layer. Hard exudates can often be found on the border of edematous and non-edematous retina, as seen in a circinate ring.

Figure 3: Above, CLARUS 500 widefield imaging of hard exudates. Below, a CIRRUS OCT scan through the area of exudation below the fovea.
Diabetic macular edema is a fluid induced retinal thickening of the macula most often associated with microaneurysms, hemorrhages, and hard exudates. This fluid accumulation is mostly comprised of water and can resolve with strict blood glucose and blood pressure control or various treatments. Chronic macular edema can lead to irreversible macular atrophy and macular hole formation.
Diabetic macular ischemia is a less understood diabetic maculopathy which has been considered both a precursor and a result of diabetic macular edema. Diabetic macular ischemia is a consequence of capillary occlusion, pericyte loss, and basement membrane remodeling. When isolated, diabetic macular ischemia is associated with foveal atrophy and a featureless fovea. Enlargement of the foveal avascular zone can be appreciated with fluorescein angiography or optical coherence angiography (OCTA).
Progressive retinal ischemia can lead to vasoproliferation on the retinal surface, optic nerve head, or anterior uvea (as described previously) via the release of angiogenic factors such as VEGF and platelet-derived growth factor. These highly permeable new vessels often grow on the border of perfused and non-perfused retina where they tend to hemorrhage or leak. Clinically, any neovascularization within 1 disc area of the optic nerve head is considered neovascularization of the disc (NVD). All other neovascularization on the retinal surface is considered neovascularization elsewhere (NVE). Hemorrhaging of these vessels between the vitreous and retina leads to a preretinal hemorrhage (boat shaped hemorrhage) with a round bottom and flat top. Vitreous hemorrhage, blood that penetrates the hyaloid membrane, can remain focal or disperse through the vitreous causing severe vision loss. Fibroglial proliferation occurs concurrently with neovascularization and can lead to significant tractional forces. Vitreous or fibroglial contraction can lead to macular schisis, tractional retinal detachment, and rhegmatogenous retinal detachment with resultant devastating effects on vision.

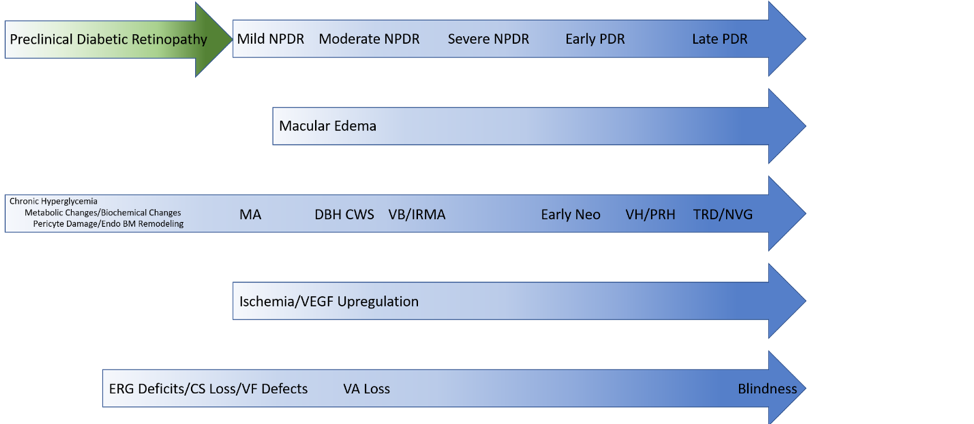
Figure 4: Diabetic Continuum
NPDR: Nonproliferative diabetic retinopathy; PDR: Proliferative diabetic retinopathy; MA: Microaneurysm; DBH: Dot/blot hemorrhage; CWS: Cotton wool spot; VB: Venous beading; IRMA: Intraretinal microvascular abnormalities; VH: Vitreous hemorrhage; PRH: Preretinal hemorrhage; TRD: Tractional retinal detachment; NVG: Neovascular glaucoma; VEGF: Vascular endothelial growth factor; ERG: Electroretinogram; CS: Contrast sensitivity; VF: Visual field; VA: Visual acuity
Diabetic papillopathy is a rare manifestation of diabetes that presents as unilateral or bilateral optic nerve head edema with peripapillary hemorrhaging and possible macular edema. Vision and visual field testing are usually minimally affected. The etiology of diabetic papillopathy is not well understood and seems to occur in both type 1 and type 2 diabetes irrespective of diabetic retinopathy severity or systemic control. The condition is relatively benign, resolving in 2-12 months with minimal optic nerve atrophy or visual sequalae.

