



The cornea is the most heavily innervated tissue in the human body, lending it to be one of the most sensitive.1 A functioning sensory innervation allows the cornea to maintain an adequate metabolic environment and provides a protective environment for tear production and the blink reflex. This environment encourages additional growth factors to promote rapid healing.
Neurotrophic keratopathy (NK) is a degenerative corneal disease of the trigeminal nerve (fifth cranial nerve), which is responsible for providing afferent input via the terminal ophthalmic nerve branch. When impaired, corneal sensitivity is reduced. NK results in spontaneous epithelium deterioration and poor corneal healing.
Overview of perforated neurotrophic corneas
A wide variety of etiologies can potentially affect the nerve, such as herpetic keratitis, diabetes mellitus, multiple sclerosis, vitamin A deficiency, ophthalmic and neurosurgical procedures, and physical and chemical injuries.2,3,4,5
NK has also been associated with contact lens usage, tumors, leprosy, specific corneal dystrophies, and rare congenital conditions, such as familial dysautonomia and familial corneal hypoesthesia, to name a few.3,4
This ocular condition affecting the integrity of the epithelium can fall on a spectrum:
- Mild: Epithelium and tear film changes; “stage 1”
- Moderate: Non-healing epithelial defect; “stage 2”
- Severe cases: Stromal melting and perforation; “stage 3”
The Mackie Classification is based on the three stages and is widely used in diagnosing and managing NK.5 This article will focus on the presentation and management of the severe case or stage 3 of NK: perforation of neurotrophic ulcer.
Diagnosing stage 3 NK or a perforated neurotrophic cornea
The diagnosis is based on clinical history, including any conditions affecting the fifth cranial nerve causing impairment, as mentioned earlier, the presence of ulcers or persistent epithelial defects (PED), and corneal sensitivity loss.
Due to poorly functioning corneal nerves, patients with NK are rarely symptomatic with pain, regardless of the stage of the disease. This highlights the relatively classic inconsistency between clinical presentation and patient symptoms.2,3 Symptoms of visual impairment will manifest when central corneal involvement is noted.6
However, in the early stages of NK, symptoms of dryness, photophobia, curtailed reading time length, and reduced blink rate can be present.6 There may be occasional complaints of blurred vision, which may be due to severe dryness, epithelial defect, stromal haze/scarring, or corneal edema. Other conditions, such as immune and infectious keratitis, should be on the differential diagnosis when NK is suspected.3
An approach to the general exam is as follows:
Neurologic examination
Assess all cranial nerve functions. A neurological exam can localize to the trigeminal nerve, but additional cranial nerve involvement, such as the third and sixth nerves, can be affected and should be tested.
Ophthalmologic examination
An ophthalmologic examination can include an external examination (eyelids and conjunctiva) and slit lamp examination (i.e., cornea, iris, anterior chamber). The eyelids should be examined for diagnosis and prognosis. For example, examining for lagophthalmos could reveal further cranial nerve involvement and related exposure keratitis, which can worsen keratopathy and contribute to stromal melt related to NK.
Further, a conjunctival assessment should be performed. Conjunctiva may be less inflamed than expected with a corneal epithelial defect or ulceration. Any subconjunctival fibrosis should be noted as it relates to any chronic autoimmune or severe dry eye disease.
In addition, corneal epithelial changes should be quantified. Such changes are frequently noted in the central area. Neovascularization and scarring will highlight a record of old infections or recurrent corneal ulcers. The anterior chamber should be examined for the presence of any inflammatory reaction, such as flare, keratic precipitates, cells, or hypopyon.
Vital dye staining
Fluorescein and lissamine green dyes aid in visualizing changes in the corneal epithelium and conjunctiva.
Diagnostic testing
Assessing corneal sensation is essential to diagnosing NK. This can be measured and performed by different methods. One method uses a cotton wisp, which is applied to both corneas. The patient’s bilateral reaction is documented.
Cochet-Bonnet aesthesiometer
The Cochet-Bonnet aesthesiometer is a semi-quantitative measurement via a contact instrument. This method uses varying lengths of a nylon filament (from 5mm to 60mm) to contact the cornea at different applied forces to observe the patient’s subjective reaction.
