Optometrists provide nearly 80% of primary eyecare in the United States.1 We diagnose more than 300,000 cases of diabetes annually based on an eye exam alone.2
Yet, a significant portion of the country goes without crucial eyecare due to a lack of access. Many of these patients receive their medical care at
community health centers (CHCs), which are multi-disciplinary non-profit organizations; however, as of 2021, only 26% of health centers nationwide offered optometry services on-site.
3The value of offering eyecare services in CHCs
Community health centers can significantly increase access to affordable eyecare for these patients by providing in-house optometry services. For the CHC, this service can also bring in additional revenue as Medicaid encounters for optometry are billed at the same encounter rate as other CHC medical providers.
What is a CHC/federally qualified health center?
Federally-qualified health centers (FQHCs) are multi-disciplinary, non-profit healthcare organizations that provide affordable, cost-effective, high-quality primary and preventative care to underserved patient populations.3 FQHCs meet certain federal guidelines in terms of how they are structured and organized.
In addition to those health centers designated as FQHCs, there are many other variations, such as FQHC look-alikes, migrant farm worker clinics, rural health clinics, and those with tribal or
Indian Health Service affiliations. For the purposes of this article, we will refer to all of these clinic types as community health centers or CHCs.
Figure 1 highlights the average insurance breakdown for patients who go to community health centers.
Figure 1: Courtesy of National Association of Community Health Centers.
A review of the problem facing CHCs
Most CHCs offer medical, dental, and behavioral health services. Many also offer pharmacies and on-site labs. According to the
National Association of Community Health Centers, as of 2020, only 26% of all CHCs nationwide included full-time on-site eyecare services.
3 Socioeconomic status itself has been associated with higher rates of vision impairment and eye diseases.
1Many under- and uninsured patients rely on their community health centers for all of their healthcare needs, yet most CHCs are not currently providing eyecare services; therefore, the majority of these patients are going without this essential care. Lack of routine comprehensive eyecare leads to delayed treatment for ocular diseases.
Oftentimes these patients are only seen once permanent, irreversible vision loss has already taken place from conditions such as glaucoma or diabetic retinopathy.
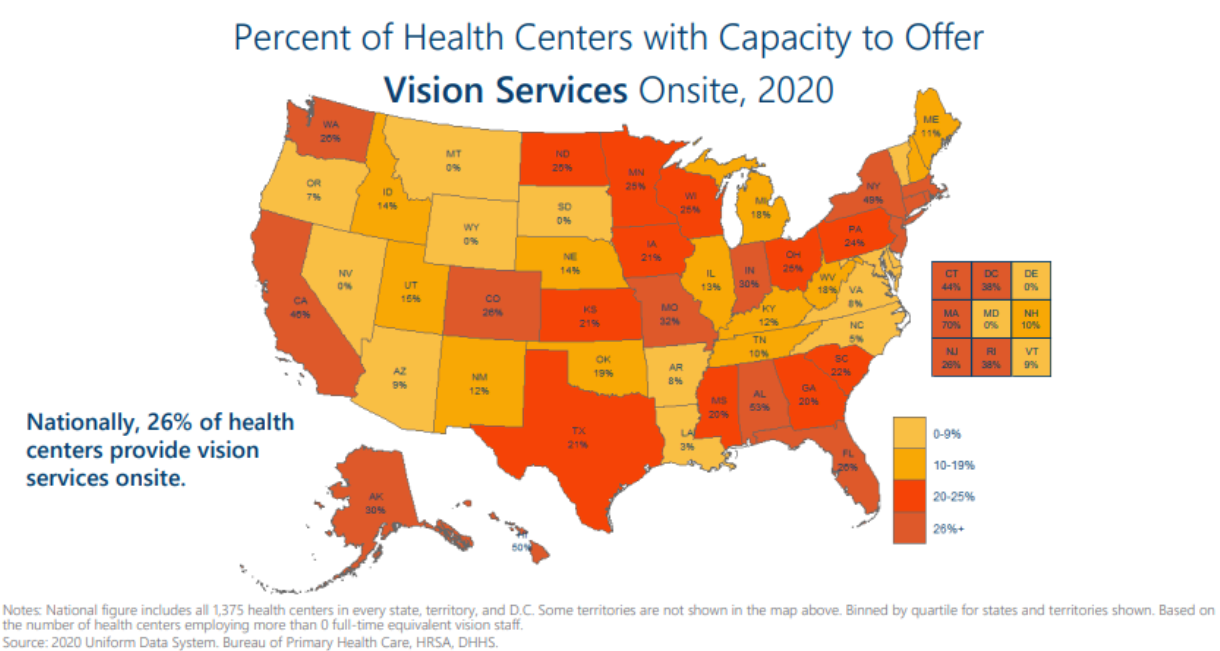
Figure 2 shows the percentage in each state of health centers employing one or more full-time equivalent vision staff.