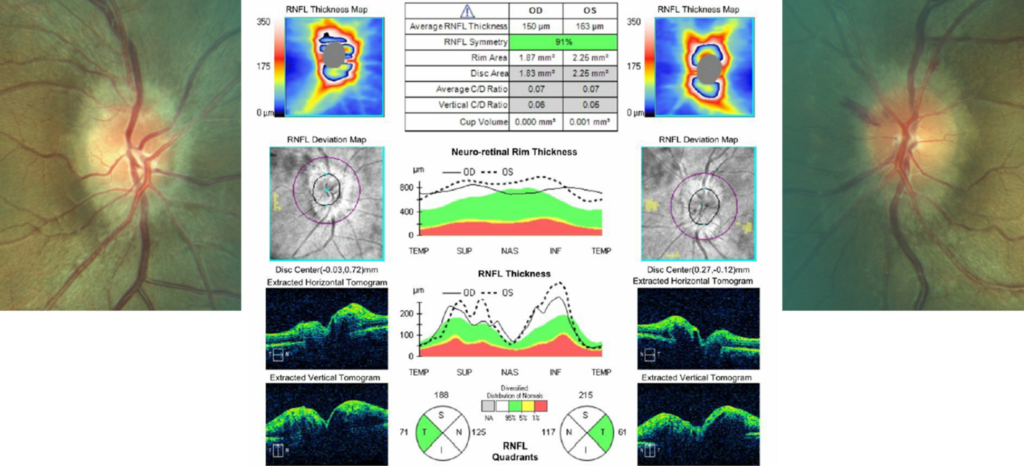
Figure 5: Fundus images and CIRRUS Optic Nerve Head OCT scans of diabetic papillopathy.
Here is a comprehensive in-depth overview on utilizing OCT to treat and manage retinal pathology with 10 pathologies and sample images.
Classification of Diabetic Retinopathy
The two most commonly used classification systems for diabetic retinopathy are a simplified Early Treatment Diabetic Retinopathy Study (ETDRS) scale and the International Clinical Diabetic Retinopathy Disease Severity Scale. The classification systems distinguish different levels of non-proliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR). Diabetic macular edema can occur at any stage of diabetic retinopathy and therefore has a separate grading system within each scale. The International Scale is easier to use because it is a simpler system and does not rely on reference images from the Airlie House classification system. Though the two grading scales are similar, they are not interchangeable. Both scales are summarized in the below.
| Diabetic Retinopathy Grade | Simplified ETDRS Scale | International Scale |
|---|---|---|
| No apparent DR | No abnormalities | |
| Mild NPDR | At least one MA but no H/MA ≥ standard photo 2A | MA only |
| Moderate NPDR | H/MA ≥ standard photo 2A, and/or CWS, VB, IRMA but NOT satisfying criteria for severe NPDR | More than just MA but less than severe NPDR |
| Severe NPDR | One or more of the following: H/MA ≥ standard photo 2A in all 4 quadrants VB in at least 2 quadrants IRMA ≥ standard photo 8A in at least 1 quadrant | Any of the following (4-2-1 rule) and no PDR Severe H in each quadrant VB in 2 or more quadrants IRMA in 1 or more quadrants |
| PDR | One or more of the following: Neovascularization VH or PRH | |
| Early PDR | New vessels and definition not met for high risk PDR | |
| High risk PDR | One or more of the following: NVD >1/3 DD NVD with VH or PRH NVE >1/4 DD and VH or PRH |
ETDRS: Early Treatment Diabetic Retinopathy Study; DR: Diabetic retinopathy; NPDR: Nonproliferative diabetic retinopathy; PDR: Proliferative diabetic retinopathy; MA: Microaneurysm; H: Hemorrhage; CWS: Cotton wool spot; VB: Venous beading; IRMA: Intraretinal microvascular abnormalities; DME: Diabetic macular edema; CSME: Clinically significant macular edema; FPD: Fibrous proliferations discs; FPE: Fibrous proliferations elsewhere; NVD: Neovascularization disc; NVE: Neovascularization elsewhere; VH: Vitreous hemorrhage; PRH: Preretinal hemorrhage; DD: Disc diameter
Posterior Segment Comorbidities
Diabetes is a risk factors for several posterior segment complications, some of which may be difficult to distinguish from diabetic complications.
