


As well as being the proverbial window to the soul, in the optometry world, the eye is also the window to the brain. Just by looking at optic nerve health and visual fields, optometrists can diagnose brain diseases such as tumors and strokes. But can the eye be part of the key to solving a debilitating brain disorder that has stumped scientists for years?
Introduction to Alzheimer’s disease
For many decades, scientists and doctors have dedicated their careers to finding a way to detect and prevent the onset of Alzheimer’s disease (AD).
Alzheimer’s disease is a degenerative disorder of the nervous system that affects approximately 10% of the population over the age of 65.1 It leads to atrophy in mainly the frontal, temporal, and parietal lobes, which typically manifests as short-term memory loss, impairment of judgment, and loss of emotional control.
There has been a very small genetic correlation found in Alzheimer’s disease, but most of the cases are random.
Currently, the only precise way to diagnose Alzheimer’s disease is via brain tissue biopsy or post-mortem tissue samples in which they look for abnormal aggregates of Beta-amyloid in the form of senile plaques and abnormal phosphate tau or neurofibril tangles, both of which are responsible for maintaining normal neuronal morphology in its healthy form and, when sick and aggregated, can lead to cell death and dementia.
Doctors and scientists are still trying to find ways to identify AD pre-mortem and changes in the eye may be one of them.
Identifying Alzheimer's through visual functional changes
There are myriad changes to visual function that can occur in an AD patient that can be useful for detecting the disease. Many of these tests can be performed in an optometric office with little to no equipment.
Visual acuity
Visual acuity can be impacted by Alzheimer's disease. Studies have shown that using Regan low-contrast acuity charts, visual acuity reduction is correlated with contrast reduction.2 Furthermore, when visual acuity is reduced to an extreme level, whether due to lack of optical correction or cataracts, visual hallucinations can occur in patients.3
Color vision
Color vision defects may be present in up to 50% of patients. Whether it is a red/green or blue/yellow defect is still unknown. A study by Wood et al., 19974 found that cognitive tasks in which color was used as an attention enhancer, a cue, or a distractor, patients with AD were less accurate in their performance than controls.
Visual fields
A study by Simao et al., 20135 found that greater than 10% per year loss in visual field and optic disc cupping were demonstrated in glaucoma patients who were later diagnosed with AD, whereas an average of 3% per year loss in visual field was observed in glaucoma patients who did not develop AD. This indicates that AD may accelerate the progression of glaucoma.
Defects in fixation, smooth, and saccadic eye movements
It was found that patients with AD lost their ability to fixate over time, which is thought to be due to degeneration of the parietal lobe. Sadun et al., 19906 found that 50% of the patients with AD had difficulty initiating or maintaining saccadic eye movements. Smooth pursuits, which can be a sensitive indicator of brain function, may be affected. A study by Fletcher et al, 19887 found that smooth pursuit ability gradually deteriorated with AD. This is likely due to the degeneration of frontal and/or parietal lobes.
Pupillary function
One study found that 0.01% tropicamide instilled into the pupils caused at least a 13% greater dilation in AD eyes compared to controls due to changes in the cholinergic system.8 However, this is not a well proven test and can be confounded by other diseases such as Parkinson’s or vascular dementia.
Naming and identifying objects
Studies have found that AD patients can have an impairment in eye-head coordination as well as problems with finding objects when surrounded by other objects in the environment.9 Improvement is seen with optical correction and increase in stimulus contrast.
ERG changes
In one of the largest prospective studies to date with nearly 3300 patients, Parisi et al., 200110 found that AD was significantly correlated with abnormal pattern electroretinogram (PERG) responses. As you can see from the image below (right side), AD patients show a delayed and reduced amplitude response in PERG recording, which was also associated with RNFL thinning.
In Figure 1, the left image shows measurement of nerve fiber layer thickness (NFL) in control (top), AD patients (middle and bottom). To the left of each NFL image is the corresponding PERG recordings. A marked decrease in NFL was found which correlated with delayed implicit times and reduced amplitudes of PERG.