Figure 2: Courtesy of National Association of Community Health Centers.
Expanding treatment offerings at CHCs with eyecare services
At the time of writing this article, many CHCs are showing great interest in adding optometry services due to the recognized benefits to their patients, a desire to improve quality improvement metrics such as diabetic retinal exams for GPRA and HEDIS, and in some cases having stimulus or grant money that may assist in the development of new programs.
Are you a CHC administrator? Still unsure whether optometry is right for you? Be sure to take the Vision Services Readiness Assessment created by the Association of Clinicians for the Underserved.
While other options for eyecare exist, such as referring patients outside the health center, virtual eye exams, or contracted mobile optometry, none of these solves the issue of consistent, ongoing care for chronic eye diseases and vision needs. This can only be met when CHCs offer on-site eyecare services through primary eyecare providers, namely, optometrists.
This article is designed to provide a step-by-step guide for the community health center and affiliated optometrists to follow when creating an on-site optometry department within a community health center.
Step 1: Assess the needs of the community.
Perform a needs assessment of your patient population.
This could include a survey of patients asking questions such as:
- When they last had an eye exam
- Whether they wear glasses
- Patient awareness of locations for affordably-priced glasses
- Patient awareness of where to go in case of an urgent eye problem other than the emergency room
This assessment can also look at the number of active CHC patients with certain medical conditions, such as
diabetes and
hypertension. It should also include an assessment of local optometrists and ophthalmologists and what insurances they accept.
Evaluating how many patients need eyecare services
You’ll also need to look at the total number of patients seen at your CHC. If your CHC sees between 18,000 to 20,000 medical encounters annually, then one full-time equivalent (FTE) optometrist (OD) can be sustained. If your health center is larger, you can expect to need more ODs based on this ratio of 1 OD/20,000 medical encounters.
An optometrist can be expected to see about 10% of the number of medical encounters annually. However, keep in mind that optometry will also bring in novel patients to the health center, especially in
rural settings, so if the number of medical encounters is lower than this, a full-time optometrist can still be viable.
If your health center is significantly smaller than this, say only between 6,000 to 10,000 medical encounters annually, it would be best to consider part-time optometry services. Consider contracting with a local OD to provide care at the health center 2 to 3 days/week. This may still pose a challenge as the CHC will still need to purchase the same amount of equipment as they would if full-time services were being provided.
Referring to or contracting a primary eyecare provider for your CHC
Referring patients outside to a local optometrist can prove difficult as most
private optometrists will not accept all Medicaid plans accepted by the CHC. Ensuring those referrals are completed is typically a large hurdle as nationwide, only about half of the referrals to specialists outside the health center get completed.
1Contracting a mobile optometry company to provide services with a set frequency can be another option for smaller health centers. Or, if you have multiple small, rural health center locations, consider purchasing a mobile unit and hiring an optometrist to travel to each site on a weekly basis.
If there are other smaller health centers in your area, consider purchasing the mobile unit together and contracting the optometrist jointly to cut down on costs and provide services to the collective patient population.
Knowing which direction makes the most sense for your health center will help you create a business plan and form a realistic idea of services that can be provided without overextending your budget.
Step 2: Get CHC Board approval and a Federal Scope Expansion.
Once you’ve assessed the needs of your CHC population, the health center’s Board of Directors will need to approve the new service. This may consist of the optometrist working with the CEO and CFO to create a business plan that is presented to the Board. The
American Optometric Association (AOA) created a business model that can help health centers assess the full cost of creating this new department.
4The Board may only require a more informal needs assessment and description of how this service can benefit the health center’s patients. For example, a breakdown of the number of patients with diabetes, hypertension, or high risk for those conditions and the benefits provided in caring for these patients specifically.
“Not to mention improvement in HEDIS and GPRA quality measures that can lead to financial benefits for the health center.”