Once the filament makes contact with the cornea, pressure is applied to create a bend by which the patient typically senses the filament tip. The filament length is reduced in 5mm increments until the patient can appreciate the sensation. For example, if a patient notes filament sensation at a longer length (i.e., 45mm compared to 10mm), the patient has a higher corneal sensitivity threshold.
Belmonte non-contact gas aesthesiometer
Another semi-quantitative measurement is the Belmonte non-contact gas aesthesiometer (BNGA). Unlike the Cochet-Bonnet aesthesiometer, the BNGA prompts the cornea via a calibrated gas emission from an injector at close range to the cornea. The patient’s subjective blink response is observed.
The BNGA is placed on the slit lamp while the gas injector tip is maintained perpendicular to the cornea (5mm from the surface using a transparent ruler). The patient is instructed to fixate on a target. The patient will open and shut their eyes before activating the stimulus.
The gas’s temperature, flow, and composition (i.e., CO2 concentration) are changed, in turn assessing different aspects of corneal sensation, such as mechanical, chemical, and thermal sensitivities.6
Corneal nerve imaging
In vivo confocal microscopy (IVCM) is a diagnostic test to measure corneal nerve health, among other things. While confocal microscopy may not be available outside of academic centers, it can be a helpful adjuvant when the diagnosis is unclear or when other etiologies are being considered (such as acanthamoeba keratitis).
Severe NK, examined by IVCM, may appear to have less nerve density as compared to normal corneas. In addition, there may be a decrease in epithelial and endothelial cell density and an increase in hyperreflective keratocytes in comparison with normal eyes.6
Anterior segment optical coherence tomography (AS-OCT)
This test can help measure corneal thickness changes. It is helpful in determining which cases are at high risk for perforation, as well as monitoring for progressive stromal thinning.
General management of a perforated neurotrophic cornea
NK is a degenerative disease process that can result in loss of vision and even the eye if not treated. The focus of therapeutic interventions for stage 3 NK is on ulcer healing and avoiding corneal perforation. Corneal perforation requires prompt management to save the globe and restore vision.
Treatment can be divided into medical, non-surgical, and surgical interventions. Frequently, management is approached in a stepwise manner based on NK staging and severity.
Medical management of a perforated neurotrophic cornea
Medically managing NK depends on the staging and severity, and the types of treatment are geared toward the clinician’s specific goal, such as treating the underlying pathology, preventing progression, and reducing inflammation.
Options for medically managing stage 3 NK include:
- Suspend therapies with preservatives: Discontinue any ocular treatment for sterile ulcers with preservatives—preservative-free formulations are preferred in these compromised eyes.
- Reduce inflammation: Avoid irritating and inflammatory cosmetics around the eyes. In addition, increase moisture by wearing protective and insulating glasses as well as increase dietary omega-3 fatty acids for anti-inflammatory benefits.
- Use preservative-free drops: Initiate frequent preservative-free artificial tears.
- Try targeted medical therapies: Start a trial of innovative therapies such as Cenegermin (recombinant human nerve growth factor). It is the first FDA-approved medication for treating patients with NK suffering from corneal ulcers and persistent defects.5
Non-surgical management of stage 3 NK
- Eyelid closure: Tarsorrhaphy is the hallmark of NK management. Alternative non-surgical techniques to tarsorrhaphy are eyelid closure with tape, pressure patching, pad and bandage, and ptosis induction via botulinum toxin injection.6
- Therapeutic contact lenses: Silicone hydrogels, limbal, semi-scleral, or scleral lenses are commonly used. The prosthetic replacement of the ocular surface ecosystem (PROSE) device is a fluid-ventilated, gas-permeable lens that permits customization of the corneal vault, which is the distance between the posterior surface of the optic zone and the cornea.7
- Devices using both amniotic membranes as well as a combined amniotic membrane with a contact lens are common among cornea practitioners. OmniLenz and Prokera are two examples of this type of advanced device.6
- Punctal occlusion: Punctal plugs, which can be temporary or permanent, are an option to help increase tear volume and lubrication of the ocular surface. Other options include permanent occlusion with thermal cautery, closure using an argon laser, suturing the punctum, or canalicular ligation.6
Surgical management of stage 3 neurotrophic keratopathy
Surgery is often necessary for advanced stages and disease refractory to medical management. Medical and surgical options are not independent of one another and are typically started simultaneously.
