



While the balance between red and blue states in America seems to be at the heart of any talking head debate on cable news, it may be more appropriate to characterize an increasing proportion of the country as green. In recent years, a significant number of states have legalized marijuana for medicinal or recreational use, despite remaining illegal at the federal level.
Here we examine the factors driving this societal change and why eyecare providers must stay informed on policy and science.
A changing cannabis map
More than two-in-three Americans (68%) support legalizing marijuana, according to a recent Gallup poll from 2021, continuing a five-decade-long upward trend, as seen in Image 1 from Gallup.
While support does appear to fall along party lines, with 83% of Democrats surveyed supporting legalization, for the first time, Republicans were divided 50-50. State governments across the country, incentivized by the prospect of billions in additional tax revenue, have capitalized on this support to legalize cannabis in some form.
Only Idaho and Nebraska remain as states where marijuana and its components remain 100% illegal. While marijuana remains illegal at the federal level, both Republican and Democratic administrations have essentially turned a blind eye to these state-level changes, allowing access to marijuana to millions of Americans for the last several years.

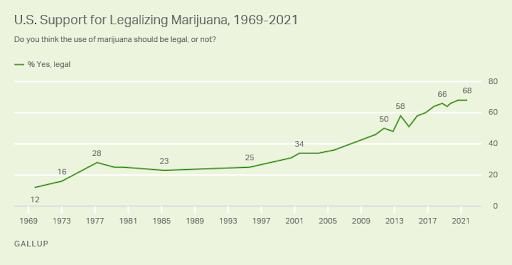
Image 1: Growing Support:Gallup
A parallel trend: Interest in alternative medicine and social media
With increasing life span, chronic systemic disease requiring treatment is growing. Two-thirds of all US adults aged 49-64 and 90% of individuals 65 or older have been prescribed five or more medications at a time.1
Many Americans have grown more open-minded to complementary and alternative medicine (CAM) avenues to reduce their reliance on prescription medications. Rhee et al. reported as many as 5-10% of glaucoma patients reportedly used CAM, with almost 60% of these patients using more than one modality.
Social media has emerged as a powerful tool in marketing marijuana directly to consumers. Building online communities around marijuana use have had specific consequences in the glaucoma population. Jia et al. performed a social media content analysis regarding marijuana and glaucoma, concluding that a “significant portion of online material was pro-medical cannabis use in the setting of glaucoma (24% of Google, 59% of YouTube, and 21% of Facebook results).”2
The combination of growing availability, increasing patient interest in alternative treatment, and the marketing campaigns of the growing marijuana industry have an increasing number of glaucoma patients wondering, “Is marijuana an option for me?”
Cannabis and the Endocannabinoid System (ECS) and glaucoma
Cannabinoids, the active components of cannabis, are derived from flowers and leaves of Cannabis sativa, Cannabis indica, and Cannabis ruderalis. About 113 different cannabinoids can be isolated from Cannabis sativa, of which the most represented and studied include delta-9-tetrahydrocannabinol (THC), classically responsible for the psychoactive effects, and cannabidiol (CBD), more traditionally associated with “wellness and healing.”
Cannabinoids can be administered orally, topically, or through inhalation, with bioavailability for cannabinoids in humans highest when inhaled.3 An extensive first-pass liver metabolism reduces the oral bioavailability to 5–20% for THC and 13–19% for CBD.4
To understand the potential for marijuana as a therapeutic for glaucoma, let’s review the physiology of the Endocannabinoid System (ECS). Cannabinoids bind with cannabinoid receptor 1 (CB1) and cannabinoid receptor 2 (CB2). CB1 and CB2 are natural receptors for endocannabinoids, lipid-based neurotransmitters produced naturally throughout the body that modulate several physiologic and cognitive processes such as appetite, pain sensation, and memory.
CB1 and CB2 are expressed in the human retina, RPE, ciliary body, Schlemm’s canal, and trabecular meshwork (Image 2)5, and are thought to modulate signal transduction photo-transduction, and IOP control.5
Image 2 represents the endocannabinoid receptors in the angle.

