



Fuchs’ endothelial corneal dystrophy (FECD) is a common condition encountered by cataract surgeons when patients present for evaluation for surgery and carries significant implications for refractive outcomes.
Although estimates vary widely by study, depending on the demographics of the study, the overall prevalence ranges from 3 to 9% and is more commonly observed in females and Caucasians.1,2
The management of these patients has evolved substantially over the last decade, largely driven by advances in endothelial keratoplasty.
A brief overview of Descemet membrane endothelial keratoplasty (DMEK)
The introduction of Descemet membrane endothelial keratoplasty (DMEK) has transformed the standard of care by enabling faster visual recovery and more predictable refractive outcomes for this patient population.3
The presence of FECD has historically strongly influenced the choice of intraocular lens (IOL) at the time of cataract surgery, with advanced technology IOL (ATIOL) options being avoided owing to the unpredictable visual and refractive outcomes with previous keratoplasty techniques.
With the emergence of DMEK, surgeons have shifted their approach and are now able to treat this patient population with improved predictability of refractive outcomes and associated lower rejection rates, compared to other keratoplasty techniques such as Descemet stripping endothelial keratoplasty (DSEK).4
The anatomical endothelium-to-endothelium transplant with DMEK avoids the potential issues with the stromal interface with DSEK and allows for excellent quality of vision and quicker visual recovery.5
Improved visual acuity after DMEK versus DSEK is likely attributable to the increase in posterior corneal higher-order aberrations (HOA) observed in DSEK, which is not observed in patients after DMEK.6
Figure 1: DMEK intra-operative view: (a) 8mm descemetorhexis on the recipient eye and (b) the endothelial graft was inserted into the anterior chamber.


Using ATIOLs in patients with FECD
Multiple studies have been published reporting favorable outcomes evaluating the use of ATIOLs in patients with Fuchs’ combined with DMEK.7 However, if a patient is motivated for spectacle independence with an ATIOL, questions remain regarding the timing of surgery—whether DMEK should be performed in combination with cataract surgery or in a staged approach.
Although the DMEK procedure was initially thought to be refractively neutral, studies have demonstrated changes in total corneal power following DMEK alone that can be accounted for with a staged approach.8,9
DMEK and cataract surgery: Staged vs. combined approach
As mentioned, debate exists whether a staged or combined approach is superior for visual and refractive outcomes.10 Studies have been performed evaluating each approach with favorable outcomes. A study by Price et al. published in 2020 advocated for the staged approach with an average keratometry change of 0.26D with a wide range (-1.74 to +1.18D) following DMEK prior to cataract surgery.11
In this study, albeit a small sample size (n=16 eyes), favorable visual and refractive outcomes were reported with 81% of eyes achieving 20/25 or better UDVA and a median post-operative manifest refractive spherical equivalent refraction of 0.05D (range -0.75 to +0.75D).11
A later study from the same group in 2024 evaluated combined DMEK and cataract surgery with implantation of the light adjustable lens (LAL, RxSight, Inc.).12 In this study, the visual and refractive outcomes were largely favorable, with 81% of eyes within ±0.50D of target and 90% of eyes achieving 20/25 or better UDVA following the adjustment process with the LAL.
Weighing the pros and cons of a staged approach
The drawbacks to a staged approach include a longer recovery time and inherent risk associated with two separate procedures on each eye. Further, performing cataract surgery after the DMEK may introduce risk to the corneal transplant with potential endothelial cell loss of the graft and/or iatrogenic trauma to the graft during the subsequent procedure.
The main advantage of performing DMEK first, followed by cataract surgery after, is that DMEK offers the potential for improved IOL calculation accuracy because the cornea is no longer edematous and the refractive impact of the DMEK procedure is considered.10
Cataract surgery in FECD patients: Pearls from practice
In my own practice, I have found a staged approach to be the most reliable strategy for optimizing both visual and refractive outcomes in motivated patients with FECD. I typically perform DMEK in each eye first, allowing a minimum of 12 weeks of healing after the second eye before proceeding with cataract surgery and IOL implantation.
This interval provides time for corneal clarity to stabilize and for any refractive changes induced by the DMEK procedure to be incorporated into the subsequent IOL power calculations.
For IOL selection, I have used a range of IOL options with the staged approach in this population, including extended depth of focus (EDOF), trifocal, and the LAL. Based on my own experience, I now predominantly favor the LAL, as shown in Figure 2.
Figure 2: Retroillumination image of an eye with an LAL implant after DMEK.