Options for surgically managing stage 3 NK include:
- Permanent punctal occlusion: This is beneficial in patients requiring lifelong punctal occlusion.
- Tarsorrhaphy: This can be temporary or permanent and partial or complete, depending on the severity and etiology of the condition. The location of tarsorrhaphy to be performed should be considered as well (i.e., lateral, medial, central). Lateral tarsorrhaphy aims to neutralize upper lid retraction with the lower lid laxity.8,9
- While it may be underutilized, medial tarsorrhaphy sews the canicular portions of the eyelids, which contrasts with the lateral technique because there is no eyelash involvement. As a result, the eyelid can be inverted without prompting ocular irritation; plus, it spares peripheral vision, however resulting in decreased central vision.9
- Among the various methods of performing tarsorrhaphy, the most common is suturing the eyelids to one another over foam bolsters. Lateral tarsorrhaphy allows some functional vision and is often easier for patients to be able to apply their eye drops.
- Lateral tarsorrhaphy also allows the eyecare professional to examine the patient’s eye more easily. Total or near-total tarsorrhaphy may be reserved for refractory cases.
- Debridement: Expanding the size of the defect in a sterile manner when there is an adjacent epithelial ridge can promote healing by allowing migration of the epithelium to close the defect.6
- Amniotic membrane transplantation (AMT): This has been proven to be effective in stage 3 NK. AMT can be used as a graft or a patch. Available amniotic membranes are cryopreserved (Amniograft), freeze-dried (Ambio dry), and vacuum-dried (Omnigen).6
- Tissue adhesives: For small perforations (<3mm), using tissue adhesives with a soft bandage on the lesion is the preferred method. Larger perforations necessitate conjunctival flaps or lamellar keratoplasty. Synthetic (cyanoacrylate) and biologic (fibrin glue) are two types typically used.6
- Conjunctival flap: A conjunctival flap is often used to prevent progression to perforation. They replace the damaged stromal bed with healthy basal tissue on which epithelium can develop. The conjunctival flap provides a blood supply to the defective cornea, which offers serum-based growth factors.
- Vascularized structures are more resistant to perforation as well. Additionally, conjunctival flaps are particularly useful due to their ability to stop the inflammatory process and remove the dependency on frequent medication instillation.6
- Corneal transplantation: Tectonic corneal transplants are considered once there is a failure of medical and other surgical management. A tectonic transplant is performed on perforated corneas or those with impending further perforation or melt.
- An amniotic membrane can be placed on the tectonic graft to promote further healing. A suture tarsorrhaphy may also be placed simultaneously to promote epithelialization and less exposure of the ocular surface during the postoperative period.
- Direct neurotization: This option involves utilizing the patient’s (or a donor’s as first described by Terzis and her colleagues) contralateral supraorbital and supratrochlear branches of the ophthalmic division of the trigeminal nerve. Once the nerve is obtained, it can then be inserted at the limbus of the affected eye.
- This is used to restore corneal sensitivity. It is a newer procedure with the goal of maintaining anatomical integrity, preserving a cosmetic appearance, and regenerating nerve function.6,10
Following up with NK patients
Stage 3 NK patients should be monitored very closely. For patients who may be unable to self-administer eye drops or where there are concerns about follow-up, hospitalization may be considered to provide an additional level of oversight and care.
A perforated neurotrophic cornea case report through images
A 74-year-old male with a complex ocular history, including chronic iridocyclitis, steroid-induced glaucoma, corneal failure s/p penetrating keratoplasty, limbal stem cell deficiency s/p keratolimbal allograft transplantation, and neurotrophic keratopathy presented with a recurrent epithelial defect.
