




Advances in ophthalmic imaging have transformed the real-time assessment of a patient’s ocular health. Imaging studies are critical to make an informed diagnosis and monitor the pathophysiological progression of ocular diseases, particularly those with structural changes to the retina and choroid. This is especially important in diagnostic dilemmas when there are similarities in clinical presentation, yet treatment plans are disease-specific.
This article will discuss utilizing various imaging modalities to accurately differentiate between and guide management for various causes of posterior uveitis.
What is posterior uveitis?
Posterior uveitis is characterized by inflammation of the retina and/or the choroid that can be attributed to a wide range of infectious and non-infectious etiologies. It accounts for approximately 15 to 30% of uveitis cases globally, and the leading causes are idiopathic and infectious (toxoplasmic retinochoroiditis). In many cases, patients present with painless blurred vision.
Imaging techniques to visualize posterior uveitis
It is important to understand how each imaging modality differs in scanning range, resolution, sensitivity, and cost. Oftentimes, it will be important to utilize a multimodal approach to obtain a comprehensive view of any pathophysiological, structural, and functional changes.
Optical coherence tomography (OCT) is a noninvasive method to visualize and measure the thickness of the retinal layers, choroidal layers, and the optic nerve. There are two main OCT technologies currently in use: spectral-domain OCT (SD-OCT) and swept-source OCT (SS-OCT). While they primarily differ based on their light source and photodetection method, SS-OCT allows for faster scanning speed, higher resolution at greater scanning depths, and, consequently, enhanced visualization of the choroid.1
In addition, OCT-angiography (OCT-A) is another tool that combines the strengths of OCT and motion contrast imaging to visualize blood flow throughout different depths of the retina and choroid.2 Fundus autofluorescence (FAF) is another noninvasive tool that uses the naturally-fluorescent lipofuscin in retinal pigment epithelium (RPE) to primarily observe the microvasculature and pigmentation of the retina and optic nerve. FAF is especially beneficial for retinal pathologies that result in the accumulation of lipofuscin or damage to the RPE.
While all the previously discussed techniques are non-invasive, an important test called fluorescein angiography (FA) requires a fluorescein dye to be injected intravenously to assess for ischemia, vascular leakage, or neovascularization.
Imaging biomarkers for infectious posterior uveitis
The most common infectious causes of posterior uveitis are parasites like Toxoplasma gondii and DNA viruses, including herpes simplex virus (HSV) and varicella-zoster virus (VZV). These infections can lead to a necrotizing retinitis. Infectious posterior uveitis often presents unilaterally with an acute onset, and can progress to a retinal detachment.
In addition to laboratory testing, including polymerase chain reaction (PCR) testing for viruses and toxoplasmosis, imaging tools, including OCT, are helpful to refine the differential diagnosis and monitor the disease over time. Using OCT, one of the defining imaging biomarkers of viral retinitis is full-thickness retinal hyperreflectivity with no choroidal involvement. In contrast, the hallmark characteristic of toxoplasmosis on OCT is a significant thickening of the choroid paired with hyperreflective spots localized to the posterior hyaloid.3
Figure 1 highlights retinal vasculitis, defined as inflammation of the retinal vasculature, which is another common finding in both infectious and non-infectious causes of posterior uveitis.4

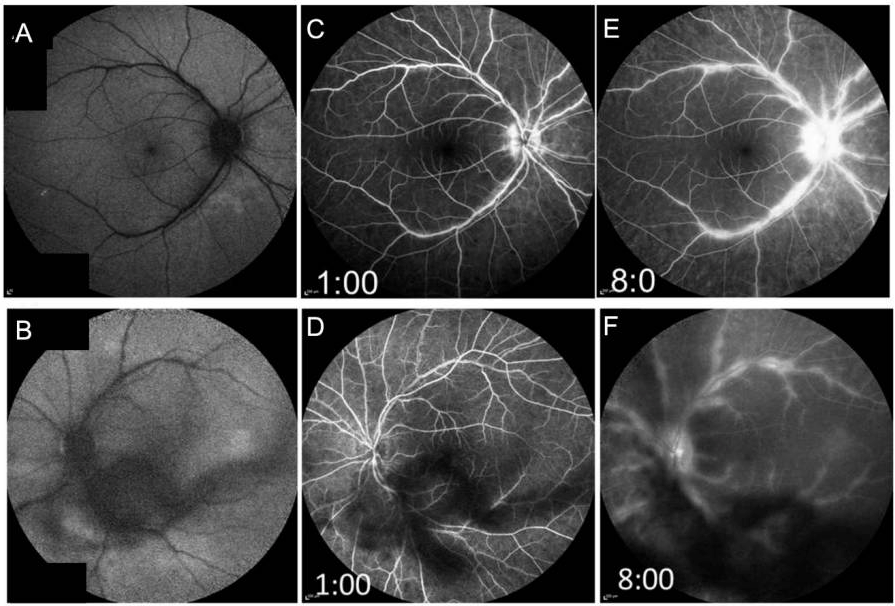
Figure 1: Courtesy of Agarwal et al.
It is important to identify the presence of retinal vasculitis because several non-infectious etiologies, such as Vogt-Koyanagi-Harada disease (VKH), do not typically present with vasculitis. Fluorescein angiography is the mainstay for evaluating and monitoring retinal vasculitis and its response to treatment, but there is growing research utilizing SD-OCT and OCT-A.
FA is the gold standard for retinal vasculitis because it can help to stage and visualize vascular and perivascular leakage, which will differ based on the disease etiology.5 For example, in toxoplasmosis, FA will show hyperfluorescent plaques but without any leakage.
In contrast, as shown in Figure 2, vascular leakage can be seen in cases of ocular syphilis, which also presents with diffuse hyperautofluorescence around the macula on FAF.6