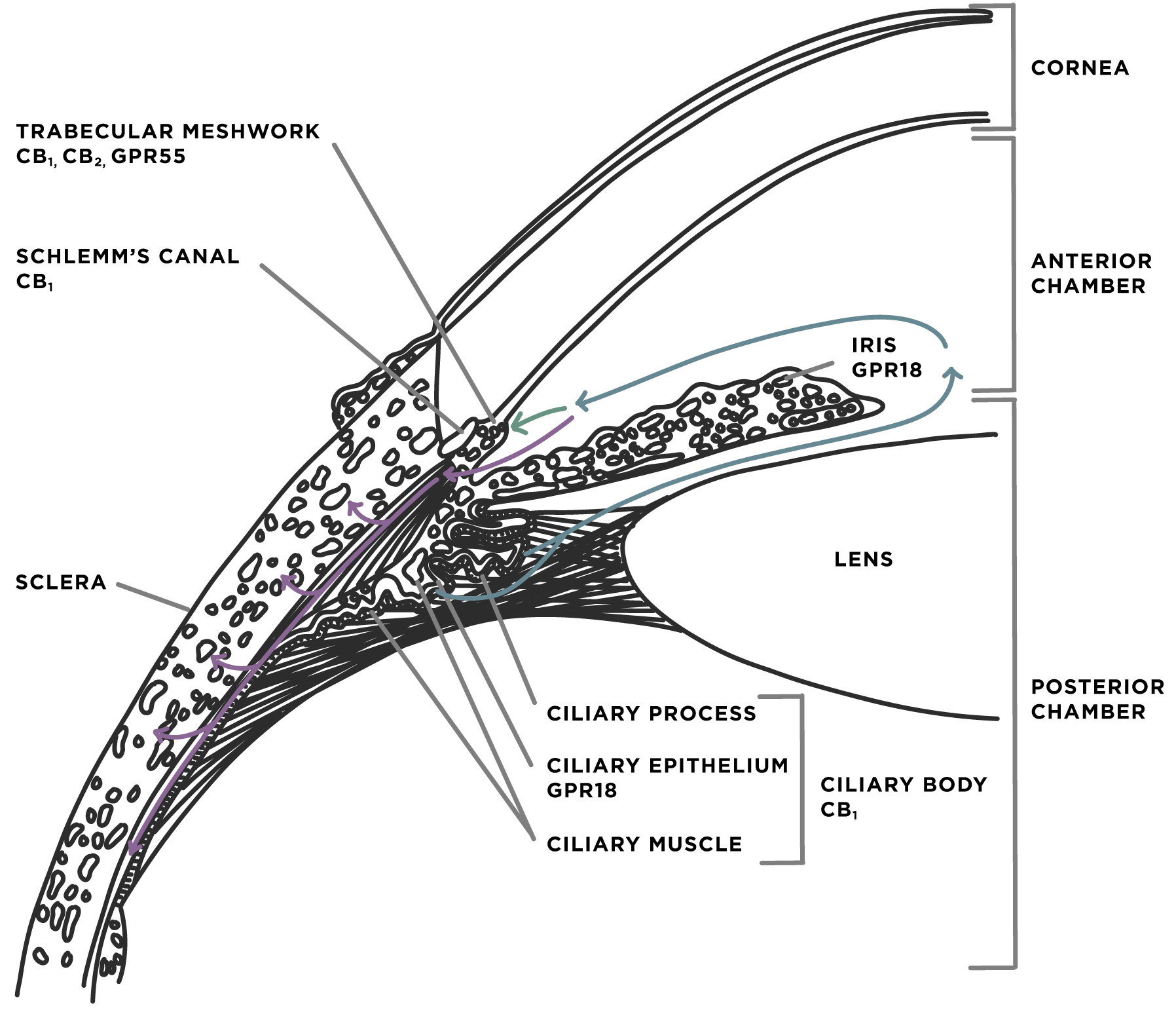
Image 2
The best-studied endocannabinoid is Anandamide, which is thought to play an important role in Parkinson’s and Alzheimer’s disease. Anandamide is present in high levels in the retina and anterior structures. It interacts with CB1 for ciliary muscle contraction, dilation of Schlemm’s canal, and effects on vascular tone,6 all possible mechanisms by which intraocular pressure (IOP) may be lowered.
The ECS facilitates neuroprotective effects by decreasing retinal ganglion cell death by a variety of pathways, including:6
- Inhibition of the excitatory amino acid glutamate, which is known to facilitate cell death pathways
- Inhibition of Endothelin-1, possibly improving optic nerve head perfusion
- Inhibition of nitric oxide release. Similarly to glutamate, the release of nitric oxide is involved in cell death pathways
Glaucoma and marijuana: Where is the data?
In 1997, glaucoma was designated by the National Institute of Health (NIH) as one of five conditions with “at least a suggestion of therapeutic value for marijuana, for which further study is indicated.” Despite this special designation, studying the potential medical benefits of cannabis has proven challenging, with interested researchers having to navigate significant red tape.
Another limitation has been that THC remains a psychoactive substance that can lead to impairment with systemic administration. While a few studies have managed to recruit larger cohorts, many suffer from small sample sizes (most ten or fewer subjects) and involve healthy subjects, limiting their applicability to populations with the disease. Below we review the available data on the effect of cannabis on IOP and glaucoma.
