
Watch Dr. Ryan Vida discuss SMILE surgery in this video!
Chapter 1: Preoperative assessment
1.1 Ophthalmic examination
- History
- Ocular dominance
- Pupils
- Cover testing at distance and near, with and without glasses and ocular motility testing
- Confrontational fields testing
- Monocular and binocular uncorrected distance visual acuity (UDVA)
- Monocular and binocular uncorrected intermediate visual acuity (UIVA)
- Monocular and binocular uncorrected near visual acuity (UNVA)
- Lensometry of current spectacles and corrected distance visual acuity (CDVA) and distance corrected near vision (DCNV) with these (the patient’s current vision with current correction)
- Manifest distance refraction with CDVA
- Contrast sensitivity testing (CSV-1000) through best manifest refraction correction
- Night vision simulation for patients with high refractive error or larger than average scotopic pupil diameter (greater than 6.3 mm)
- Slit-lamp examination including fluorescein staining
- Tear break-up time (TBUT)
- Schirmer's test
- Goldmann applanation tonometry
- Cycloplegic refraction and CDVA (after dilation with 1.0% Tropicamide)
- Dilated fundus examination using slit-lamp and binocular indirect ophthalmoscopy
Importance of repeatability and accuracy of manifest refraction
The goal of manifest refraction in refractive surgery is to determine the optimal sphere and cylinder lenses that will maximize visual acuity for a particular eye. Refraction for glasses is often considered to be an art, whereas refraction for surgery should be considered a science. When refracting for spectacles, the artistic elements include pushing axes to the horizontal or vertical, minimizing the cylinder used, and keeping cylinder axis orthogonal between eyes, etc. Refraction for refractive surgery is quite different as the aim is to fully correct the existing refraction, so the maximum cylinder and exact axis of astigmatism should be determined irrespective of verticality and orthogonality to the opposite eye.
Manifest refraction is the most critical data entry component for refractive surgery planning and yet it is probably the least studied and researched. So much emphasis has been placed on measuring and correcting higher-order aberrations, when in fact for most eyes, these details are completely wiped-out by a sphere or cylinder (lower order) error of -0.25 D. The limited focus on perfecting the technique is evidenced by the relatively low number of published studies investigating the accuracy, repeatability or reproducibility of refraction. A review of the literature to date highlights the fact that the repeatability of manifest refraction is in the order of 0.25 D.8 Therefore, even under controlled conditions, there is an error associated with manifest refraction that likely cannot be eliminated. This is due to the fact that manifest refraction is commonly limited to be measured in 0.25 D increments since it is difficult for most patients to differentiate between the blur induced by smaller increments.
In a refractive surgery clinical setting, it is important that the reproducibility of manifest refraction between clinicians, both surgeons and co-managing optometrists, is known in order to compare measurements obtained at different time points and detect significant changes. This is particularly important in clinical settings where numerous different clinicians are performing refractions at different time-points. The accuracy of refractive surgery depends on nomogram adjustments, which in turn depend on the agreement between the measured refraction and the actual refraction. A nomogram can only be built with accurate manifest refraction measurements, both before and after surgery.
1.2 Refraction stability
1.3 Dry eye
- Previous ocular history including detailed history for glasses and contact lens wear: period of wear, type of lens/glasses, wear modality, last worn, comfort or visual symptoms associated with wear, history of blepharitis
- Ocular symptoms, especially dry eye symptoms with/without contact lenses and pattern, and use of lubricants
- OSDI dry eye questionnaire9
- Slit-lamp examination including fluorescein and lissamine green staining
- Tear break-up time
- Schirmer’s test
- Strip meniscometry10
- HD Analyzer optical quality and scatter11
- Anterior blepharitis
- Posterior blepharitis & meibomian gland dysfunction (MGD)
- Exposure dry eye
- Aqueous deficiency
- Inflammatory dry eye
- Anterior basement membrane dystrophy (ABMD)
- Corneal hypoesthesia
- Ocular surface toxicity
1.4 Contraindications for SMILE
- Previous herpes simplex virus (HSV) keratitis within 1 year (if more than 1 year, perform corneal sensitivity testing and use oral antiviral medication prophylaxis before and after surgery)
- Active auto-immune disease – lupus, rheumatoid arthritis, etc.