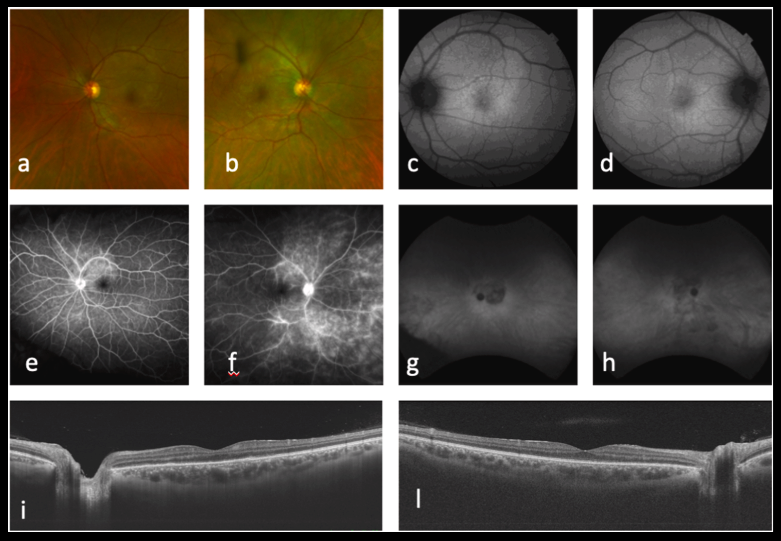
Figure 2: Courtesy of Ferro Desideri et al.
There is growing research that retinal vasculitis can also be indirectly evaluated with SD-OCT and OCT-A, which is especially useful in cases when evidence of retinal damage during vasculitis is limited on FA but still results in changes in retinal thickness. Likewise, OCT-A can be used to monitor hypoperfusion or nonperfusion in retinal vasculitis but is limited in its utility in identifying vascular leakage.7,8
Imaging biomarkers for non-infectious posterior uveitis
Non-infectious posterior uveitis can manifest from other systemic pathologies. Some of the leading identifiable etiologies are Behçet's disease and Vogt-Koyanagi-Harada disease (VKH). Importantly, cystoid macular edema (CME) may be found in up to 40% of posterior uveitis cases, and its presence may result in decreased vision.
Figure 3 features optical coherence tomography of the macula, demonstrating cystoid macular edema and subretinal fluid.

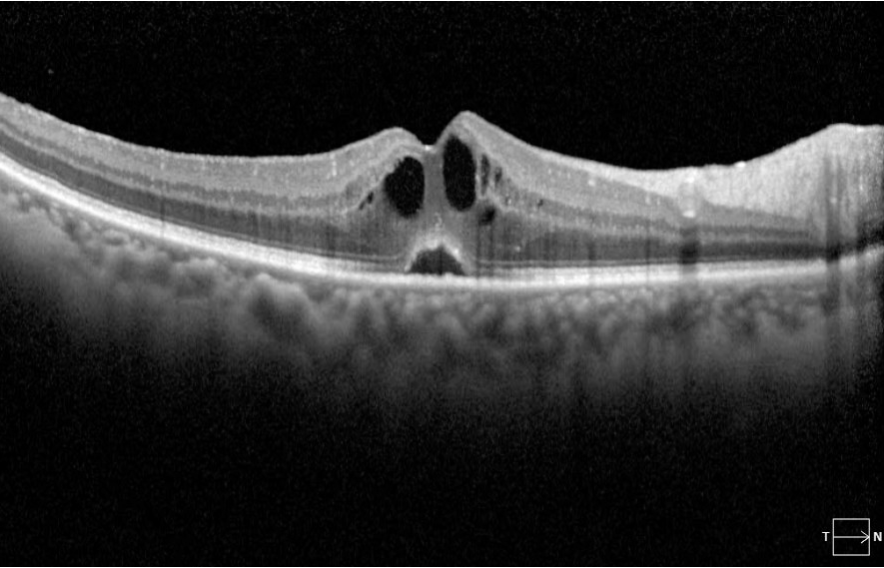
Figure 3: Courtesy of Edmund Tsui, MD.
Behçet's disease is an inflammatory disorder that primarily manifests as vasculitis in the eye. Patients may also present with genital and mouth ulcers. Because the blood vessels are often inflamed, FA is most commonly used to visualize the extensive vascular leakage from the capillaries, optic disc, and macula.
Cystoid macular edema is another complication of posterior uveitis, and as the name implies, CME causes a cyst-like buildup of fluid in the macula, diminishing central vision. OCT is beneficial in identifying macular edema, evident by a significantly greater central retinal thickness and macular volume compared to eyes without CME.9 As treatment is initiated, obtaining serial OCT scans can help monitor for CME resolution or recurrence over longer-term follow-up and may help guide treatment.
In addition to assessing retinal thickness, OCT is frequently used to monitor structural changes throughout the disease course. In particular, VKH is an autoimmune disorder that results in inflammation in the choroidal stroma and bilateral multifocal serous retinal detachment.
OCT imaging shows that VKH disease is frequently associated with bacillary detachment, in which the inner segment myoid remains attached to the RPE while the external limiting membrane becomes detached.10 Diagnosis of VKH can be further supported by fluorescein angiography, which shows scattered hyperfluorescent leakage in the RPE and pooling in the areas of subretinal fluid.
Figure 4 demonstrates a late-phase fluorescein angiogram in a patient with Vogt-Koyanagi-Harada disease, demonstrating pinpoint hyperfluorescence, pooling, and disc leakage.