IOP studies
The first publication demonstrating the IOP lowering effect of cannabis came from Hepler and Frank in 1971.7 Demonstrating ~30% reduction in IOP sustained for 3-4 hours after smoking and ingestion. Cooler and Gregg showed in 1977 that IOP dropped by 37.5% when THC was administered intravenously to a group of 6 human subjects.8
Topical administration has been evaluated but has been found to be significantly less efficacious. Jay et al. reported no difference in IOP when comparing topical 1% THC vs. control vehicle in 1983.9 They postulated that their lack of effect was related to poor corneal penetration.
While the research rate has slowed down in subsequent decades, a comprehensive literature review of more recent studies, published in 2020 by Passani et al., corroborates the early evidence. Substantial IOP lowering (>25-30%) was demonstrated in the majority of studies involving oral, inhaled, and intravenously administered cannabinoids (predominantly delta-9-THC), which was sustained for 30-180 minutes after administration.
The vast majority of studies involving topically administered cannabinoids failed to demonstrate a significant IOP lowering effect.
The most recent evidence includes the gold standard for research, a prospective randomized double-blinded placebo-controlled trial from Mosaed et al.11 Here study participants were randomized to receive a single dose of inhaled cannabis or a placebo. Subjects self-administered inhaled cannabis or placebo cigarette in negative-pressure rooms, with measurements of IOP, systemic blood pressure, and plasma THC levels taken at baseline and every 40 minutes for 2 hours, and afterward, every hour for 3 hours.
Their conclusions were once again that inhaled cannabis lowers IOP significantly from baseline in healthy adult subjects, with this effect being detected from 40 minutes post-treatment and lasting up to 4 hours. Systemic blood pressure was not significantly affected.
Neuroprotection
Beyond IOP lowering, animal studies have suggested additional neuroprotective effects of cannabinoids. Reduction in ganglion cell death increased optic nerve head blood flow, and reduced axonal oxidative stress have all been reported in rat and rabbit models after treatment with cannabinoids.12,13,14
Sex-related differences
Miller et al. demonstrated sex-dependent IOP response in mice treated with topical THC, with male mice showed a statistically significantly greater and more sustained response than females.15 The latter calls into question the results of the human studies, as many of these studies involved primarily male subjects.
Tolerance
To date, many of the studies have established an immediate IOP lowering effect with inhaled, ingested, or intravenous cannabinoids.
But how does this affect change with time?
Flach et al. looked at nine POAG patients on maximally tolerated medical therapy and added 10 to 80mg of orally administered delta-9-THC to their glaucoma regimen.16 Over 36 weeks, they noted that the initial IOP lowering effect was limited in subsequent weeks, concluding subjects were likely developing tolerance to the cannabinoid effect. The requirement for increased dosing to achieve the same IOP lowering effect lent itself to increased systemic side effects, which became intolerable for many of the subjects throughout the study.
Summary of cannabis evidence and limitations
- Cannabis in inhaled, oral, and intravenous forms can significantly lower IOP for 30 minutes, with effects lasting up to 4 hours after administration.
- Topical cannabinoids have not been able to demonstrate a similar effect in numerous studies to date, presumably due to poor ocular penetration across the cornea.
- While the data is clear that cannabis can achieve comparable IOP to lowering to other pharmacologic agents on the market, there remain several limitations to cannabis becoming a legitimate treatment option
- The deleterious systemic effects of smoking have been well documented and at this point appear to negate any medicinal benefits of cannabis for the treatment of glaucoma, especially compared to other available treatments
- While oral and intravenous forms avoid the negative health impacts of smoking, concerns around impairment due to psychoactive effects do not make this administration routes viable options for most patients in the real world
- Animal study data suggests that there may be significant sex-related differences in IOP reduction, which requires additional study in humans.
- While the majority of studies have looked at the isolated IOP lowering effect after a single dose of cannabis, the currently limited data on regular dosing suggests a tolerance or tachyphylaxis effect, with increased amounts required with repeat administration to achieve similar IOP lowering
What about CBD?
CBD has been increasingly ubiquitous in society and is legally available in various forms both via retail stores and online. Unlike the traditional associated psychoactive effects of THC, CBD has been dubbed a “safer” cannabinoid, reportedly offering numerous health benefits “without the high.” While ongoing investigations on the medicinal properties of CBD are underway, there is some early evidence to suggest it may be harmful in the setting of glaucoma.
Miller et al. at Indiana University demonstrated statistically significant and sustained IOP increases with topical CBD in mice. Although the exact mechanisms are under investigation, this increase in IOP is thought to be mediated by CB1 antagonism.
Anecdotally, I have noted a handful of my glaucoma patients whose IOP had been previously well-controlled until they began incorporating CBD supplements into their diet. IOP normalized once the patient stopped these supplements. Given how easily accessible CBD is and its growing popularity, I routinely ask all my patients specifically about any CBD supplementation, particularly if their IOP begins to rise without another explanation.