Retinal vein occlusions occur when a retinal vein becomes occluded via thrombus, vasculitis, or other arterial compression. The vein occlusion is classified as branch, hemi, or central depending on the location of the obstruction. Hemorrhaging, cotton wool spots, and vascular remodeling will correspond to the area affected by the occlusion. Vein occlusions may resemble diabetic retinopathy especially in low grade or resolving cases. Significant interocular or intraocular (in the case of a branch or hemi retinal vein occlusion) asymmetry can help differentiate NPDR from retinal venous occlusive disease. Both diabetic retinopathy and retinal vein occlusions can present with macular edema which can be difficult to distinguish without significant asymmetries or association with a single vein. Fundus photography can help visualize asymmetries in hemorrhaging/vascular remodeling and edema to help with differential diagnosis. Ultra-widefield photography is particularly useful in imaging vein occlusions because one image can capture the whole expanse of the occlusion, eliminating the need for montaging multiple images. With its high resolution and stereographic capabilities, the CLARUS 500 can be used to monitor both hemorrhaging and macular edema.

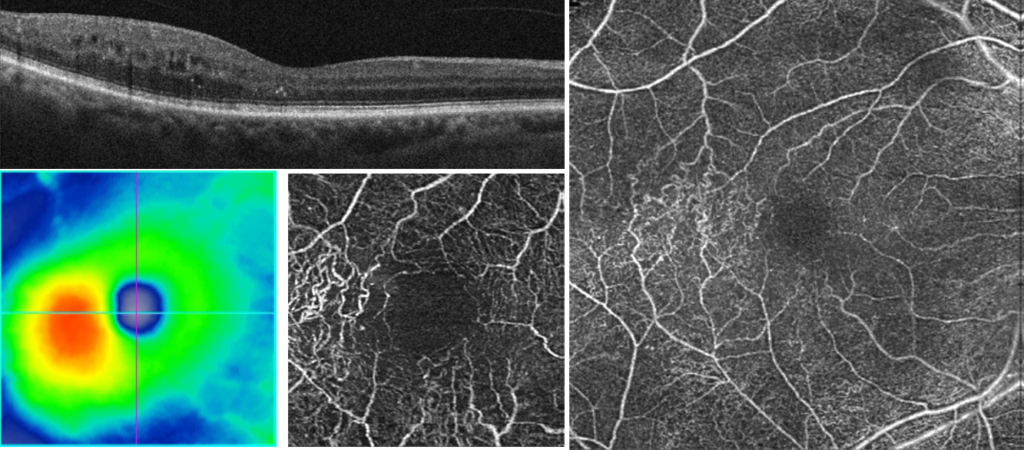
Figure 6: CIRRUS OCT scans of retinal thickening temporal to the fovea. CIRRUS Angioplex reveals vascular remodeling consistent with a compensated branch retinal vein occlusion

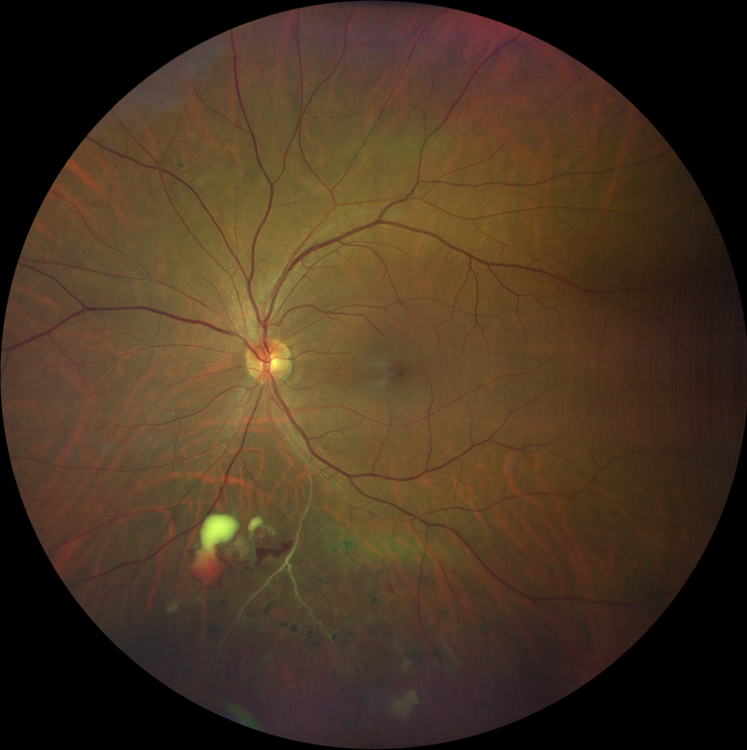
Figure 6: CLARUS 500 widefield imaging of a chronic branch retinal vein occlusion with old and new hemorrhaging. Note the areas of panretinal photocoagulation.