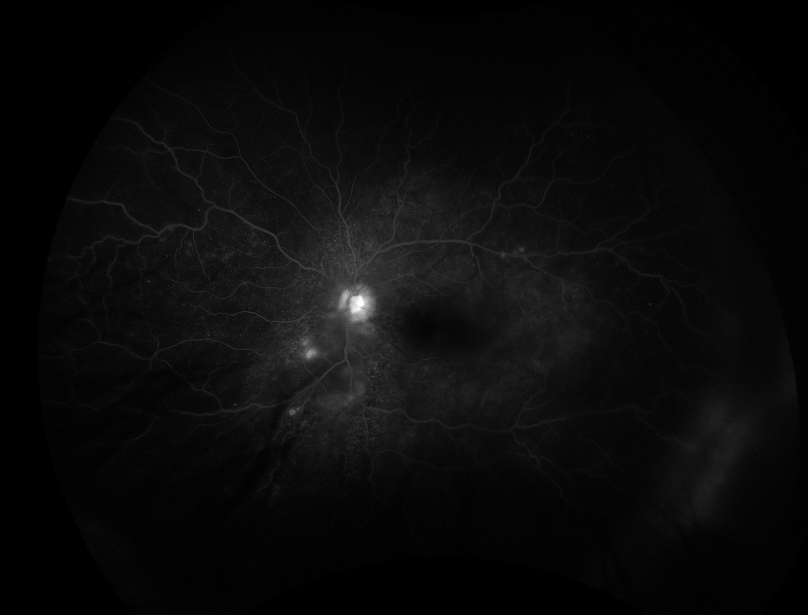
Figure 4: Courtesy of Edmund Tsui, MD.
Compared to other imaging modalities, FAF is better equipped to distinguish diseases that involve disruption to the RPE, such as multiple evanescent white dot syndrome (MEWDS) and serpiginous choroidopathy.
Compared to other imaging modalities, FAF is better equipped to distinguish diseases that involve disruption to the RPE, such as multiple evanescent white dot syndrome (MEWDS) and serpiginous choroidopathy.
As seen on clinical examination in Figure 5, using FAF, MEWDS is distinguished by hyperautofluorescent lesions spread throughout the retina that corresponds to “white dots.”11

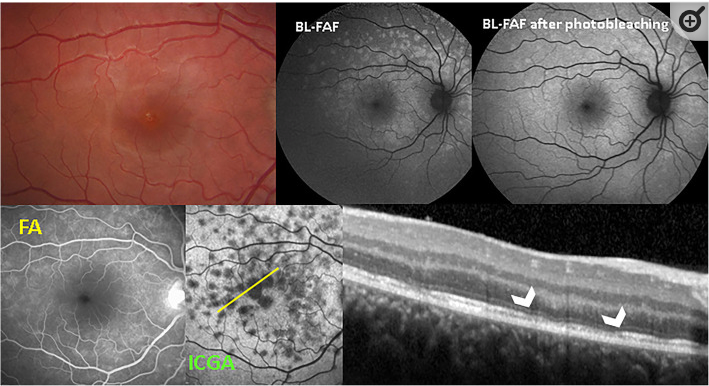
Figure 5: Courtesy of Agarwal et al.
These “white dots” are more frequently observed via FAF than FA or other clinical examination.12 Likewise, FAF is helpful in monitoring the progression of serpiginous choroidopathy because these rare yet acute, cases of RPE atrophy are characterized by hyperfluorescent edges around hyperautofluorescent lesions that become hypoautofluorescent as they become less active.13
The future of ophthalmic imaging techniques
With recent advances in imaging platforms and increasing research in imaging biomarkers in conditions such as posterior uveitis, there are opportunities for artificial intelligence (AI) to supplement clinical expertise potentially.14
Currently, there is research demonstrating the potential of AI to detect uveitis and grade the severity of vitreal inflammation primarily based on OCT and fundoscopy images. More diverse and representative datasets in terms of patient demographics and diagnoses are needed before AI can be used as a reliable and ethical tool in ophthalmic imaging.
