


For this month’s edition of this column, I wanted to switch gears a bit. Now that we have reviewed many common conditions such as AMD, VMT, macular hole, and diabetic retinopathy, let’s jump into a few cases of rarer conditions.
If there are any specific topics or conditions that you would like me to cover, send me an email at daniel.epshtein.od@gmail.com and we’ll put it on the list for future editions!
A torpedo appears in an optometrist’s office
A 54-year-old male was referred by his PCP for a diabetic eye exam. He was diagnosed 4 months prior and his latest A1C was 7.3%. He denies any other pertinent medical or ocular history and reports that this is his first eye exam. His entering distance acuities were 20/25 OD and OS which improved to 20/20 with a mild hyperopic prescription.
Externals and anterior segment were unremarkable. IOP was 17mmHg OD and OS. Upon dilation, his right eye was noted to be unremarkable but the below lesion was noted in his left eye. Multimodal imaging as seen below was ordered.
An ovoid, flat, mostly hypopigmented lesion was noted temporal to the fovea. Irregular hyperpigmentation was scattered throughout the lesion. Retinal vessels were visualized overlying the lesion but no irregular vasculature was noted. Due to the typical appearance and location at the temporal horizontal raphe, torpedo maculopathy was primary tentative diagnosis. Chorioretinal scarring and CHRPE were also considered.
In Figure 1, a large torpedo maculopathy lesion is noted temporal to the fovea. Fundus autofluorescence reveals a predominately hypo-autofluorescent lesion.

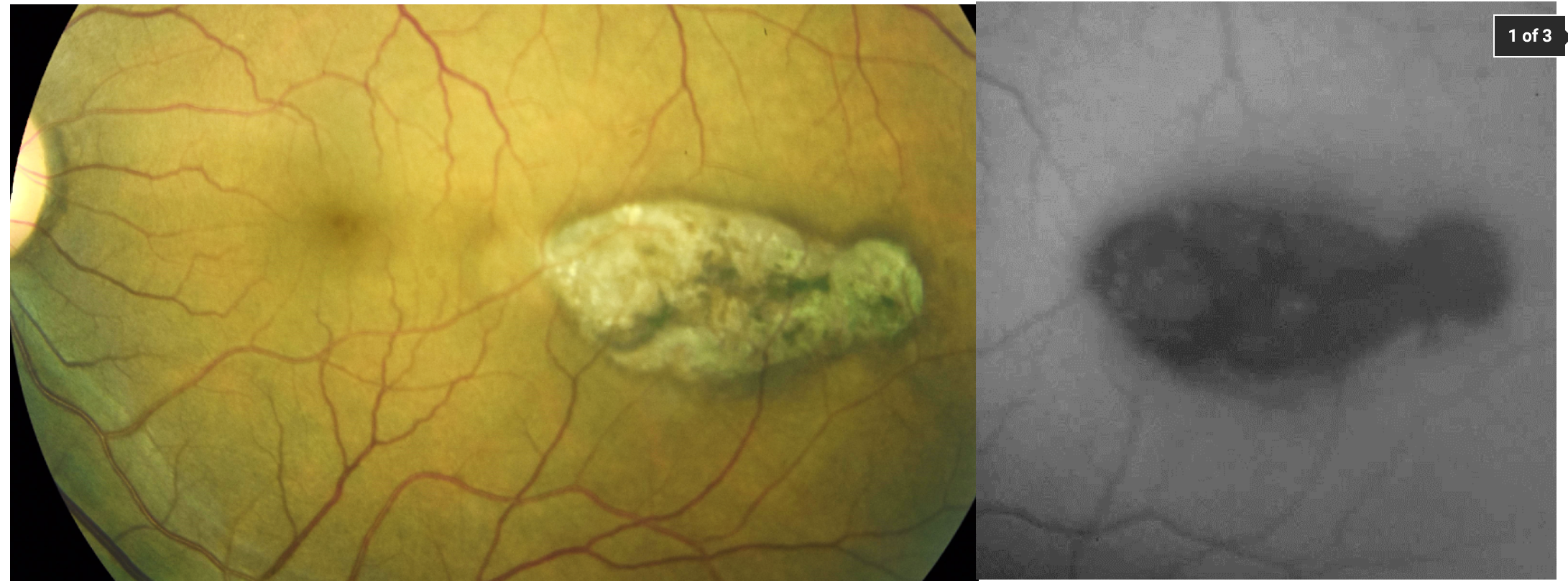
Figure 1
Fundus autofluorescence imaging revealed hypo-autofluorescence corresponding to the entirety of the lesion. No hyper-autofluorescence was noted, suggesting that this was an inactive lesion. OCT imaging confirmed that this lesion was typical of torpedo maculopathy. A prominent subretinal cleft/outer retinal cavitation was evident.
Thinning of the outer nuclear layer and loss of both the ellipsoid zone and interdigitation zone were noted throughout the lesion. The inner retina was seemingly intact. The choroid was easily visualized due to increased signal transmission secondary to attenuation of the overlying RPE. Choroidal excavation/thinning was noted within the center of the lesion.
Figure 2 illustrates OCT imaging of the lesion reveals a subretinal cleft without RPE and outer retinal degeneration. The choroid is thinner in the center of the lesion.

