


As dry eye disease (DED) continues to be one of the most common conditions in our chairs, staying current with emerging research ensures that we continue to expand our clinical toolbox with accessible, innovative strategies.
Dry eye symptoms range from mild discomfort to significantly disrupted quality of life and vision. As digital device use rises, so does the incidence of DED.1,2 As a result, having a diverse, practical range of interventions is more critical than ever. An area of renewed emphasis involves blink exercises to improve ocular surface health and dry eye symptoms.3,4,5
For many of us in clinical practice, it is easy to default to artificial tears or prescription dry eye therapeutics as first-line recommendations. Recent research suggests blink training may meaningfully influence tear film mechanics, though its role in everyday patient care is still being defined.3,4,6
In this article, we will review the definition and epidemiology of DED, the physiological role of blinking, current research in blink exercises, and practical takeaways.
Current definition and statistics on DED
DED is defined as a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, accompanied by ocular symptoms.7
Key signs of DED include:
- Tear film instability
- Hyperosmolarity
- Ocular surface inflammation
- Neurosensory abnormalities of the cornea in more severe cases
Diagnosis relies on a combination of symptom questionnaires and objective testing (e.g., TBUT, osmolarity, and staining).8,9,10
Exploring the epidemiology of DED
It is estimated that DED affects 6.8% or 16 million US adults and up to 50% of adults globally.11 Risk increases with age, female sex, digital device use, and certain comorbidities, such as diabetes.
DED can disrupt daily activities like reading, driving, and computer use.5,6 With increased screen reliance, DED will remain a major health concern for eyecare providers to treat and manage.8,12
The physiological role of blinking in DED
Although the use of pharmacological therapy can have significant therapeutic effects on DED, at its core, blinking is an essential mechanism for maintaining ocular surface health and tear film stability.5
Blinking impacts DED through the following processes:5
- Complete blinking mechanically compresses the meibomian glands, releasing lipids that form the outer layer of the tear film to reduce evaporation and maintain homeostasis.
- Each blink spreads and redistributes the lipid, aqueous, and mucin layers of the tear film evenly across the eye, providing optical clarity and comfort.
- Blinking also clears debris, regulates drainage, and re-lubricates the cornea.
In DED, incomplete or decreased blinking rate leads to inadequate tear distribution, resulting in poor tear film stability, increased evaporation, and ocular surface damage. When the upper and lower eyelids do not fully meet, this results in an exposed portion of the lower cornea and can also reduce meibomian gland secretion and function over time.10
Additionally, prolonged use of digital screens has been shown to further reduce blink frequency and completeness, contributing to DED.3,13 What makes this particularly challenging is that incomplete blinking often occurs subconsciously. Many patients are unaware that their eyelids never make full contact, especially during concentrated visual tasks.
This underscores the importance of careful evaluation of eyelid positioning and epithelial dryness patterns during slit lamp examination. Taking an extra few seconds to take a closer look can help guide your patient education and potentially lead to recommendations for structured blink exercise training.3,9
Findings from recent studies on DED and blinking
New literature has provided insight into the relationship between blink patterns and their impact on DED. Incomplete blinking is associated with an increase in risk of DED development, higher symptom scores, greater meibomian gland dropout, and more pronounced ocular surface changes.3,10
Interestingly, blink completeness appears to be more influential on dry eye symptoms rather than the frequency of blinking in isolation.3 In other words, two patients may both blink 15 times per minute, yet, on average, the patient with incomplete eyelid closure may show a tendency towards more corneal staining, discomfort, and compromised tear film.
The blink quality, not just frequency, has a strong impact on tear film stability as previously discussed.3 As a result, this distinction has led some researchers to emphasize blink exercises as a potential avenue for addressing DED.3
A closer look at blink exercises
Structured blink exercises have reported potential benefits for DED patients. For example, in a prospective study published in 2020, participants performed a 10-second cycle of blinking exercises every 20 minutes during working hours for 4 weeks.3
Results showed significant improvements in symptom scores (based upon the Dry Eye Questionnaire and Ocular Surface Disease Index), tear breakup time (TBUT), and a reduction in the proportion of incomplete blinks.3
Recent research by Reiko Arita, MD, PhD, from The University of Tokyo, focused on the therapeutic potential of blinking exercises for DED.4 Specifically, the study evaluated the effects of blink exercises on palpebral fissure height, subjective symptoms, and tear film parameters.
Participants were instructed to perform blinking exercises as outlined below after instillation of artificial tears five times daily for 3 days. In short, the exercise movements target the orbicularis oculi and aim to strengthen both the superior and inferior sections.
