


Naturally, prior to space missions, astronauts undergo a wide range of medical tests to determine their fitness to fly as well as establish baselines for the effects of space on each anatomical system.
Before, during, and after flight, astronauts are assessed and monitored with routine imaging to evaluate for spaceflight-associated neuro-ocular syndrome (SANS), an ocular condition identified in astronauts after space missions.
SANS is characterized by disc edema, choroidal folds, globe flattening, and induced hyperopia. The longer the mission, the more likely the astronaut is to show signs or have symptoms of this condition. Retrospective examination of retired astronauts has shown the condition is not new, just more recently on the radar.
This article will introduce this interesting condition, along with potential long-term sequelae and current research aimed toward preventing these ocular changes.1
A history of spaceflight-associated neuro-ocular syndrome
During the earliest space flights in the 1980s, subjective in-flight visual changes were documented. Since the flights were of short duration, most symptoms reported were brief and not severe.2
Research dating back to 1987 attempted to simulate the impact of microgravity on the eye. This early research showed that intraocular pressure (IOP) increased in a head-down-tilt position that simulated microgravity and that certain individuals could be predisposed to hypoperfusion effects of microgravity over others.3
The term first coined for the changes was VIIP (visual impairment and intracranial pressure syndrome) since the proposed mechanism was an increase in intracranial pressure.2
SANS, as we currently know it, was described in 2011 after studying a small sample of seven US astronauts pre- and post-long duration space flight.1 Choroidal folds, disc edema, cotton wool spots, and increased optic nerve sheath cerebrospinal fluid were noted after the longer duration flights. The neuro-ocular effects led to the renaming of the condition to SANS.3
SANS and long-duration space flight
In the late 1980s, a survey of 300 astronauts found that roughly a quarter of astronauts who completed short-duration spaceflight and about half of those who completed long-duration spaceflight reported subjective visual changes.2 Data supports a cumulative effect from repeat missions and that men may be more likely to experience effects than women.2,3
The effects of long-duration space flight continue to be better characterized through the modernization of multimodal ophthalmic imaging, magnetic resonance imaging (MRI), and ultrasound.3 Further, the increasing sample size of astronauts over time has also helped research in this area to progress since a small sample size in the field of spaceflight has been a major limitation in obtaining quality data.
Recent data from the National Aeronautics and Space Administration (NASA) suggests up to 70% of astronauts experience SANS in some form.4
A clinical picture of SANS
SANS is characterized by clinical signs of disc edema, choroidal folds, and globe flattening—which can be unilateral or bilateral. The globe flattening leads to hyperopic refractive shifts and can be accompanied by a symptom of blurred vision.5
Blurred vision at near is most common in astronauts over the age of 40 and plus-powered readers have been made available on the International Space Station in anticipation of the change, being called “spaceflight glasses.”3 If blurred vision is not present, the patient is often asymptomatic. More rarely, cotton wool spots and pigment epithelial detachments (PEDS) have also been noted.5
Comparing IIH and SANS
SANS has been compared to idiopathic intracranial hypertension (IIH); however, the symptoms and demographics are not similar. Headaches, pulsatile tinnitus, and vision obscurations, which are hallmarks of IIH, are rare with SANS. Also different is that on lumbar puncture, SANS has normal or only a slight increase in pressure as opposed to more pronounced increases seen with IIH.2,5
Sibony et al. studied disc edema in eyes with IIH versus SANS and found several differences. One was a disparity in the severity of disc edema, with IIH causing significantly more optic disc swelling when compared to SANS.
Another difference was the deformation in the peripapillary shape of Bruch’s membrane, which was anteriorly displaced in the majority of IIH cases but not SANS cases. This supports the hypothesis that SANS has a more complex pathogenesis than solely an increase in intracranial pressure.6
Figure 1 demonstrates a fundus photograph of blurred disc margins characteristic of disc edema commonly present with SANS (Note: Not from actual SANS patient).