Retinal artery occlusions occur when a retinal artery becomes occluded via embolus, thrombosis, or vasculitis. The artery occlusion is classified as branch or central depending on the location of the obstruction. During the acute phase, inner retinal opacification and thickening is noted along the course of the occluded artery. This will eventually resolve with significant inner retinal atrophy which is easily visualized with OCT imaging. Retina previously affected by an artery occlusion will be less prone to diabetic retinopathy which may confound diagnosis.

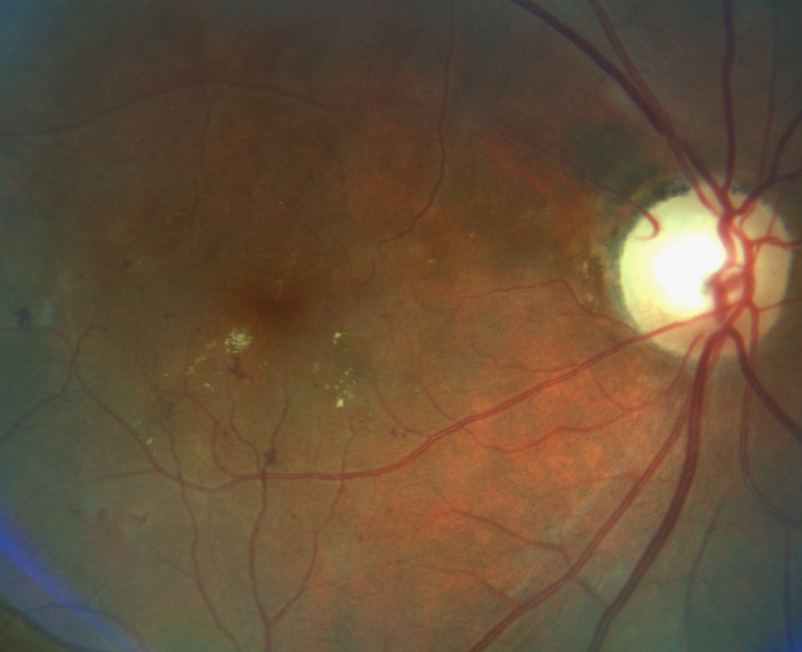

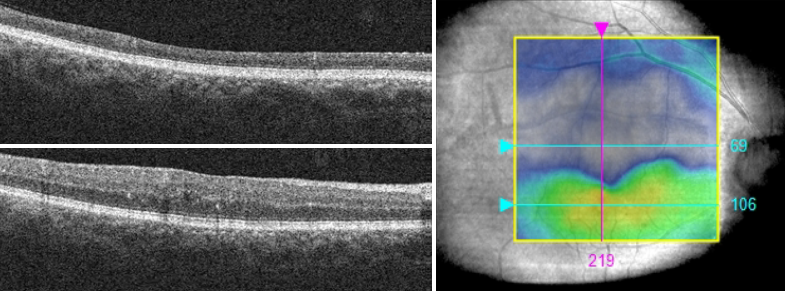
Figure 7: A chronic superior-temporal branch retinal artery occlusion with significant inner retinal atrophy as seen on CIRRUS OCT imaging. Optic nerve head pallor consistent with the occlusion is noted as well. Note the lack of NPDR in the area corresponding to the occlusion induced atrophy.
Nonarteritic anterior ischemic optic neuropathy (NAION) is believed to be caused by vascular insufficiency of the posterior ciliary circulation of the distal optic nerve. Up to 25% of patients with NAION have diabetes, with hypertension, hypercholesterolemia, and a small optic nerve head being other risk factors. During the acute phase, patients present with diffuse or sectoral disc edema with or without mild peripapillary hemorrhaging. Funduscopically, this condition is very similar to diabetic papillopathy but can be distinguished by NAION’s tendency to have more significant vision loss. Visual field testing will often reveal an altitudinal defect which can help distinguish NAION from diabetic papillopathy.