- Keratoconus or other corneal ectatic disease
- Severe aqueous deficient dry eye
- Unrealistic expectations
- Diabetes with active retinopathy (higher risk of infection and slower healing response)
- Fibromyalgia (FM) / myalgic encephalomyelitis (ME) / irritable bowel syndrome (IBS): referral to a corneal specialist needed, but SMILE can be performed with appropriate consent and management
- Visually significant cataract: corneal refractive surgery is a good option for mild cataract as the cataract may not progress. Corneal surgery is also more accurate and avoids the increased risks associated with intraocular surgery
- Glaucoma: can have surgery if IOP is well controlled with minimal visual field loss, and diurnal IOP curve is assessed before and after surgery
- Vascular macular disease: note that PRK is conventionally safer than LASIK as no suction is applied, but the VisuMax affords the lowest increase in IOP of any femtosecond laser or microkeratome at levels that are negligible12,13
- Retinal detachment: clearance from a retinal specialist is recommended, beware scleral bands anteriorly
- Epithelial or anterior stromal dystrophies: PRK may be a more appropriate treatment as it has a therapeutic effect,14 although the low suction applied by the VisuMax means SMILE can be performed even in patients with known ABMD
- Fuch’s endothelial dystrophy: endothelial cell count is required before surgery, SMILE can be performed as long there are >1,200 cells/mm2, consider treating one eye at a time
- Corneal scar that could affect intrastromal cutting accuracy in the optically active zone
- Depression or anxiety conditions if not stabilized
- Non-availability for follow-up or co-management
Keratoconus
Just as for LASIK, keratoconus screening is the main focus of the suitability assessment for SMILE; keratoconus has conventionally been a contraindication for any elective refractive procedure that involves the removal of stromal tissue. Unfortunately, it seems that the attention given to the biomechanical advantages of SMILE has sometimes been misinterpreted as there being no risk of accelerating ectasia after SMILE, and therefore a reasonable treatment for keratoconus patients. However, this is not the case. SMILE, just as with any other type of corneal laser procedure, should not be performed in the presence of keratoconus.
Chapter 2: Informed consent
2.1 Lay explanation of SMILE
Here is a view of a cornea in cross-section [draw cross-sectional view diagram]. In LASIK, an infra-red laser is used to make a cut just below the surface of the cornea that becomes a flap. This flap is lifted and an ultra-violet laser is used to evaporate a lens of tissue. The flap is then put back in place, so at the end it looks like this from the outside [draw front view diagram].
In SMILE, the same tissue that was evaporated in LASIK is removed from slightly deeper in the center of the cornea [draw cross-sectional view diagram], with the lens of tissue delineated by the infra-red laser alone. Then a small tunnel is made to the surface and the tissue is removed through the tunnel. Therefore, it looks like this from the outside [draw front view diagram] with only a small incision visible on the surface, quite different to LASIK.
In SMILE, all of the tissue in front of the lens that was removed has not been cut, whereas in LASIK all the tissue in front of the lens has been cut. Because the front of the cornea is stronger than the back of the cornea, SMILE leaves the strongest part of the cornea intact rather than operating in the strongest part of the cornea as in LASIK. Similarly, most of the nerves in the cornea are in the front part, so SMILE disturbs the corneal nerves less than LASIK.
Figure 1: Simple cartoon diagram that is hand-drawn in front of the patient, together with the associated script, to help explain the difference between SMILE and LASIK.
2.2 Lay explanation of expected outcome and safety
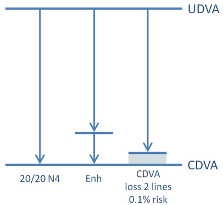
The overall aim of treatment is to go from here [draw UDVA line], what you currently see without glasses for both distance and near, to here [draw arrow from UDVA line to CVDA line], your best corrected level of vision at distance and near. This is the intended outcome based on all our findings and simulations so far [annotate CVDA line with current visual acuity].