Once the Board of Directors has approved the new department, the health center will need to apply for a
Federal Scope Expansion through the Health Resources and Services Administration (HRSA). This is because HRSA has defined both optometrists and ophthalmologists as “specialists” according to section 330 of the PHS Act, leaving eyecare services largely out of the picture for CHCs in the past even though optometrists provide primary medical eyecare.
Step 3: Hire an optometrist.
As soon as your health center is serious about adding optometry services, it would make sense to start looking for an optometrist, as this can sometimes be a lengthy process. Don’t feel you need to wait to make steps on getting started until you have hired someone, though.
You can contract with a local optometrist or consulting service to help better understand the needs of your health center and make your plan as above. Ask optometrists who already live and work in your community whether they would be interested in working for the health center.
Working at a health center for an optometrist provides a number of benefits and a work-life balance that is often not achieved in other work settings.
Consider posting your job position with optometry schools and residency programs as well as with
Eyes On Eyecare to have a broader reach. In addition to public service loan forgiveness that optometrists will qualify for working at the CHC, consider creating a loan repayment program as another part of the benefits package to entice newer graduates.
Once you find the optometrist who will work for you, hire them early, either full-time or on a consulting basis, prior to the start of patient care. During this time they will establish the ins and outs of the department as below.
Step 4: Acquire a space/find a location.
Is there currently space within the health center that is not being fully utilized that could be converted into an optometry department? Does the
community health center need to lease or purchase and renovate an off-site location?
Of course, there are a variety of ways this space can be designated. If you only have one exam room to devote to an optometrist but intend to do a larger health center renovation in the future, it could make sense to start small and grow as you’re able. If there is absolutely no space within the health center and purchasing or leasing additional space doesn’t make sense for your CHC at this time, consider purchasing and outfitting a mobile optometry unit.
This way, you have a full-service eye clinic and can see patients at your main location, satellite locations, within the community, or even at schools. You may consider leasing a storage unit that sits on-site somewhere, such as in the parking lot, and outfit it to become an eye clinic.
Tips for getting creative to make space for an eyecare provider
Ideally, you will want to create a space that can provide full-scope services to take the best care of your patients. For this reason, I would encourage you to view these smaller options only as temporary solutions or if your health center is very small in size and scope.
Options for health centers with limited space:
- Reorganize the current space to provide a single exam lane for the service.
- Share a medical exam room part-time based on need.
- Rent/lease space in an external location.
- Mobile unit or convert storage unit.
- Future health center renovations/expansions.
Figure 3 features the exterior of a leased storage unit in the parking lot of a satellite clinic at Dr. White’s former health center.
Figure 3: Courtesy of Kristin White, OD.
To provide a full-scope optometry department, you’ll need the following:
- One to two exam rooms (ideally 10’ x 12’ or larger) for one provider. Two exam rooms for one provider will increase efficiency.
- Pre-testing room = exam room of the same size or larger to screen patients prior to seeing the provider.
- A waiting area/lobby.
- A receptionist desk.
- Technician workstation (can be inside the pre-testing room).
- Optical (see considerations below).
Figure 4 highlights the interior of the above-photographed storage unit that was converted into an eye clinic lane/exam room.
Figure 4: Courtesy of Kristin White, OD.
Step 5: Purchase equipment.
Providing comprehensive optometry services means managing a significant amount of ocular disease. In addition to an exam room or “lane” of optometry equipment, the CHC will be able to provide the best care if it also has pre-testing equipment, as well as tools for diagnosing and managing ocular disease, such as diabetic retinopathy, glaucoma, and
macular degeneration. This is essential given the high number of patients with these conditions or co-morbidities that lead to them.
You can find a full equipment list for various models of clinical care
here. Reach out to various ophthalmic equipment distributors for the best pricing. There are both local and national distributors who can provide this service. One source should be able to provide the bulk of the equipment. Be sure to have the equipment ordered at least 1 to 2 months prior to the anticipated patient care start date in case there are any equipment delays.
Considerations for acquiring an optical coherence tomographer
The most costly piece of equipment that may be debated is whether or when to purchase an
optical coherence tomography (OCT) device. This piece of equipment provides a scan of the retina and is, at this point in time, essential for diagnosing and properly managing ocular disease.
Given the high amount of ocular disease that will be seen in the optometry department of a CHC, too many patients would need to be referred out for this test which would run into the same logistical headaches that you’re likely running into now by not offering optometry services at all.