Systemic hypertension is often comorbid with diabetes and can affect the retinal vasculature in similar ways. Hypertensive retinopathy tends to have more flame hemorrhages and cotton wool spots than dot/blot hemorrhages and does not present with microaneurysms. Severe cases may present with optic nerve head edema with minimal visual changes similar to diabetic papillopathy. In theses cases, systemic blood pressure will be significantly elevated to help differentiate from a diabetic etiology. High resolution ultra-widefield fundus photography with the CLARUS 500 from ZEISS is particularly great at picking up changes in vasculature over large areas of the retina. Arterio-venous nicking and vascular attenuation can be examined easily by zooming in on images and then monitored for progression by evaluating several dates at the same time.
Learn more about the CLARUS 500 and real world clinical applications of this instrument.
Management of the Diabetic Patient
Management of the diabetic patient centers around individual risk stratification of vision loss. It is important to gather an accurate patient history, perform a thorough examination, and use auxiliary testing such as OCT when necessary to determine when a patient should follow up.
The history of every diabetic patient should include the following:
Type of diabetes: Type 1 diabetics are recommended to have an examination five years after diagnosis and at least annually thereafter.3 Type 2 diabetics are recommended to have an examination soon after diagnosis because an estimated 30% will have diabetic retinopathy at the time of diagnosis.3 Assuming no significant retinopathy is noted an annual examination is then recommended.
Diabetic patients who plan to become pregnant should have an examination before conceiving. Early in the first trimester a repeat examination should be performed. If no retinopathy, mild NPDR, or moderate NPDR is found then a repeat examination should be performed every trimester, based on individual risk for vision loss.3,4 If diabetic macular edema, severe NPDR, or PDR is found, then evaluation with an ophthalmologist experienced in the management of diabetic retinal disease should be considered (as per the author’s experience as there are no specific optometric preferred practice guidelines for these patients). Patients with gestational diabetes are not at an increased risk of vision loss and do not need to be monitored during pregnancy.
- Duration of diabetes: Time since diagnosis is an important risk factor for the development of diabetic eye disease. Duration of significant hyperglycemia is also an important risk factor but is often more difficult to discern without an extensive history of bloodwork.
- Hemoglobin A1c: The most recent hemoglobin A1c provides a valuation of overall diabetic control. Trends in hemoglobin A1c can help in the management of diabetic eye disease.
- Blood glucose: Recent blood glucose readings can help diagnose acute diabetic ocular changes such as refractive shifts.
- Systemic comorbidities: Systemic hypertension, hypercholesterolemia, and a history of smoking are independent risk factors of diabetic retinopathy and its progression.
Management and Treatment of Patients Without Diabetic Retinopathy
Diabetic patients without diabetic retinopathy require annual examination because 5-10% of patients will develop DR within 1 year. OCT imaging is not necessary in patients without diabetic retinopathy but can be useful in those with unexplained vision loss. Patients with previously poorly controlled blood glucose levels may have macular atrophy from resolved DME or macular ischemia.
Author’s Note: In diabetic patients who have media opacities, poor fixation, or difficulty sitting for an exam, I will often acquire a fundus photo or macular OCT if I feel that I was not able to properly examine the posterior pole. Fundus photos, especially ultra-widefield photos, can quickly capture a high definition image of the posterior pole which is frequently better than the clinical view in some patients. Similarly, a macular OCT scan can reveal pathology that may be missed clinically on a noncooperative patient.
Management and Treatment of Mild and Moderate Non Proliferative Diabetic Retinopathy without Diabetic Macular Edema
Mild and moderate NPDR pose minimal risk to vision and these patients should be evaluated every 6-12 month based on individual risk criteria such as comorbidities, hemoglobin A1c, and trends in blood glucose control. Patients with considerable microaneurysm turnover are more susceptible to the development of DME and should be monitored more often.5 It is difficult to appreciate microaneurysm turnover with funduscopy therefore serial fundus photography is preferred. Patients with combined posterior pole diabetic retinopathy and peripheral diabetic retinopathy may be at higher risk for disease progression and vision loss compared to patients with strictly posterior pole diabetic retinopathy.6 Ultra-widefield photography with the CLARUS 500 allows for detailed examination of small vascular details in both the macula and periphery to accurately monitor for signs of worsening disease. As retinal nonperfusion develops, a featureless retina can be easily detected using serial ultra-widefield imaging. Patients with coexistent macular disease such as vitreomacular traction or epiretinal membrane formation may be at higher risk of developing DME. An OCT scan may be useful in these patients to distinguish mechanical retinal stretching from retinal thickening associated with edema.