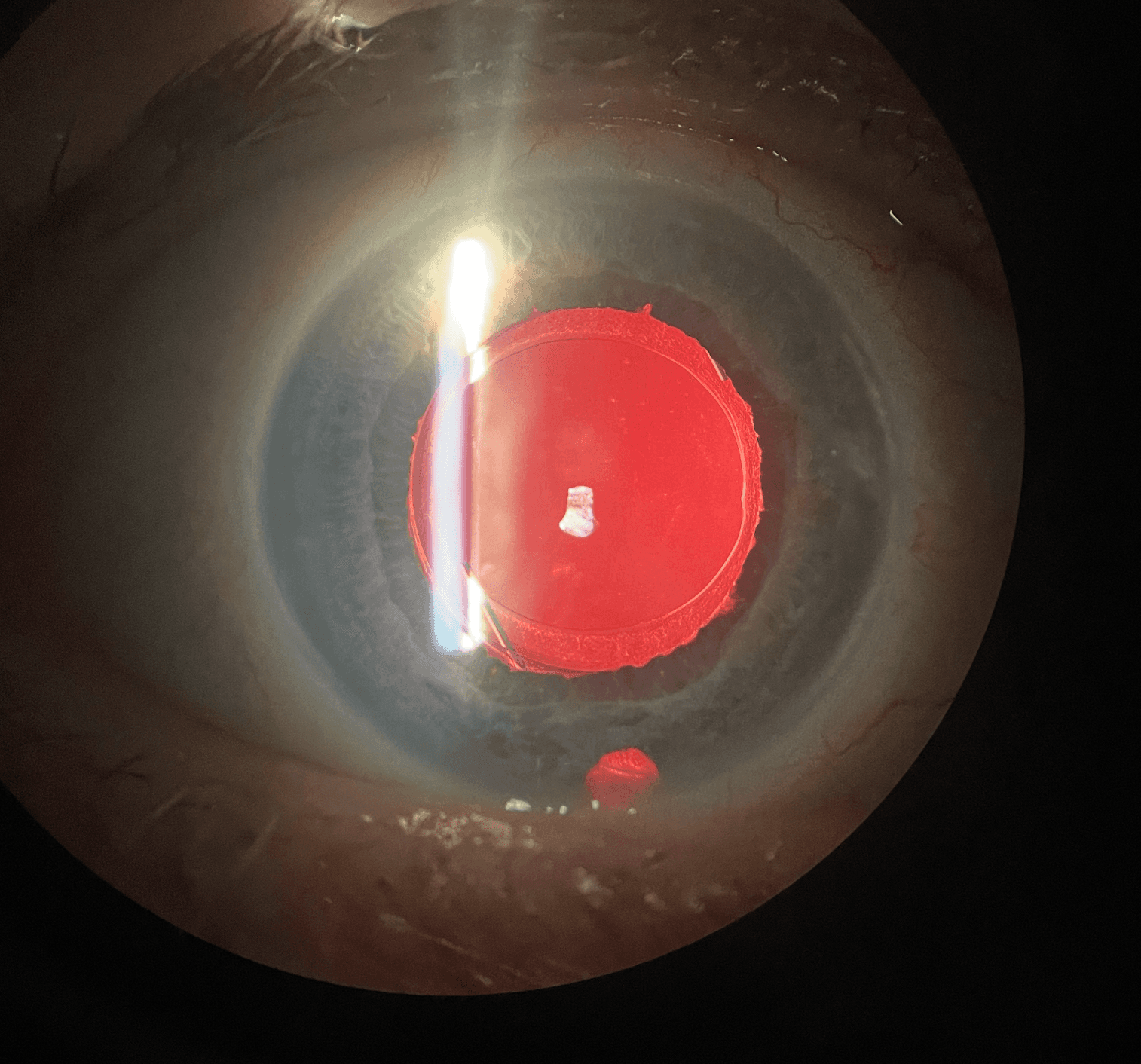
Figure 2: Courtesy of Tanner Ferguson, MD.
Despite the theoretical advantage of the LAL’s post-operative adjustability in a combined procedure, I have consistently observed superior predictability and patient satisfaction when the surgery is staged.
Prior to cataract surgery following the DMEK, I re-dilate these patients to confirm adequate pupil size for post-operative light adjustments, a necessary requirement for performing light adjustments with the light delivery device following surgery.
In terms of peri-operative management, I increase the topical steroid to three times daily during the first month following cataract surgery, then taper back to the scheduled drop regimen. This protocol has been effective for mitigating inflammation and supporting graft health.
A review of the results
For visual and refractive outcomes with the LAL in this population, the results thus far have been tremendous and exceed what has been previously reported with a combined approach utilizing the same IOL technology.12
This data is yet to be published, but in a series of 40 eyes from 20 patients undergoing staged DMEK-CEIOL with implantation of LAL, for uncorrected distance visual acuity (UDVA), 89% of eyes targeted for emmetropia (0.00D) were 20/20 or better, with 28% of eyes achieving 20/15 or better.
Overall, 100% of eyes in this series were 20/30 or better for UDVA. For refractive outcomes, the results were also impressive, with 92% of eyes within ±0.50D of target and 100% of eyes within ±1.00D of target. Overall, these results underscore the potential advantages of staging, even when utilizing adjustable IOL technology.
In conclusion
In summary, the evolution of endothelial keratoplasty, particularly with DMEK, has redefined the refractive management of patients with Fuchs’ endothelial corneal dystrophy.
With improved graft clarity and predictable corneal power stability, ophthalmologists can now confidently consider advanced IOL options, including the LAL, for these patients.
Although both staged and combined approaches yield excellent results, the staged strategy appears to offer superior precision in IOL calculations and visual predictability.
As clinical experience and outcomes data continue to expand, the integration of DMEK with modern IOL technologies promises even greater visual outcomes and patient satisfaction in the management of FECD.