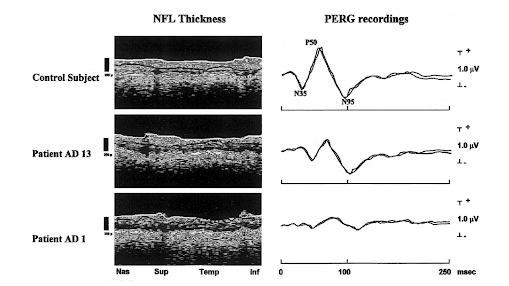
Figure 1 (Parisi et al., 2001)
Identifying Alzheimer's through ocular structural/pathological changes
Studies have been endlessly researching ways to identify AD via structural changes in the eye. With the help of OCT, OCTA and FAF (fundus autofluorescence) they were able to identify markers of AD in the retina. This may allow scientists in the future, even optometrists, to identify AD patients in a non-invasive way.
OCT
In a recent large review done by Song et al., 202111, the authors found that in most studies there was a statistically significant association found between the diagnosis of AD and abnormal RNFL thinning, mostly pronounced in the inner layers such as RNFL and GL-IPL layer (AKA: the ganglion cell complex). In a study by Cunha et al., 201712, they were able to demonstrate a statistically significant thinning in the fovea and parafoveal region in the AD vs control group.
Furthermore, in a study by Parisi et al., 2001, as previously mentioned, found abnormal PERG responses that were significantly correlated with reduced RNFL thinning in each quadrant in AD patients compared to control (see image above). It is important to note, however, that other neurodegenerative diseases such as Parkinson’s Disease and Lewis Body Dementia were also shown to have reduced RNFL thickness when compared to healthy controls, so we need other ways to differentiate AD.
OCTA
OCTA is a new, non-invasive technology that can map out the retinal vascular network and identify areas of hypoxia or damage without the invasive use of intravenous fluorescein angiography dye. Since AD is a neurodegenerative disease and is shown to cause microvascular disease in the brain, it was believed that these vascular changes could be seen in the eye.
One study by Wang et al., 201813 found that AD patients showed a significant decrease in perfusion density in the deep capillary plexus as well as a larger foveal avascular zone. As stated earlier, studies have shown that AD can increase the risk for glaucoma progression in patients who already have it, which may be due to reduced peripapillary vessel density.14
Another study by Valenti et al., 201015 found that glaucoma patients with neurodegenerative diseases such as AD show faster rates of RNFL thinning compared to someone with just glaucoma (see image below). This is likely because AD destroys visual pathway fibers that result in earlier expression of functional losses in glaucoma.
In Figure 2, the top left image depicts the nerve fiber layer (NFL) using a stratus OCT in a healthy age-matched control patient. The top right shows the same image but in an AD patient. The middle image is also an OCT of NFL of a patient with Parkinson’s and glaucoma. The yellow arrow shows area of thinning hypothesized to be due to neurodegenerative diseases. The red arrow indicated thinning attributed to glaucoma.
The bottom three images show cross sections of optic nerve (the red areas indicate nerve fiber layer) in normal, AD patient and Parkinson’s and glaucoma patient respectively from left to right. There was a marked decreased in NFL in the Parkinson’s and glaucoma patient compared to healthy and AD patient indicating that neurodegenerative diseases can accelerate NFL thinning and progression of glaucomatous changes.

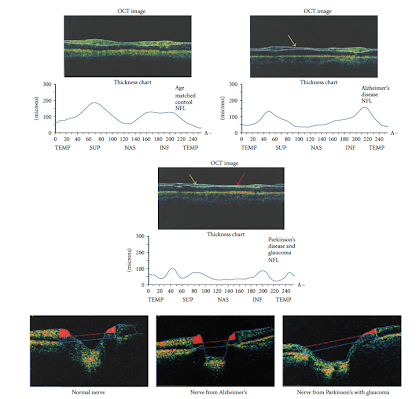
Figure 2 (Valenti et al., 2010)
Fundus autofluorescence (FAF)
Lipofuscin, a molecule found in drusen and related to ocular diseases such as AMD, have been linked to AD. Lipofuscin contains beta-amyloid and its often released following the death of neurons. In a study by Kayabasi et al., 201416, they looked at twenty-six AD patients with FAF and OCT. They found that AD patients had some areas of hypopigmented (atrophic retinal changes) and hyperpigmented (lipofuscin heavy) areas in patches (see figure on right side below).
When curcumin (which has an affinity for beta amyloid) was given to the patient, hyperintense dots on FAF became more noticeable and were mostly found within the outer plexiform, ganglion and nerve fibers layers of the retina (see figure on left side below). Brain PET-CET on 21 out of 26 patients were consistent with AD and bilateral temporoparietal hypometabolism.