Author’s Note: I like to acquire fundus photos on patients with mild and moderate NPDR to document disease, evaluate for progression, and for patient education. True color ultra-widefield images acquired with the ZEISS CLARUS 500 are especially useful as patient education tools because they give patients a glimpse into what we see in their eyes. I have been taking photos on my patients for several years now and they will ask to see their photos in the same way that my glaucoma patients ask what their IOP is. I believe that involving patients in their healthcare helps with medical adherence and vision loss prevention.
Management and Treatment of Mild and Moderate Non Proliferative Diabetic Retinopathy with Diabetic Macular Edema
Though mild and moderate NPDR may pose minimal risk to vision, DME is the most common cause of vision loss in diabetic patients. DME can occur at any stage of diabetic retinopathy. Patients with nonfoveal DME but not CSME should be counseled on the potential for vision loss and monitored every 1-4 months. Fundus photography and OCT imaging aids in the detection and management of DME. The ZEISS CIRRUS OCT overlays ETDRS sectors on the retinal thickness map to help determine the risk that DME poses on vision. DME patients with vitreomacular traction or an epiretinal membrane may be at higher risk for DME progression. Patient’s with CSME should be referred to an ophthalmologist experienced in the treatment of diabetic retinal disease.

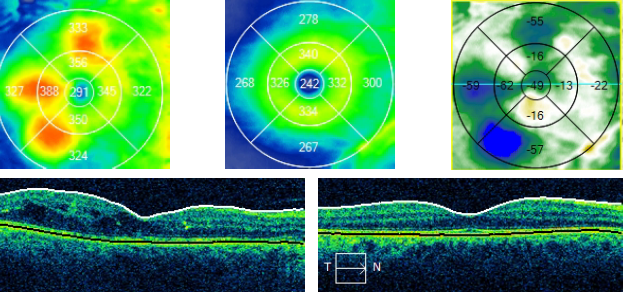
Figure 8: Sequential CIRRUS OCT imaging and Macular Change Analysis documents a resolution of diabetic macular edema.
Management and Treatment of Severe Non Proliferative Diabetic Retinopathy and Proliferative Diabetic Retinopathy
Patients with severe NPDR and PDR are at significant risk for vision loss and should be referred to an ophthalmologist experienced in the treatment of diabetic retinal disease. In some cases, it may be difficult to discern neovascularization or preretinal hemorrhages from intraretinal hemorrhages or IRMA. Diabetic neovascularization will always be on the retinal surface and tends to grow into the vitreous. A preretinal hemorrhage, especially if small, may be relatively flat and therefore difficult to discern from intraretinal hemorrhaging. An OCT scan of a preretinal hemorrhage will reveal that the blood is between the retina and posterior cortical vitreous. Dot/blot hemorrhages and IRMA will always be within the retina. In cases of fibroglial proliferation, OCT imaging can visualize vitreoretinal traction, schisis, or detachment.
Patients with quiescent PDR will often have resultant optic nerve atrophy, macular atrophy, and fibroglial proliferation. Optic atrophy will often correspond to the amount of panretinal photocoagulation and does not require intervention. Retinal nerve fiber layer imaging with OCT will usually reveal diffuse thinning. Visual field testing will often reveal diffuse or nonspecific defects which are not consistent with other forms of optic neuropathy like NAION or neurological loss. Macular thinning and outer retinal atrophy are common after macular laser therapy and can often explain chronic vision loss in patients with no current retinopathy. Macular ischemia must also be considered when vision is reduced and no active retinopathy is noted. OCT imaging is useful to determine the extent of macular atrophy and determine the cause of vision loss. Fibroglial proliferation may continue to pull on the retina even in quiescent PDR and must be monitored with clinical examination and OCT imaging to monitor for macular schisis and detachment. In cases of worsening vision or retinal architecture, referral to a vitreo-retinal specialist should be considered.
Diabetic Retinopathy in Cataract Perioperative Care
Diabetic patients tend to manifest cataracts at a younger age and progress more rapidly than non-diabetics. The literature gives conflicting reports on whether cataract surgery leads to progression of diabetic retinopathy but there is good evidence to show that cataract surgery can worsen existing diabetic macula edema.7 Extra care must be taken to rule out DME during the preoperative period to minimize poor surgical outcomes. Diabetic patients, even those without a history of macular edema, have a higher rate of pseudophakic cystoid macular edema (CME) and must be monitored appropriately.8 Patients with vision threatening diabetic eye disease should be evaluated by an ophthalmologist experienced in the care of diabetic eye disease before cataract surgery is considered. Some surgeons choose to lengthen the preoperative and postoperative drop regimen in patients with diabetic retinopathy to counteract the higher incidence of pseudophakic CME.