The results showed that the blink exercise group reported significant improvements in:4
- Standard Patient Evaluation of Eye Dryness (SPEED) score and Visual Analog Scale (VAS) scores for eye strain and discomfort
- Enlarged palpebral fissure height
- Increased TBUT
- Reduced incomplete blink rate compared to the control group
As you may recall, SPEED is a commonly used, validated questionnaire designed to assess the frequency and severity of dry eye symptoms, including questions regarding dryness, burning, soreness, and fatigue over time.4
This study reports that even a short course of structured blinking exercises, combined with artificial tears, can result in meaningful improvements in symptoms and ocular surface health.4
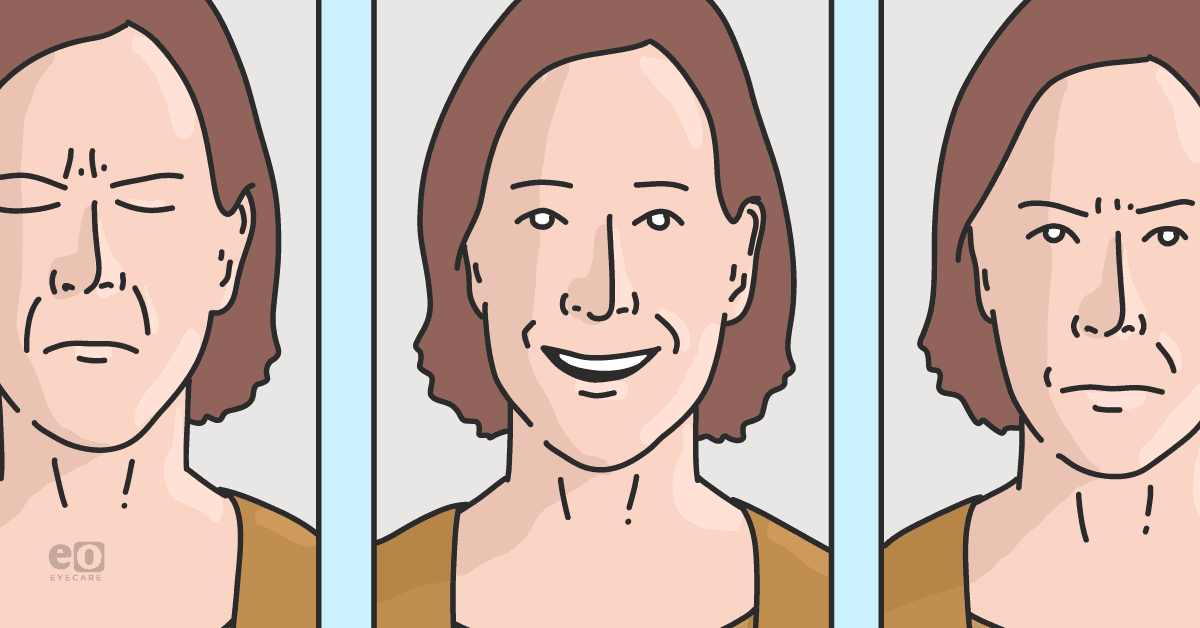
Figure 1: Graphic of blink exercises performed in Arita et al. The process consists of five exercises, including two normal blinks, gentle squeezing, dazzle appearance, and fox eyes.4 Video instructions can be found here.


Figure 1: Adapted from Arita et al.
Patient education and training for blink exercises
Given the self-performed nature of blink exercises, patient education can influence effectiveness if you choose to recommend them.
You may want to spend some time on the following:
- Discuss eyelid physiology and tear stability
- Teach and demonstrate the 5x daily blinking exercises
- Provide handouts or instructional videos
- Set appropriate timeline expectations and follow up with patients to monitor their symptoms
One strategy I recommend to improve patient compliance is framing these exercises as quick screen breaks rather than another health chore to remember. Though some studies suggest challenges with compliance, I still adhere to teaching the “20-20-20” rule, which suggests patients take a 20-second break every 20 minutes to look 20 feet away while using digital devices.14,15
Key takeaways
Here are five key takeaways from this article to bring back to your practice:
- Structured and consistent blink training can potentially be impactful for DED patients. The studies suggest that regular, defined blinking exercises can measurably improve symptoms and tear film metrics.
- Blink completeness outweighs frequency in terms of impact on DED. Be sure to check patients’ eyelid positioning and corneal integrity closely.
- Patient buy-in is heavily influenced by education and demonstration. Utilize your support staff to help reinforce the physiology and show them the exercises.
- Blink pattern analysis may become more commonly tracked in the dry eye realm.
- Most patients love a simple, no-cost intervention. Encouraging blink training may help support other dry eye treatments in your toolbox.
Conclusion
Blink exercises have been studied as a possible adjunctive approach alongside pharmacological therapy, targeting the core mechanics of tear film stability in DED.
While not a substitute for established treatments, the current evidence highlights an alternative perspective in dry eye management that may warrant further exploration.
For eyecare providers aiming to stay ahead, structured blink training offers an accessible, evidence-based addition to dry eye management worth further exploration.