Therefore, I would say an OCT is essential. If unable to purchase on day one due to cost or space restrictions, plan for it in the future once the department becomes profitable.
The exceptions to this are the following:
- You will be seeing primarily pediatric patients. Given that children have a significantly lower amount of ocular disease compared to adults if your main patient base will be pediatric, an OCT is not needed on day 1 of patient care. Once your clinic opens up to adults more regularly, you should strongly consider also bringing in an OCT.
- You are only providing basic in-house services (one exam room, no pre-testing room, minimal staff) to start until a renovation or a larger amount of space can be dedicated to the optometry service. In this case, you will not have the space or staff to run these additional tests and can hold off on adding the OCT until your clinical space is better equipped for it.
Figure 5 shows an exam lane (doctor’s exam room) at Dr. White’s former health center with an exam chair, slit lamp, and phoropter and stand. Not shown in the image is a digital visual acuity chart on the wall opposite the exam chair.
Figure 5: Courtesy of Kristin White, OD.
Step 6: Create the optical.
As with all aspects of creating this department, there is a large variation in how you can provide glasses for your patients. It is strongly encouraged to provide glasses on-site. To the patients, this is the most important part of the exam and often their driving factor for coming to get their eyes checked in the first place. Regardless of the excellent medical eyecare provided during their exam, if the patients cannot leave with the glasses they need, they will often feel the visit to be a waste and may be less likely to return in the future.
“That being said, there are a lot of considerations as to what providing glasses for your patients can look like.”
First and foremost, given that many of your patients will be on
Medicaid, the optometrist will need to determine exam and glasses coverage for each Medicaid plan that the health center accepts and how those glasses are provided. Given the increase in managed Medicaid and Medicare plans, each plan can sometimes be run very differently.
You will need to contact the plans to determine whether they will provide you with a selection of frames or whether the CHC will purchase frames to be provided to the patients. At a minimum, I would recommend starting off by providing glasses for Medicaid patients.
Providing low-cost glasses for patients
After providing glasses for Medicaid patients, it’s beneficial for a CHC to provide low-cost self-pay options as many patients either may not have any insurance or may not be covered for glasses under their insurance. Children with Medicaid are typically covered for glasses under the Affordable Care Act (ACA); however, adult coverage varies by state and plan.
Find a local lab that will give you a good price to make the prescription lenses and pass along that discount to your patients. Low-cost frames can be purchased through
Modern Optical or
Smilen Eyewear. Because you will already be offering a low-cost, discounted package rate for glasses, these glasses would not be eligible for a further sliding fee discount.
Providing free or sponsored glasses for patients
Another consideration for those who cannot afford even your low-cost glasses, is to offer free glasses through select charitable programs for those in need. Some programs offering free glasses include
Changing Life Through Lenses and
New Eyes. Additionally, local Lions Clubs will also sometimes sponsor a patient in need of glasses. Use the sliding fee application to determine who is eligible for these programs (often those who qualify for the maximum discount).
Here are some questions to ask yourself when setting up the optical:
- Who is the target optical audience: Medicaid only? Managed Medicaid plans may each have their own method of providing glasses.
- Will you also be seeing managed Medicare patients? These patients often have vision plans that cover glasses. Do you want to have options for those patients as well?
- What about inexpensive self-pay options for those without insurance? If your self-pay option is already a significantly discounted or “package” rate, you will not apply your sliding fee scale on top of this.
- What role will charitable glasses programs provide for your patients?
- Will you offer glasses for patients with private insurance? Are there other local optometrists where those with private insurance are more likely to go to get higher-end/designer frames? Or is your CHC more rural in a location in which case all patients, regardless of insurance, may be seeking services at your CHC?
The answers to these questions will depend on your CHC’s demographic. It is more than reasonable to start the optical off simply by providing charitable glasses, Medicaid glasses, and/or inexpensive self-pay options working with a local optical lab, and then expanding from there once you have a better idea of your patients’ needs.
Medicaid optical reimbursement
Depending on the individual Medicaid plan and how the glasses are made, whether the plan provides a lab that cuts the prescription lenses and inserts them into the frames or whether your CHC is being charged for this service by a private lab will determine what you can bill for in the optical.
The options include billing for the frame, lenses, and a dispensing fee depending on what your CHC was charged for. While you may not make a significant profit in the optical, you should be turning some profit at least by collecting a dispensing fee.