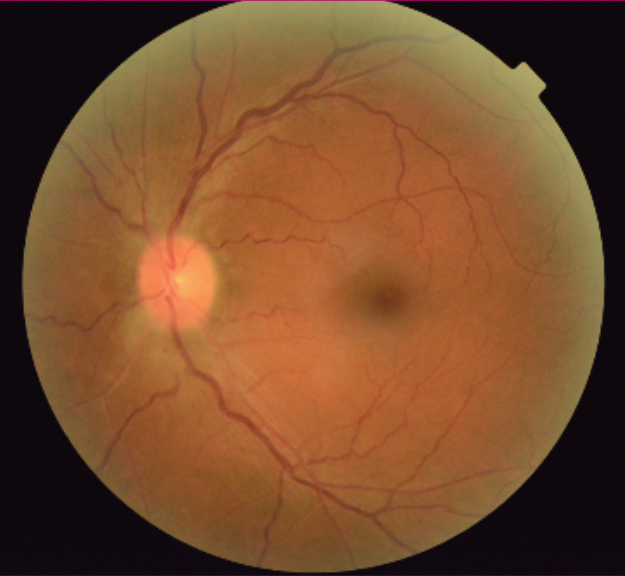
Figure 1: Courtesy of Danielle Kalberer, OD, FAAO.
The choroidal folds on macular optical coherence tomography (OCT), seen in Figure 2, are also commonly present with SANS (Note: Not from an actual SANS patient).

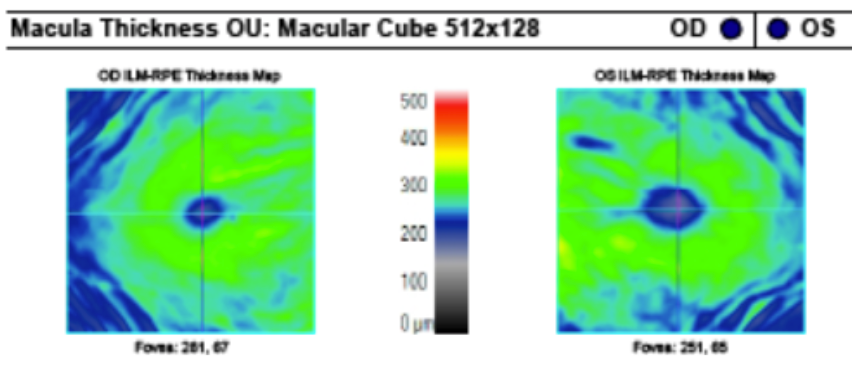
Figure 2: Courtesy of Danielle Kalberer, OD, FAAO.
Etiologies of SANS
Multiple factors likely contribute to the neuro-ocular changes associated with spaceflight. The most supported hypothesis is a shift in fluid from the lower body and extremities to the head due to gravitational change in a microgravity environment.4
Impaired CSF, lymphatic, and vascular drainage
In our normal environment, cerebrospinal fluid (CSF), lymph, and blood flow are assisted through circulation by the gravitational pull. When the environment is changed to microgravity, fluid flow is no longer assisted in that same way, leading to a slower flow velocity and congestion.2
The shift of cephalic fluid upward, along with outflow resistance, results in increased intracranial pressure, venous and lymphatic stasis, and tissue edema.5 Increased cerebral venous pressure in the head, along with decreased CSF absorption and enlargement of the 3rd and 4th ventricles, has been documented after long-duration spaceflight.
It is thought that the increase in CSF pressure is transmitted down the optic nerve to impact the ocular structures.3 The increase in intracranial pressure can result in optic nerve sheath expansion and axoplasmic stasis.1 Another factor in disc edema could be the compartmentalization of CSF within the sheath of the optic nerve.7
The venous congestion can specifically impact cerebral and ocular venous flow, including in the vortex veins, which are responsible for the outflow of most of the ocular blood supply. Similarly, the choroid can experience congestion, causing an increased thickness and foveal displacement, leading to a hyperopic refractive shift.2 The axial length decrease documented pre- and post-flight is thought to be due to the pressure of CSF behind the globe.3
Microgravity and the glymphatic system
A more recent hypothesis for pathogenesis relates to the glymphatic system. CSF transport and drainage of excess interstitial fluid occur through this system. Much like the other fluid pathways discussed, this system is reliant on a pressure gradient and assisted by gravity.8
In simulated scenarios of head-down-tilt to mimic microgravity, the lymphatic drainage system was temporarily impaired. Similar results occurred when patients were placed in a supine position. It is proposed that slowed lymphatic drainage can also impact overall fluid dynamics and autoregulation systems in the body as well.3
There are additional factors like elevated ambient carbon dioxide within the space station, exposure to radiation, and the use of certain inflight resistive exercise devices that could play a role in SANS. None of these mechanisms of pathogenesis alone are thought to be mutually exclusive—experts agree an interplay is most likely.2
Evaluation of spaceflight-associated neuro-ocular syndrome
The International Space Station is equipped with imaging systems, like orbital ultrasound and MRI. Specific eye exam testing, including visual acuity, Amsler grid, tonometry, fundus photography, and ophthalmoscopy, are also regularly performed.