Figure 3 demonstrates FAF (left) and OCT (right) cross section in posterior pole showing hyperintensive dots in outer plexiform, ganglion and nerve fiber layer when curcumin was given to patient. Curcumin binds to beta-amyloid.

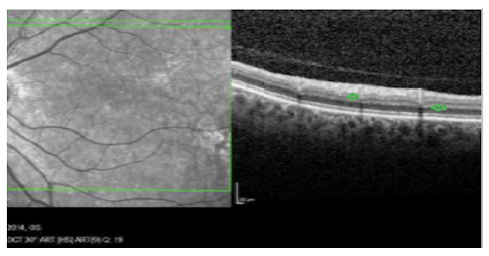
Figure 3 (Kaybasi et al., 2014)
In Figure 4, FAF shows areas of hypopigmented (atrophic retinal changes) and hyperpigmented (lipofuscin heavy) in posterior pole.

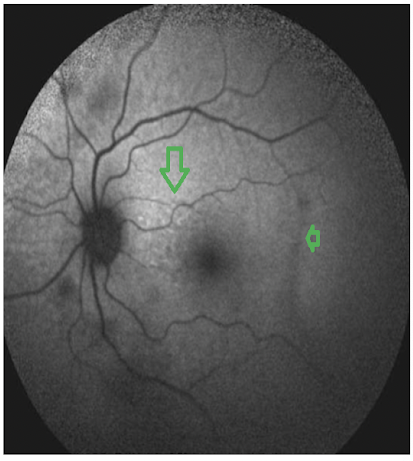
Figure 4 (Kaybasi et al., 2014)
The optometrist’s role in identifying Alzheimer’s disease
Most optometrists have the equipment necessary to test for both structural and functional visual changes in AD patients. Aside from OCTA, most OD’s have access to common ophthalmic imaging techniques such as OCT and FAF which can help identify physical structural changes in AD patients. When these structural changes are found, patients can be monitored or referred to neurology for a more thorough examination.
Also, patients who are known to have AD and glaucoma should be watched more closely as they are at risk for faster rates of progression.
When checking the patient in the chair, some tests that can be performed include refraction, EOMs, saccades, and color vision (monocularly and binocularly). Furthermore, as stated above AD patients tend to perform worse in low-contrast settings. Educating the patient and their caretaker can help improve reading and function of daily living.
One of the biggest impacts that we as optometrists can have on patients with AD is providing the best optical correction. This can help reduce visual hallucinations, improve hand-eye coordination and motility.
Some other treatment options that show potential benefit in studies are vitamin D and curcumin (component of turmeric). Researchers have found that antioxidants and anti-inflammatory substances can help slow AD and reduce cataract severity by slowing formation of beta-amyloid deposits.17 Furthermore, NMDA (N-methyl-D-aspartate) receptor antagonists (aka memantine) and cholinesterase inhibitors (such as galantamine and donepezil) have shown neurovascular protection that help to enhance cerebral blood flow.18
Billing and coding
The current CPT code used for OCT is 92134 which can also be used nowadays to code for OCTA. Therefore, if you perform both on the same day you likely will only receive reimbursement for one of the procedures. Therefore, it is best to bill these procedures on different days. The CPT code for FAF is 92250 which is also used for fundus photography. Unfortunately, you also cannot bill any form of fundus photos and OCT on the same day. In terms of diagnosis code, AD is coded as G30.9.
Referring to a neurologist
As of now there is no definitive way to diagnose AD through ocular changes. However, if some of these findings do appear in testing—whether a reduction in subjective testing (e.g., poor saccadic functions) or objective testing (e.g., bright highlighted deposits in the retina on OCT)—it may be worthwhile to reach out to the neurologist for further scans/testing and a more extensive neurological work-up.
Conclusion
Although Alzheimer’s research is still in the early stages, it is exciting to consider the potential of identifying biomarkers of this disease without invasive or post-mortem techniques. By utilizing common ophthalmic imaging techniques and testing available in most offices, optometrists may soon be on the frontlines of diagnosing neurodegenerative diseases, such as Alzheimer’s disease.