Figure 1 demonstrates persistent epithelial defect in a patient with history of limbal stem cell disease s/p keratolimbal allograft transplantation and subsequent penetrating keratoplasty. This epithelial defect persisted despite lateral tarsorrhaphy, amniotic membrane transplantation x 3, and elimination of all preserved eye drops.

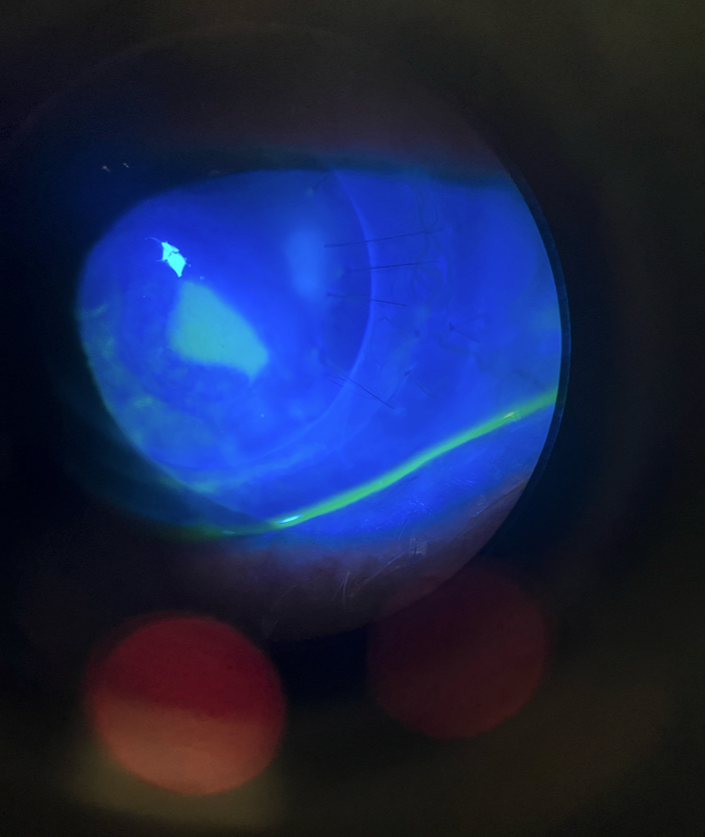
Figure 1: Courtesy of Mina Farahani, MD, MS, MS.
In Figure 2, the patient presented with a corneal perforation about 3 months after the initial epithelial defect, despite medical management. Given this, the patient was taken to the operating room the same day for tectonic penetrating keratoplasty with the placement of an amniotic membrane and a large-diameter contact lens.
The inferonasal cornea was also noted to be quite friable; therefore the corneal graft was slightly decentered inferonasally to incorporate this area. Follow-up for this patient is seen in Figure 3.

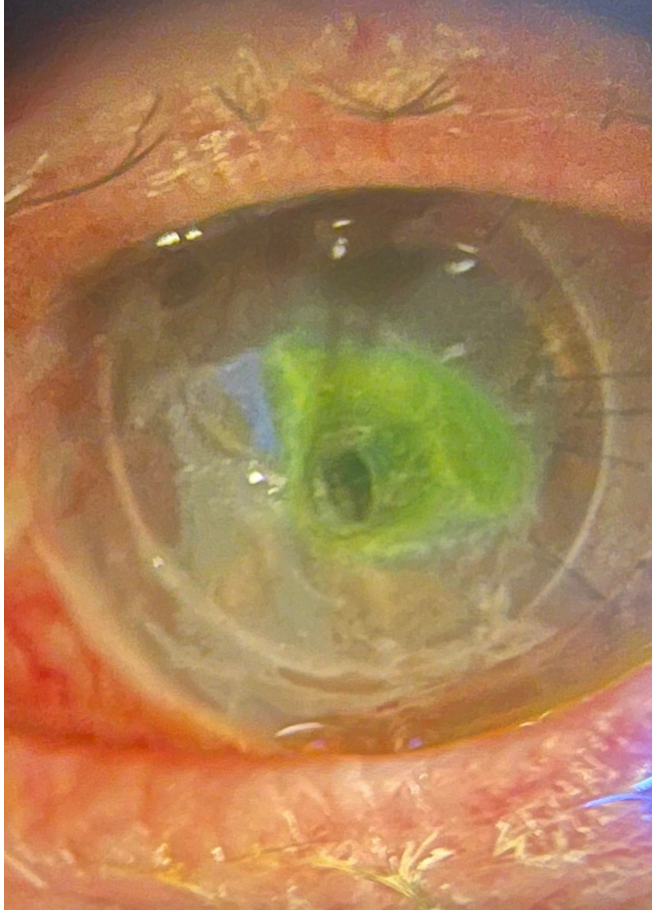
Figure 2: Courtesy of Mina Farahani, MD, MS, MS.