Conclusions and future directions
The current evidence demonstrates that cannabis can lower IOP, quite comparably to other IOP lowering pharmacologic agents on the market. However, concerns remain regarding detrimental lung and cardiovascular effects of chronic cannabis use, particularly when smoked, and potential negative impacts on mental health and impairment when consumed in any form.
Currently, the American Academy of Ophthalmology (AAO) and American Glaucoma Society (AGS) both recommend against the use of cannabis in treating glaucoma, given the numerous other options that have been well studied are known to be effective. Eyecare providers must be aware of the potentially harmful effects of CBD, with its potential to significantly raise IOP.
Researchers are still searching for the holy grail, with investigations ongoing to formulate a topical cannabinoid, which would avoid many of the current concerns around medical cannabis for glaucoma. The potential for a new class of glaucoma medications, which would utilize our natural endocannabinoid system to lower IOP and potentially offer neuroprotective effects, remains a warranted area of investigation.
Additional research is necessary to investigate potential sex-related differences between males and females as well as the role of tolerance and potential diminished therapeutic effect with prolonged use.
Understanding how your front-line colleagues approach glaucoma is more important than ever. Download Eyes On Eyecare's free 2024 Glaucoma Report to see how your colleagues diagnose, treat, and manage this condition!
References
- Jia et al. Marijuana and Glaucoma: A social media content analysis. Ophthalmology Glaucoma; March 2020: 1-5.
- Kantor ED, Rehm CD, Haas JS, Chan AT, Giovannucci EL. Trends in prescription drugs use among adults in the United States from 1999-2012. JAMA. 2015;314:1818-31.
- Mechoulam R., Parker L.A., Gallily R. Cannabidiol: An overview of some pharmacological aspects. J. Clin. Pharmacol. 2002;42:11S–19S. doi: 10.1002/j.1552-4604.2002.tb05998.x
- Lindgren J.E., Ohlsson A., Agurell S., Hollister L., Gillespie H. Clinical effects and plasma levels of DELTA 9-tetrahydrocannabinol (DELTA 9-THC) in heavy and light users of cannabis. Psychopharmacology. 1981;74:208–212. doi: 10.1007/BF00427095.
- Cairns et al. The Endocannabinoid System as a Therapeutic Target in Glaucoma. Neural Plasticity. Volume 2016.
- Yazulla S. Endocannabinoids in the Retina: From Marijuana to Neuroprotection. Prog Retin Eye Res. 2008 September; 27(5): 501-526
- Hepler RS, Frank IR. Marihuana smoking and intraocular pressure. JAMA. 1971;217(10):1392.
- Cooler P, Gregg JM. Effect of delta-9-tetrahydrocannabinol on intraocular pressure in humans. South Med J. 1977;70:951–4.
- Jay WM, Green K. Multiple-drop study of topically applied 1% delta 9 tetrahydrocannabinol in human eyes. Arch Ophthalmol. 1983;101:591–3.
- Passani A, Posarelli C, Sframeli AT, Perciballi L, Pellegrini M, Guidi G, Figus M. Cannabinoids in Glaucoma Patients: The Never-Ending Story. J Clin Med. 2020 Dec 8;9(12):3978.
- Mosaed et al. The Effect of Inhaled Cannabis on INtraocular Pressure in Healthy Adult Subjects. US Ophthalmic review. 2020;13(2): Epub ahead of journal publication
- Crandall J., Matragoon S., Khalifa Y.M., Borlongan C., Tsai N.T., Caldwell R.B., Liou G.I. Neuroprotective and intraocular pressure-lowering effects of (-)Delta9-tetrahydrocannabinol in a rat model of glaucoma. Ophthalmic Res. 2007;39:69–75.
- Hommer N., Kallab M., Szegedi S., Puchner S., Stjepanek K., Bauer M., Schmidl D. The effect of orally administered dronabinol on optic nerve head blood flow in healthy subjects—A randomized clinical trial. Clin. Pharmacol. Ther. 2020;108:155–161. doi: 10.1002/cpt.1797
- Yoles E., Belkin M., Schwartz M. HU-211, a nonpsychotropic cannabinoid, produces short- and long-term neuroprotection after optic nerve axotomy. J. Neurotrauma. 1996;13:49–57.
- Miller et al. Delta-9-Tetrahydrocannabinol and Cannabidiol Differentially Regulate Intraocular Pressure. IOVS, December 2018; Vol 59, No 15.
- Flach A.J. Delta-9-tetrahydrocannabinol (THC) in the treatment of end-stage open-angle glaucoma. Trans. Am. Ophthalmol. Soc. 2002;100:215–222.