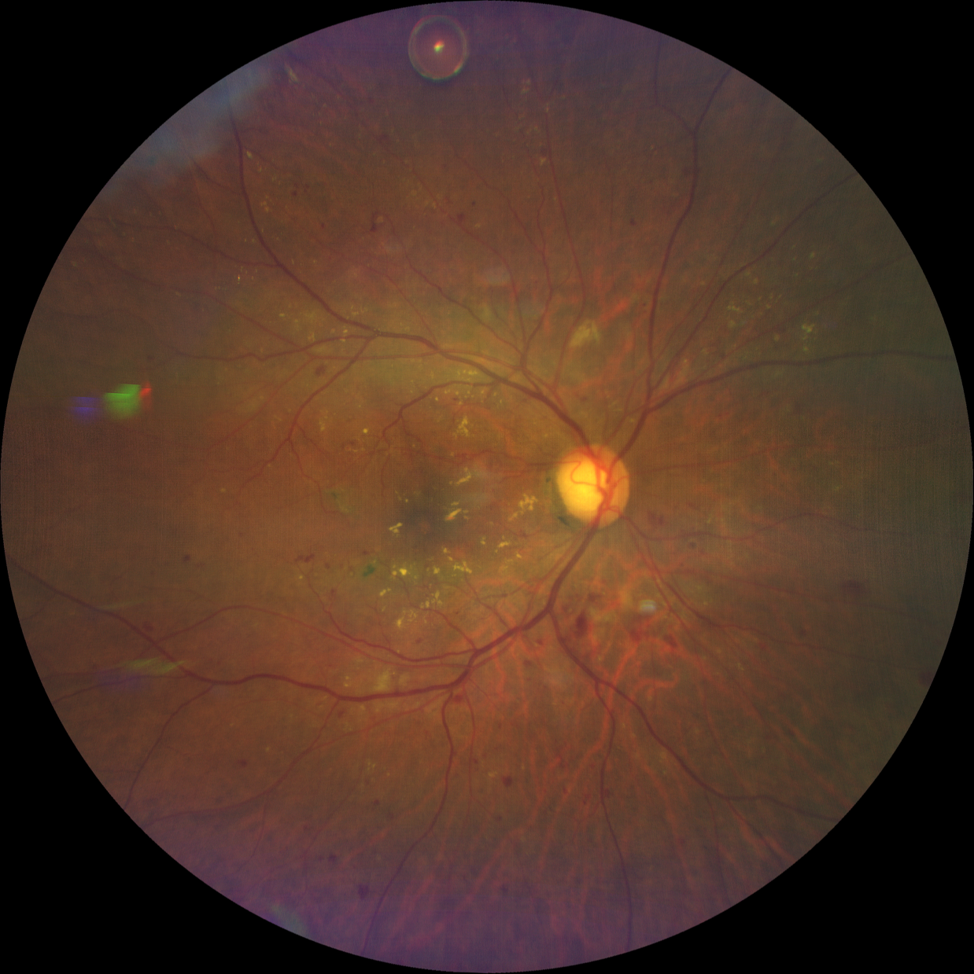
Figure 9: CLARUS 500 widefield imaging of a patient with moderate NPDR and DME referred for cataract surgery. A bolus of intravitreal anti-VEGF can be seen floating superiorly. The patient was pretreated with anti-VEGF by his retinal specialist before being referred for cataract surgery.
Author’s Note:
I would get an OCT scan of the macula of every patient with diabetic retinopathy before referring for cataract surgery and then repeat the scan 3-4 weeks postoperatively to ensure that there is no macular edema. The ZEISS CIRRUS Macular Change Analysis is especially useful in these cases to see if any edema is present as it allows visualization of both scans at the same time and calculates any differences in retinal thickness.
To prevent superfluous referrals, it is important to distinguish DME from pseudophakic CME. DME tends to be irregular and asymmetric in regard to the fovea whereas pseudophakic CME tends to be symmetric and centered on the fovea. Unlike pseudophakic CME, DME tends to be associated with hard exudates which can be visualized as hyper-reflective structures in or adjacent to the outer plexiform layer. In cases of pseudophakic CME, topical treatment can be initiated and referral to an ophthalmologist deferred.