References
- Ferri CP, Prince M, Brayne C, Brodaty H, Fratiglioni L, Ganguly M, et al. Global prevalence of dementia: a Delphi consensus study. Lancet. 2005;366:2112-2117.
- Lakshminarayanan V, Lagrane J, Kean ML, Dick M, Shankle R. Vision in dementia: contrast effects. Neurol Res. 1996;18:9-15.
- Chapman FM, Dickinson J, McKeith I, Ballard C. Association among visual associations, visual acuity, and specific eye pathologies in Alzheimer’s disease: Treatment implications. Am J Psych. 1999; 156:1983-1985
- Wood S, Mortel KF, Hiscock M, Bretmeyer BG, Caroselli JS. Adaptive and maladaptive utilization of color cues by patients with mild to moderate Alzheimer’s disease. Arch Clin Neuropsychol 1997;12:483-489
- Simao LM. The contribution of optical coherence tomography in neurodegenerative diseases Curr Opin Ophthalmol 2013; 24: 521-527
- Sadun AA, Bassi CJ. Optic nerve damage in Alzheimer’s disease. Ophthalmol. 1990;97:9-17.
- Fletcher WA, Sharpe JA. Smooth pursuit dysfunction in Alzheimer’s disease. Neurology. 1988;38:272-277.
- Mudher A, Lovestone S. Alzheimer’s disease: do tauists and Baptists finally shake hands. Trends in Neuroscience. 2002;25:22-26
- Gilmore GC, Cronin-Golomb A, Neargarder SA, Morrison SR. Enhanced stimulus contrast normalizes visual processing of rapidly presented letters in Alzheimer’s disease. Vis Res. 2005;45:1013-1020
- Parisi V, Restuccia R, Fattapposta F, Mina C, Bucci MG, Pierelli F. Morphological and functional retinal impairment in Alzheimer’s disease patients. Clin Neurophysiol. 2001;112 (10):1860–1867. doi:10.1016/s1388-2457(01)00620-4)
- Song A, Johnson N, Ayala A, Thompson AC. Optical Coherence Tomography in Patients with Alzheimer's Disease: What Can It Tell Us? Eye Brain. 2021 Jan 8;13:1-20. doi: 10.2147/EB.S235238. PMID: 33447120; PMCID: PMC7802785.
- Cunha JP, Proença R, Dias-Santos A, et al. OCT in Alzheimer’s disease: thinning of the RNFL and superior hemiretina. Graefes Arch Clin Exp Ophthalmol. 2017;255(9):1827–1835. doi:10.1007/ s00417-017-3715-921
- Wang L, Murphy O, Caldito NG, Calabresi PA, Saidha S. Emerging Applications of Optical Coherence Tomography Angiography (OCTA) in neurological research. Eye Vis (Lond). 2018 May 12;5:11. doi: 10.1186/s40662-018-0104-3. PMID: 29796403; PMCID: PMC5956832
- Lahme L, Esser EL, Mihailovic N, et al. Evaluation of ocular perfusion in Alzheimer’s disease using optical coherence tomography angiography. JAD. 2018;66(4):1745–1752. doi:10.3233/ JAD-180738
- Valenti DA. Alzheimer's disease and glaucoma: imaging the biomarkers of neurodegenerative disease. Int J Alzheimer's Dis. 2011 Jan 5;2010:793931. doi: 10.4061/2010/793931. PMID: 21253485; PMCID: PMC3022203.
- Kayabasi U. Retinal examination for the diagnosis of Alzheimer’s disease. Int J Ophthal Pathol. 2014;03(04). doi:10.4172/2324-8599.1000145
- Mishra S, Palanivelu K. The effect of curcumin (turmeric) on Alzheimer's disease: An overview. Ann Indian Acad Neurol. 2008 Jan;11(1):13-9. doi: 10.4103/0972-2327.40220. PMID: 19966973; PMCID: PMC2781139.
- Guo L, Salt TE, Luong V, Wood N, Cheung W, Maass A et al. Targeting amyloidbeta in glaucoma treatment. Proc Natl Acad Sci USA 2007; 104: 13444–13449
- Melov S, Wolf N, Strozyk D, Doctrow SR, Bush AI. Mice transgenic for Alzheimer'sdisease beta-amyloid develop lens cataracts that are rescued by antioxidant treatment. Free Radic Biol Med 2005; 38: 258–261