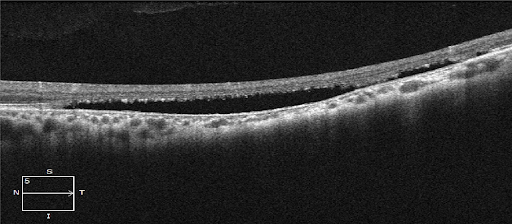
Figure 2
After review of the multimodal imaging, the retinal lesion was thought to be torpedo maculopathy. Though chorioretinal scarring and CHRPE were considered in the differential diagnosis, OCT clearly showed that this lesion was not a CHRPE and the subretinal cleft was typical of torpedo maculopathy. Chorioretinal scarring was ruled out due to a lack of overlying vitreal debris and symptoms suggestive of a past chorioretinitis. Based on the OCT findings of a subretinal cleft and intact inner retinal, this lesion was classified as type 2 torpedo maculopathy.
Since this was an incidental lesion with no previous documentation, I scheduled the patient to follow up in 2-3 months to ensure that the lesion was stable. I discussed the use of an Amsler grid and the importance of urgent follow up if he noted any vision changes. Repeat fundus examination and OCT imaging was stable. The patient was asked to continue self-monitoring of his vision and follow up in 1 year, with strict return precautions to follow up urgently if he notices any changes in his vision.
Torpedo maculopathy
Torpedo maculopathy is characterized by a solitary hypopigmented or mixed hypopigmented-hyperpigmented torpedo shaped lesion temporal to the fovea, at the level of the horizontal raphe. These lesions are longer horizontally than they are vertically and are most often found incidentally. Due to their often non-foveal position, visual acuity is not affected though a corresponding visual field defect may be present.
Due to disruption of the RPE and outer retinal, rare cases of choroidal neovascularization have been reported.1
These lesions are thought to be congenital and nonprogressive, though the exact pathophysiology of torpedo maculopathy is still unknown. Various theories propose that developmental defects of the RPE or choroidal vasculature give rise to the characteristic lesion.
Wong et al developed an OCT based classification system which distinguishes the two types of torpedo maculopathy lesions based on the presence of a subretinal cleft and amount of outer retinal degeneration.2 A third subtype, with inner retinal depression and excavation has been proposed but no unifying classification system has been created.3,4
| Classification | OCT Findings |
|---|---|
| Type 1 | Inner retina: Unremarkable |
| Outer retina: Attenuation of interdigitation zone and ellipsoid zone, thinning of outer nuclear layer | |
| Subretinal cleft/Outer retinal cavitation: Absent | |
| Choroid: Intact architecture but increased OCT signal transmission | |
| Type 2 | Inner retina: Unremarkable |
| Outer retina: Loss of interdigitation zone and ellipsoid zone, thinning of outer nuclear layer | |
| Subretinal cleft/Outer retinal cavitation: Present | |
| Choroid: +/- Inner choroidal excavation, increased OCT signal transmission | |
| Type 3 | *Type 3 Torpedo Maculopathy lesions are poorly described in the literature* |
| Type 1 or 2 lesion with inner retinal depression and excavation |
Fundus autofluorescence findings in torpedo maculopathy are variable and depend on the amount of RPE degeneration. Typically, the lesions are predominately hypo-autofluorescent due to the significant amount of RPE degeneration. Areas of hyper-autofluorescence may also be noted and typically correlate to areas with a more intact RPE.
Perimetry is not routinely ordered for patients with torpedo maculopathy but macular perimetry or microperimetry will reveal significant sensitivity reductions due to loss of RPE and photoreceptors. Areas of the torpedo lesion with minimal degeneration will have mild visual sensitivity deficits.
Torpedo maculopathy is a rare startling finding with minimal consequence. Using OCT, this lesion can be easily differentiated from potentially vison threatening disease. Once diagnosed, torpedo maculopathy can be safely monitored and referred for treatment in the extremely rare instances of choroidal neovascularization.
References
- Shirley, Katherine, et al. "Torpedo maculopathy: disease spectrum and associated choroidal neovascularisation in a paediatric population." Eye 32.8 (2018): 1315-1320.
- Wong, Evan N., et al. "Novel optical coherence tomography classification of torpedo maculopathy." Clinical & experimental ophthalmology 43.4 (2015): 342-348.
- Venkatesh, Ramesh, Bharathi Bavaharan, and Naresh K. Yadav. "Multicolor imaging findings in torpedo maculopathy." Indian journal of ophthalmology 67.2 (2019): 295.
- Tripathy, Koushik, Barsha Sarma, and Shahana Mazumdar. "Commentary: Inner retinal excavation in torpedo maculopathy and proposed type 3 lesions in optical coherence tomography." Indian journal of ophthalmology 66.8 (2018): 1213.