As seen in Figure 3, at post-operative week 1, the anterior chamber is formed, and iris details are visible underneath the new corneal transplant graft and amniotic membrane. Further follow-up images are seen in Figures 4 and 5.

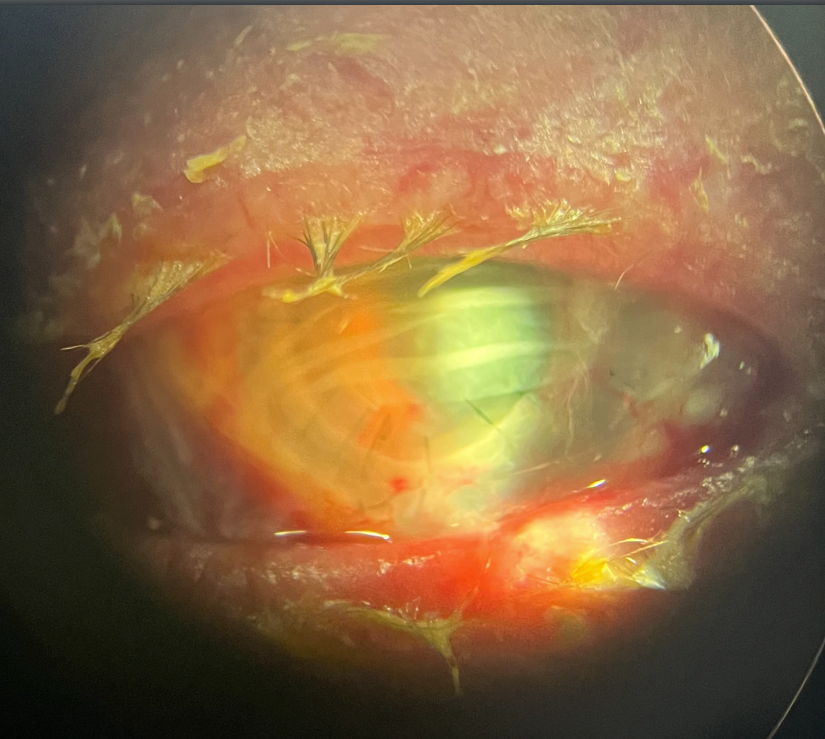
Figure 3: Courtesy of Mina Farahani, MD, MS, MS.
Figures 4 and 5 illustrate post-operative month 1; the graft remains clear and epithelialized.

