


Simple dimple? Cover-me-up . . .
Patient X and Y present with an alike degree and characteristics of a pterygium growth. Both have it surgically removed by the same surgeon…
The one-week post-operative consultation yields a happy patient X, with no complaints. Patient Y complains about a foreign body and a scratchy sensation. Their opinions of and satisfaction with the surgical outcome differ, although the pterygium excision was successful according to the surgeon’s desire in both cases.
Corneal dellen commonly present as a plain, basic dimple in a dry spot, bordering an elevated area. However, the simplicity of a dellen cannot be ignored. This saucer-shaped excavation should be managed accordingly, to rule out further patient discomfort and complications.
Anterior ocular segment educational resources provide very little information on corneal dellen (usually only a paragraph or two). Below is a detailed review and summary for clinical recognition on successfully managing and treating corneal dellen.
Overview: Corneal dellen . . . what, how, why and who?
Definition: What is corneal dellen?
Dellen, also referred to as ‘delle’ or ‘Fuch’s dimples,’ can either be corneal or scleral. It is a small, localized area of structural thinning (usually the epithelium), with distinct borders of an oval-shaped lesion. Dellen are usually seen at the limbus, adjacent to a focal elevated area.1-3 Dellen can be classified as a non-infectious corneal ulcer and subcategorized as a secondary marginal or peripheral degeneration.2,4
Pathophysiology: How does corneal dellen form?
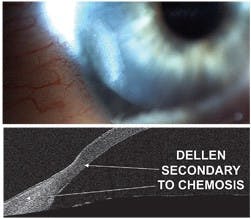
Tear film instability and dry eye are key initiating factors for dellen formation.1,3 When a localized area of corneal epithelium experiences surface drying and poor wetting, the stroma suffers from water loss.1, 3 Any elevation difference between the peripheral cornea and adjacent structures, such as the conjunctiva in the case of chemosis, allows for improper lid margin contact during blinking. This exacerbates dryness in the lower levels of the ocular surface.2
Etiology: Why does corneal dellen form?
Anterior ocular surface elevation causing dellen formation can include chemosis, conjunctival hemorrhages, episcleritis, filtering blebs, pterygiums, pingueculas, tumors, extra-ocular muscle surgery, and cataract surgery. Idiopathic formation can also occur in the elderly.1, 3, 5
Figure 1 shows post-pterygium surgery dellen, in patient Y, with different slit-lamp views.

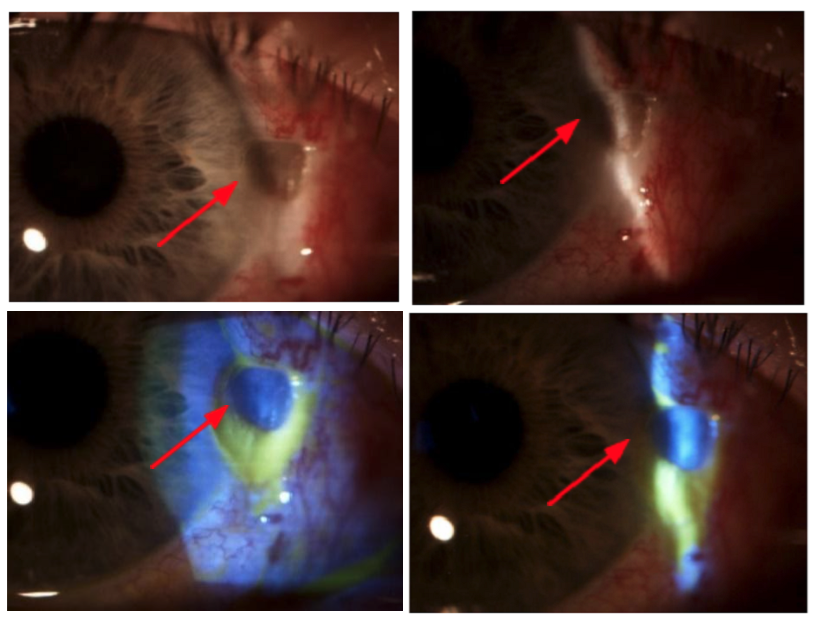
Figure 1
Typical patient type: Who is likely to experience corneal dellen?
- Patients who have had recent anterior eye surgery (post-operative dellen)3
- The elderly1
- RGP wearers6
- Dry eye patients2
- Patients with incomplete eyelid closure7
Presentation
Symptoms: Patients may complain of ocular irritation and foreign body sensation. Some patients may initially even present asymptomatically (depending on the location and size of the dellen).3
Signs: Use your slit-lamp to look for any area of peripheral corneal thinning in a focal ellipse form. Use fluorescein to confirm your diagnosis, by identifying fluorescein pooling in the excavation (minimal staining). Rose Bengal dye can also be used. As it is not of infectious nature, there will be no infiltrates, along with a quiet anterior chamber. Mild conjunctival hyperemia may surround the dellen.2,3 In dry eye patients, an obvious reduced tear break-up time and thin tear meniscus will be evident.7
Differential diagnosis of corneal dellen
- Peripheral corneal thinning, ulceration or degeneration3
- Corneal furrow degeneration (usually bilateral)4,8
- Terrien’s marginal degeneration (usually bilateral)4
Key Clue: Remember the defined dimple/ellipse/oval shape of a dellen and identify a causative area of elevation adjacent to it (unilateral condition).
Treatment and management options for corneal dellen
- Artificial tears and ointment as a baseline treatment3
- apply every two to four hours in the affected eye
- if the etiological cause cannot be eliminated, such as in the case of a filtering bleb, use viscous artificial tear drops four to eight times daily, preferably preservative-free
- Encourage eyelid-cornea surface contact / blinking action2,3
- identifying the etiology
- excision of causative elevated lesion, if dellen persists
- Patching3,6
- eye patching
- bandage contact lens
- Antibiotic ointment, if dellen persists with inflammatory signs3
- four times daily in the affected eye
- [Tear film instability allows the ocular surface to be more susceptible to infection. The normal, healthy tear film contains proteins, antibodies, and phagocytic cells which fight micro-organisms and act as a bactericidal system6]
- Autologous serum tears9
- four to six times daily in the affected eye, tapering as results prove satisfactory
- [These contain growth factors promoting cell proliferation and migration]
- Occlusion of punctum7
- punctal plugs
When to use bandage soft contact lenses with corneal dellen
If corneal re-epithelization is delayed with the first one-week follow-up, consider a bandage soft contact lens.
Fitting a contact lens in a dry eye patient is contradictory. The bandage contact lens limits mechanical eyelid irritation, which speeds up re-epithelization and enhances corneal thickening at the dellen location. Choosing the appropriate soft contact lens and using contact lens compatible (preferably preservative-free) artificial tears, will encourage dellen closure.6
It is important to follow a strict follow-up routine to monitor for any underlying corneal ulceration.
The contact lens should be replaced regularly.6
Choosing the correct type of soft bandage contact lens is fundamental.6 Ideal properties of the bandage contact lens:
- The contact lens diameter should be big enough to cover over the dellen
- Ensure that there is no contact lens edge mechanical abrasion to worsen the dellen depth
- The contact lens base curve should be compatible with the corneal curvature. Avoid a fit that’s too flat (increased movement upon eyelid blinking) or too steep, (little movement and minimal/no tear exchange beneath the lens).
- Lens material should allow for minimum lens dehydration6
- Hydrogel lenses (with a medium- to low-water content), allow for reduced in-eye dehydration. However, it cannot be used on an extended wear routine. Alternatively, a daily disposable lens can be used for already existing contact lens wearers, who are familiar with the insert, removal, and caring regimen.
- Silicone hydrogel (with a high-water content) are naturally hydrophobic. Although the latest technology advancements allow for increased lens surface hydrophilicity and lubricity. These lenses are more ideal for extended wear in non-contact lens wearers.
- Lens material should be compatible with patient’s tear film, for minimal lens surface deposits and contamination6
Patient script for treatment
- Introduce the treatment plan to the patient
- Ensure the patient knows in which eye to administer their eye drops
- Ensure the patient understands how often eye drop needs to be instilled
- Explain the timeframe of the treatment
- Alert the patient on any side effects and red-flag symptoms
- Schedule the follow-up visit with the known date and time before the patient leaves the consulting rooms and confirm the patient’s contact details.
Follow-up routine
A weekly follow-up schedule is recommended. If severe corneal thinning is noted, the patient needs to be seen sooner. Continue aggressive lubrication until the cornea proves to show normal thickness.3 Once the corneal healing process reaches satisfaction, a bi-monthly follow-up can be arranged.
A slit-lamp and anterior OCT are helpful in documenting the progression and healing of dellen.
Dellen rarely become larger than 2mm.10