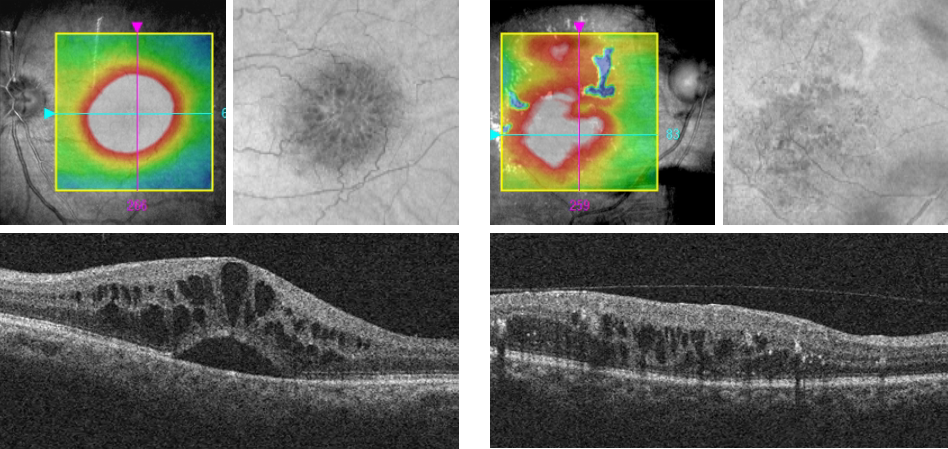
Figure 10: On the left, CIRRUS OCT imaging of pseudophakic cystoid macular edema. On the right, CIRRUS OCT imaging of diabetic macular edema.
Integrated Diagnostics in the Management and Treatment of Diabetic Patients
Integrated diagnostics (the use of multiple imaging modalities) is important in diabetic patients because multiple issues can affect the retina and optic nerve. Diabetes is also a risk factor for multiple comorbidities which may be difficult to distinguish from diabetic retinopathy with a clinical examination alone. In the presence of diabetic eye disease, accurate imaging with fundus photography, OCT, and perimetry can help guide patient management. Unfortunately, it can often become cumbersome to analyze multiple data points over multiple time periods without significant time and effort. A platform like the ZEISS Integrated Diagnostics Imaging solution, using gold-standard imaging devices and ZEISS FORUM ophthalmology software, can help streamline data analysis and reveal pathological changes that are difficult to visualize otherwise. In addition, ZEISS Integrated Diagnostic Imaging can help create individualized management plans based on multiple, easily interpreted imaging modalities.
Conclusion
Diabetes mellitus is a multi-system disease which requires a multi-disciplinary approach to manage. With a rapidly growing diabetic population, optometrists are well positioned to manage these patients and help reduce the burden of diabetic eye disease. A high-tech approach utilizing OCT, fundus photography, and integrated diagnostics can further grow the optometrist’s role in the diabetic care team and curtail the staggering forecasts of diabetic related vision loss.
References
- “Division of Diabetes Translation At A Glance | CDC.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 2019, www.cdc.gov/chronicdisease/resources/publications/aag/diabetes.htm.
- American Diabetes Association. “2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2018.” Diabetes careSupplement 1 (2018): S13-S27.
- American Academy of Ophthalmology Preferred Practice Pattern “Diabetic Retinop” 2017
- American Optometric Associated Evidence-Based Clinical Practice Guideline “Eye Care of the Patient with Diabetes Mellitus.”
- Nunes, Sandrina, et al. “Microaneurysm turnover is a biomarker for diabetic retinopathy progression to clinically significant macular edema: findings for type 2 diabetics with nonproliferative retinopathy.” Ophthalmologica5 (2009): 292-297.
- Silva, Paolo S., et al. “Peripheral lesions identified on ultrawide field imaging predict increased risk of diabetic retinopathy progression over 4 years.” Ophthalmology 122.5 (2015): 949-956.
- Hayashi, K., et al. “Changes in diabetic macular oedema after phacoemulsification surgery.” Eye 23.2 (2009): 389.
- Pollack, A., et al. “Cystoid macular oedema following cataract extraction in patients with diabetes.” British Journal of Ophthalmology 76.4 (1992): 221-224.
The statements of the healthcare professional whose opinion is contained in this material reflect only their personal opinions and experiences and do not necessarily reflect the opinions of any institution with whom they are affiliated. The healthcare professionals whose opinion is contained in this material does not have a contractual relationship with Carl Zeiss Meditec and not received financial compensation. Not all products, services or offers referenced in this article are approved or offered in every market and approved labeling and instructions may vary from one country to another.