However, there is a possibility that your eyes may heal slightly differently to how we expect, meaning that you don’t end up quite where we planned [CDVA line]. The eyes may settle either slightly over the target or slightly under the target [draw second arrow that ends short of the CDVA line]. Or one eye may be slightly over and the other slightly under the target. In these cases, the vision and visual comfort will not be as good as anticipated. In addition to this, if you get to here [CDVA line] initially, but then slowly drift back to the midway line, known as regression, again the vision will not be as expected. However, as long as glasses alone can still correct the blurring, then there is no damage to the vision, and we may be able to perform an enhancement procedure to maximize your vision to the intended target [draw a short arrow from the midway line to the CDVA line]. We do of course need to let everything settle and stabilize, during which time glasses can be used if needed and after repeating all the measurements, we can do a simple enhancement as long as it is safe to do so.
The other scenario is that if you end up just short of the perfect outcome [draw third arrow to end just short of the CDVA line], but glasses or contact lenses cannot correct your vision, then this would mean that some damage has been caused to the eyes by the surgery—i.e. you would have lost something you had before, some of your best spectacle corrected vision [shade the region between the midway line and CDVA line]. This equates to losing 2 lines on the vision chart [indicate on the ETDRS chart]. The risk of losing 2 lines in your case is <0.1% (<1% for higher prescriptions) [annotate the risk of losing 2 lines CDVA]. It ranges from <0.1% to <1% based on the prescription. However, it is usually possible to correct this last bit with further surgery if necessary.

2.3 Risks and alternatives discussed with the patient
- Things that will happen:
- Dry eye symptoms expected to last on average 3-4 months, which will require the use of artificial tear drops or additional lubricants, and may be permanent in rare cases
- Fluctuations in vision due to tear film system instability and the gradual reduction in corneal swelling that causes random blurring as it dissipates, most noticeable in the first month, but may continue for 3-4 months
- Night glare and haloes around lights at night expected to last 3-4 months, more so for higher corrections, and may be permanent in some cases
- Possible complications:
- Epithelial erosion
- Epithelial ingrowth / implantation
- Corneal haze
- Diffuse lamellar keratitis (DLK)
- Suction loss
- Rare complications:
- Infection
- Retinal detachment
- Persistent corneal swelling
- Vascular occlusion
- Ectasia
- Equipment malfunction
- Factors the surgery doesn’t change, but may affect the outcome:
- Cataract development
- Amblyopia (or lazy eye)
- Strabismus (squint)
- LASIK
- Surface ablation
- Phakic IOL
- Clear refractive lens exchange
Chapter 3: SMILE procedure
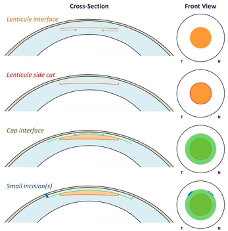
- Lenticule interface: this interface defines the refractive power of the lenticule and is created from the periphery and moves towards the center.
- Lenticule side cut: this interface is created at the border of the lenticule to provide a clearly defined edge. This is also known, and programmed, as the minimum lenticule thickness.
- Cap interface: this interface is created parallel to the corneal surface to delineate the upper surface of the lenticule, and extend further peripherally to provide access for the surgeon. The cap interface is created from the center towards the periphery.
- Small incision(s): this interface creates a tunnel to link the cap interface to the corneal surface, created at the outside edge of the cap.

3.1 Routine docking process
3.2 Accounting for cyclotorsion
3.3 Femtosecond Laser Cutting (photodisruption)
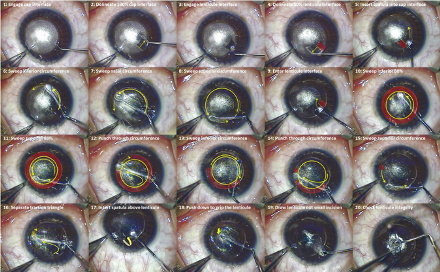
3.4 Surgical Technique

Chapter 4: Postoperative Management and Complications
4.1 Bowman’s microdistortions / cap folds
4.2 Atypical DLK: Interface focal inflammatory keratitis after SMILE

4.3 Epithelial implant
Conclusion
References
- Intrastromal corneal ring implants for corneal thinning disorders: an evidence-based analysis. Ont Health Technol Assess Ser. 2009;9:1-90.