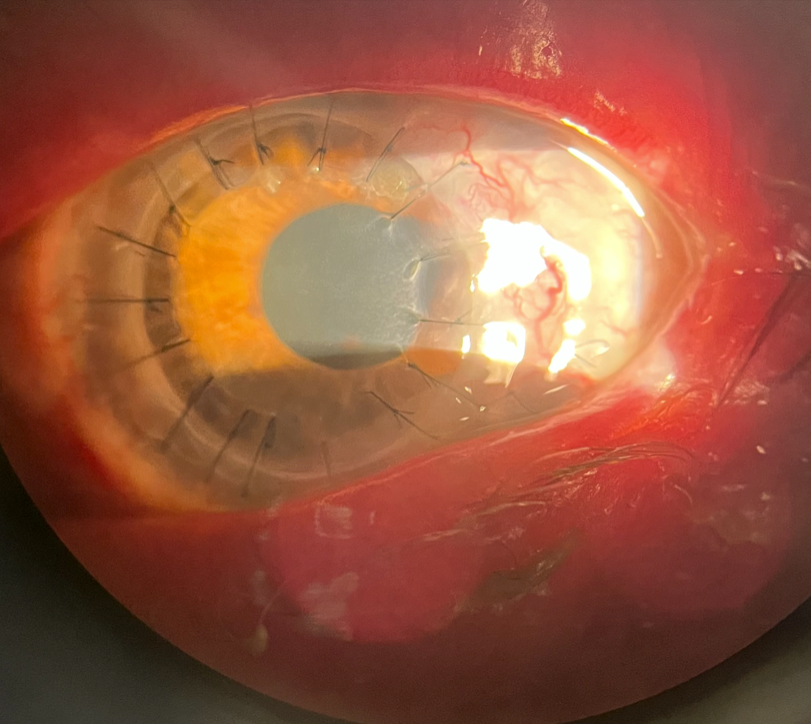
Figure 4: Courtesy of Mina Farahani, MD, MS, MS.

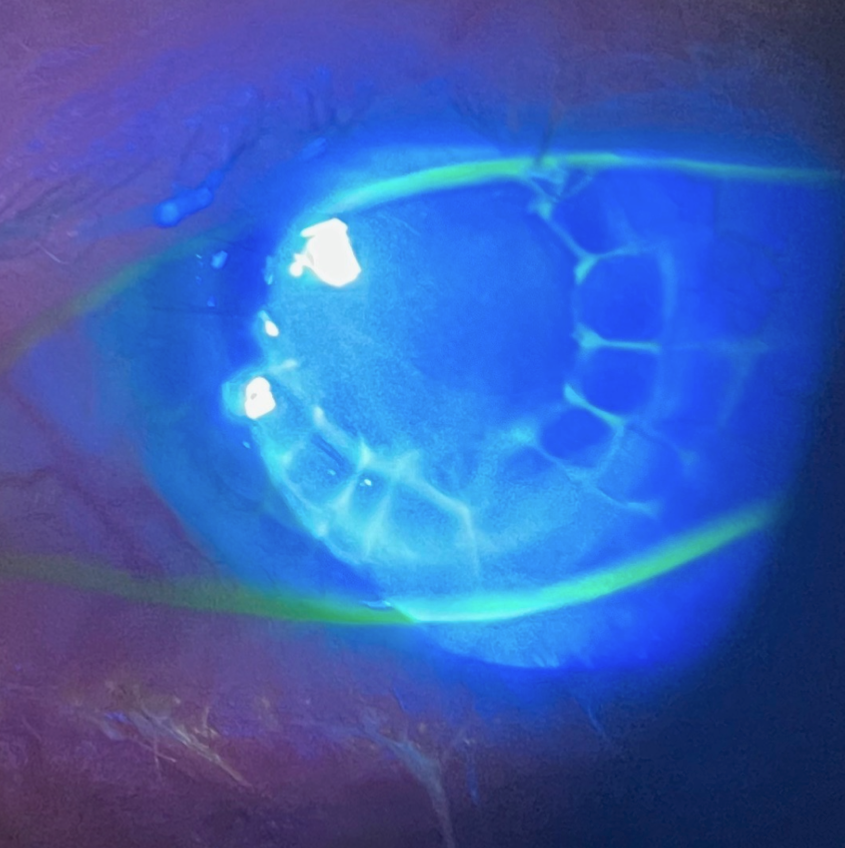
Figure 5: Courtesy of Mina Farahani, MD, MS, MS.
The patient continues to do well in post-operative month 4, with intraocular pressure and uveitis well controlled, with a clear, epithelialized corneal graft.
Conclusion
Stage 3 neurotrophic keratopathy is a vision and globe-threatening disease. It requires prompt evaluation and aggressive medical and surgical management with a corneal specialist in order to preserve vision and the integrity of the globe.