The availability of this testing has been instrumental in detecting and monitoring the changes associated with SANS. Axial length measurements pre- and post-flight have provided evidence of globe flattening alongside MRI and ultrasound.1 Refractive error has been measured in flight with autorefraction.3
A questionnaire is also performed by the astronauts regularly during spaceflight to gauge any changes they have noticed related to vision and the severity of the changes. A few examples of items on the questionnaire are difficulty focusing, difficulty with contrast/lighting, headache, nausea, double vision, and vision loss.4
Monitoring SANS patients for disc edema
One large concern for long-term ocular sequelae is disc edema. Prolonged edema can lead to permanent visual field changes, such as enlargement of the blind spot. Serial visual field tests on astronauts returning from flight will give more information about recovery and prognosis in this area.
Cycloplegic refractions up to 10 years following spaceflight have shown evidence of permanent refractive shifts. Acquired choroidal folds did improve after mission completion in some cases, but it persisted for several years after spaceflight in others.4
Artificial intelligence (AI) has great potential to advance knowledge and offer early detection of SANS. There is often a lag in data sharing from diagnostics on the space station, which could delay diagnosis and intervention.
AI algorithms are able to process data quickly and pick up subtle changes to ocular anatomy. With the right algorithm, an AI device could learn to detect patterns characteristic of SANS to alert astronauts of the change in real-time.8
Current interventions to manage SANS
Treatment for SANS involves treating the symptoms as they occur while in flight and monitoring the signs post-flight for resolution. The refractive shift, which is the most likely to cause symptoms, is alleviated by making plus power reading glasses available during flight.3
Counteracting bodily fluid displacement
Current research for interventions focuses on ways to correct fluid displacement. Countermeasures could be on the individual level or modifications to the space station environment. Thus far, thigh cuffs and negative pressure suits have been successful.
These lower-body negative-pressure devices help keep blood and fluid in the lower part of the body and promote equal distribution of fluid throughout the length of the body.2 Pressurized goggles have been proposed to specifically counteract the effects of SANS (i.e., an anteriorly displaced pressure gradient).3
Medical therapies and environmental changes
Medication therapies are an option but are considered risky because it can be difficult to predict adverse medication effects that may arise due to microgravity-related physiologic changes.3
Of note, the coenzyme Q10 (coQ10) is under investigation by the Italian Space Agency in relation to retinal and ocular protective properties.2 Higher levels of vitamin B have also demonstrated a protective effect against more severe levels of SANS.8
Environmental modifications like decreasing ambient carbon dioxide levels and radiation exposure in the space station are being investigated. Current research in this area has yielded mixed results on whether this could sufficiently prevent SANS alone since these may be instigating factors rather than the most causative factors.3
Another proposed environmental intervention is to introduce periods of intermittent artificial gravity. A centrifuge device could be used daily to reintroduce gravity and counteract the constant increased fluid pressure in the superior aspect of the body.2
NASA research on SANS
NASA’s Cross-Cutting Computational Modeling Project uses computer models to try to understand the impact of microgravity on the body and the eye. By altering parameters and changing fluid dynamics, researchers hope to better characterize the physiologic changes that occur to the cardiovascular, central nervous, and visual systems in the space environment.9
Additionally, NASA’s Human Research Program recently awarded a grant to researchers from the Department of Ophthalmology at Indiana University School of Medicine to develop a translaminar eye model for SANS countermeasure testing. Dr. Sharma, the lead in project development, is also working with a team to send donor eyes to the moon to study the impact on the eye.10
In conclusion
SANS is a result of the human body being subject to a microgravity environment not typical of its physiology. NASA continues to monitor astronauts retrospectively and prospectively to learn more about the mechanism and how long-term consequences can be prevented.5
Research to develop SANS countermeasures is an important part of safeguarding the ocular health of astronauts as space missions become longer and as astronauts deploy on repeat missions.