- Sekundo W, Kunert K, Russmann C, Gille A, Bissmann W, Stobrawa G, Sticker M, Bischoff M, Blum M. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia: six-month results. J Cataract Refract Surg. 2008;34:1513-1520.
- Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011;95:335-339.
- Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: All-in-one femtosecond laser refractive surgery. J Cataract Refract Surg. 2011;37:127-137.
- Hjortdal JO, Vestergaard AH, Ivarsen A, Ragunathan S, Asp S. Predictors for the outcome of small-incision lenticule extraction for Myopia. J Refract Surg. 2012;28:865-871.
- FDA. VisuMax femtosecond laser system for refractive correction (PMA), 2016.
- FDA. VisuMax femtosecond laser PMA supplement for approval of myopia with and without astigmatism, 2018.
- Raasch TW, Schechtman KB, Davis LJ, Zadnik K. Repeatability of subjective refraction in myopic and keratoconic subjects: results of vector analysis. Ophthalmic Physiol Opt. 2001;21:376-383.
- Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the Ocular Surface Disease Index. Arch Ophthalmol. 2000;118:615-621.
- Dogru M, Ishida K, Matsumoto Y, Goto E, Ishioka M, Kojima T, Goto T, Saeki M, Tsubota K. Strip meniscometry: a new and simple method of tear meniscus evaluation. Invest Ophthalmol Vis Sci. 2006;47:1895-1901.
- Ye C, Ng PK, Jhanji V. Optical quality assessment in normal and forme fruste keratoconus eyes with a double-pass system: a comparison and variability study. Br J Ophthalmol. 2014;98:1478-1483.
- Vetter JM, Faust M, Gericke A, Pfeiffer N, Weingartner WE, Sekundo W. Intraocular pressure measurements during flap preparation using 2 femtosecond lasers and 1 microkeratome in human donor eyes. J Cataract Refract Surg. 2012;38:2011-2018.
- Vetter JM, Holzer MP, Teping C, Weingartner WE, Gericke A, Stoffelns B, Pfeiffer N, Sekundo W. Intraocular pressure during corneal flap preparation: comparison among four femtosecond lasers in porcine eyes. J Refract Surg. 2011;27:427-433.
- Zuckerman SJ, Aquavella JV, Park SB. Analysis of the efficacy and safety of excimer laser PTK in the treatment of corneal disease. Cornea. 1996;15:9-14.
- Reinstein DZ, Gobbe M, Gobbe L, Archer TJ, Carp GI. Optical Zone Centration Accuracy Using Corneal Fixation-based SMILE Compared to Eye Tracker-based Femtosecond Laser-assisted LASIK for Myopia. J Refract Surg. 2015;31:586-592.
- Li M, Zhao J, Miao H, Shen Y, Sun L, Tian M, Wadium E, Zhou X. Mild decentration measured by a Scheimpflug camera and its impact on visual quality following SMILE in the early learning curve. Invest Ophthalmol Vis Sci. 2014;55:3886-3892.
- Lazaridis A, Droutsas K, Sekundo W. Topographic Analysis of the Centration of the Treatment Zone After SMILE for Myopia and Comparison to FS-LASIK: Subjective Versus Objective Alignment. J Refract Surg. 2014;30:680-686.
- Liu M, Sun Y, Wang D, Zhang T, Zhou Y, Zheng H, Liu Q. Decentration of optical zone center and its impact on visual outcomes following SMILE. Cornea. 2015;34:392-397.
- Ganesh S, Brar S, Pawar A. Results of Intraoperative Manual Cyclotorsion Compensation for Myopic Astigmatism in Patients Undergoing Small Incision Lenticule Extraction (SMILE). J Refract Surg. 2017;33:506-512.