Untreated dellen
Dellen complications are rare because of their sterile nature. Although in severe cases, if left untreated, continued thinning can lead to perforation.11
It is important to maintain the equilibrium of the limbus. The limbus acts as the doctor, being responsible for corneal regeneration, wound repair, and barrier protection. Corneal stem cells are generated by the limbus for the ongoing process of corneal re-epithelization. These functions are crucial in order to maintain corneal transparency and avoid inflammation.9,12
ICD-10 coding
- Z09.0 – Follow-up examination after surgery
- H04.1 – Dry eye syndrome
- H18.8 – Erosion (recurrent) of cornea
Conclusion
A dry eye is not a healthy eye. In our clinic, post-operative dellen seem to be more common in smokers. Ensure adequate case history and consider systemic health as part of the healing process and prognosis. It is also important to rule out infectious ulceration. Don’t underestimate an area of corneal thinning. Be alert to anterior segment red flags as well as patient complaints and symptoms.
Dynamite comes in little packages . . . clip the fuse before the explosion. Treat and follow up dellen accordingly.
References
- Grayson, M. Diseases of the cornea. Missouri : The C.V. Mosby Company, 1979. pp. 182, 276. 0-8016-1964-5.
- Chandler, W.C., Sugar, J. and Edelhauser, H.F. External Diseases. Singapore : Mosby, 1994. p. 9.12. Vol. 8. 1-56375-101-1.
- Bagheri, N. and Wajda, B.N. The Wills Eye Manual. 7. s.l. : Wolters Kluwer, 2017. pp. 90,91. 9781496318831.
- Bohigian, G.M. External diseases of the eye. Second. St. Louis : DAC Medical Publishing Assoc., 1982. pp. 43,44. 80-67605.
- 5. Episcleritis: An Everyday Infection. Rubinfeld, R. and Chase, C. 8, August 15, 2001, Review of Optometry, Vol. 138.
- Efron, N. Contact lens complications. Three. s.l. : Elsevier, 2012. pp. 87,90,255,152. 978-0-70-20-4269-0.
- Don’t Act Rash for Rash. Gurwood, A.S. 09, September 29, 2006, Review of Optometry, Vol. 143:09.
- Is Patient's Age a Factor? Gurwood, A.S. October 21, 2009, Review of Optometry.
- When Corneal Wounds Won’t Heal. Bozung, A. and Hammond, P. August 15, 2019, Review of Optometry.
- Anterior Segment OCT Revealed. Miller, J. October 20, 2009, Review of Optometry.
- A visual guide to some of the worst complications of the anterior segment. Sindt, C.W. January 15, 2014, Review of Optometry.
- Corneoscleral Concerns: Trouble at the Border. Mannen, M. April 15, 2021, Review of Optometry.