- Jun I, Kang DSY, Reinstein DZ, Arba-Mosquera S, Archer TJ, Seo KY, Kim TI. Clinical Outcomes of SMILE With a Triple Centration Technique and Corneal Wavefront-Guided Transepithelial PRK in High Astigmatism. J Refract Surg. 2018;34:156-163.
- Zhao Y, Li M, Yao P, Shah R, Knorz MC, Zhou X. Development of the continuous curvilinear lenticulerrhexis technique for small incision lenticule extraction. J Refract Surg. 2015;31:16-21.
- Ganesh S, Brar S. Lenticuloschisis: A "No Dissection" Technique for Lenticule Extraction in Small Incision Lenticule Extraction. J Refract Surg. 2017;33:563-566.
- Yao P, Zhao J, Li M, Shen Y, Dong Z, Zhou X. Microdistortions in Bowman's layer following femtosecond laser small incision lenticule extraction observed by Fourier-Domain OCT. J Refract Surg. 2013;29:668-674.
- Luo J, Yao P, Li M, Xu G, Zhao J, Tian M, Zhou X. Quantitative analysis of Microdistortions in Bowman's Layer using optical coherence tomography after SMILE among different myopic corrections. J Refract Surg. 2015;31:104-109.
- Shetty R, Shroff R, Kaweri L, Jayadev C, Kummelil MK, Sinha Roy A. Intra-Operative Cap Repositioning in Small Incision Lenticule Extraction (SMILE) for Enhanced Visual Recovery. Curr Eye Res. 2016;41:1532-1538.
- Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: diagnosis and management. J Cataract Refract Surg. 2000;26:1072-1077.
- Reinstein DZ, Stuart AJ, Vida RS, Archer TJ, Carp GI. Atypical presentation of diffuse lamellar keratitis after SMILE: sterile multifocal inflammatory keratitis. J Cataract Refract Surg. 2018 [In Press].
- El-Naggar MT. Bilateral ectasia after femtosecond laser-assisted small-incision lenticule extraction. J Cataract Refract Surg. 2015;41:884-888.
- Mattila JS, Holopainen JM. Bilateral Ectasia After Femtosecond Laser-Assisted Small Incision Lenticule Extraction (SMILE). J Refract Surg. 2016;32:497-500.
- Sachdev G, Sachdev MS, Sachdev R, Gupta H. Unilateral corneal ectasia following small-incision lenticule extraction. J Cataract Refract Surg. 2015;41:2014-2018.
- Wang Y, Cui C, Li Z, Tao X, Zhang C, Zhang X, Mu G. Corneal ectasia 6.5 months after small-incision lenticule extraction. J Cataract Refract Surg. 2015;41:1100-1106.
- Reznik J, Salz JJ, Klimava A. Development of unilateral corneal ectasia after PRK with ipsilateral preoperative forme fruste keratoconus. J Refract Surg. 2008;24:843-847.
- Navas A, Ariza E, Haber A, Fermon S, Velazquez R, Suarez R. Bilateral keratectasia after photorefractive keratectomy. J Refract Surg. 2007;23:941-943.
- Graue-Hernandez EO, Pagano GL, Garcia-De la Rosa G, Ramirez-Miranda A, Cabral-Macias J, Lichtinger A, Abdala-Figuerola A, Navas A. Combined small-incision lenticule extraction and intrastromal corneal collagen crosslinking to treat mild keratoconus: Long-term follow-up. J Cataract Refract Surg. 2015;41:2524-2532.
- Ganesh S, Brar S. Clinical Outcomes of Small Incision Lenticule Extraction with Accelerated Cross-Linking (ReLEx SMILE Xtra) in Patients with Thin Corneas and Borderline Topography. J Ophthalmol. 2015;2015:263412.
- Reinstein DZ, Archer TJ, Gobbe M, Bartoli E. Corneal sensitivity after small-incision lenticule extraction and laser in situ keratomileusis. J Cataract Refract Surg. 2015;41:1580-1587.
- Reinstein DZ, Archer TJ. Real-time bilateral LASIK procedure, 2013.