Examples of how to showcase optical offerings in CHCs
Medicaid-only insurance coverage
You may have ~50 frames (depending on state requirements), some Medicaid plans will provide frames their patients are required to choose from. An optical does not have to be complicated or take up a lot of space to meet the needs of your patients.
Figure 6 features a simple optical that can be moved between exam rooms at a Mississippi Health Center. These trays can also be stored in a cabinet or closet, depending on space.
Figure 6: Courtesy of Kristin White, OD.
Full-scope optical insurance coverage
Offers ~350 to 450 frames in a variety of styles and price points.
Figure 7 depicts a larger optical displaying ~450 frames in a small, converted storage closet. This provides glasses ranging from very inexpensive to high-end designer frames.
Figure 7: Courtesy of Kristin White, OD.
Step 7: Assemble a staff.
Staffing, like everything else when developing a new department, depends on the scope of care you intend to provide. If you only have one exam room available, then you will only have space for the optometrist in that room. A receptionist and billing specialist will likely be shared with other departments depending on the location of the exam room.
However, if you are going to provide more full-scope care, offering pre-testing, diagnostic imaging (OCT/fundus photography), contact lenses and an optical, then you will need more staff to support your optometrist. Support staff would need to include at least one receptionist devoted to optometry, one optometric/ophthalmic technician, and one
optical assistant/optician.
Hiring opticians and ophthalmic technicians
Depending on your state, opticianry can be a licensed profession. If you are able to secure a licensed optician, all the better, as they will be able to handle measuring patients for glasses and fixing and fitting complicated glasses prescriptions. An optical assistant, on the other hand, would be a staff member who is trained on the job to handle these tasks.
An
optometric or ophthalmic technician can be a certified position (not licensed); however, certification is not required, and most technicians have not been certified and receive all training on the job. A billing specialist will likely be shared with other departments but will need training on optometry-specific billing.
Step 8: Add up and address start-up costs.
As in creating any new department, there will be a start-up cost for these services. Below is a chart of basic equipment costs. The
AOA Business Model for CHC Optometry will provide a more thorough cost analysis. Your CFO can input your own health center’s exam reimbursement and any potential renovation costs.
Keep in mind optometry services will be reimbursed at the same encounter rate as all other medical services in your health center from Medicaid, meaning this service can be profitable for your health center.
Table 1 breaks down basic start-up costs associated with introducing eyecare services to a community health center.
| Factor | Estimated Cost |
|---|
| Basic exam room and pre-testing equipment | $50,000 |
| Advanced diagnostic imaging | $20,000 to $70,000 (optional day one) |
| Optical dispensary | $500 to $25,000 |
| Optometrist salary with benefits (FTE), may vary based on location | $160,000 |
| TOTAL START-UP COST | $210,000 to $305,000 |
Table 1: Courtesy of Kristin White, OD.
Grants can help offset start-up costs:
- ACU Eye Health and Vision Care Grant (applications accepted annually)
- American Rescue Plan Funds
- Health Resources and Services Administration (HRSA) Service Expansion Grants
- Private donors
- Other grant opportunities:
- Local Lions Club
- National Eye Institute (NEI) may have grants qualify for
- Contact your Congressperson for any local grant options that may exist
Step 9: Gain insurance credentialing.
Plan on the optometry department being credentialed with all the same medical insurances the rest of the health center already accepts to facilitate interdepartmental care. Keep in mind that in addition to the medical insurance plans, the optometrist will also need to be credentialed with corresponding vision plans.
“More and more, Medicaid and Medicare are moving to managed care plans.”
For optometry, this means that there is a portion of the plan managed by a medical insurance company and a portion of the plan that is managed by a vision plan carrier. Whether you will try to be credentialed with private vision insurance plans will depend on location and patient base, as discussed in the optical section above. Keep in mind some private vision plans will not credential health centers.
It can take several months for your optometrist to get credentialed on all of the necessary panels, so it is recommended to start this process at least 3 months prior to your anticipated start date of patient care.
Step 10: Choose the electronic health records system.
For maximum efficiency in integrating the optometry department with the rest of the health center, optometry should plan to use the same electronic health record (EHR) system already used in the health center. The one exception to this is in regard to optical management software (
glasses sales and inventory management).
Sometimes this software needs to be purchased separately. Look into this software thoroughly before deciding whether it makes sense to go with the brand that integrates with your EHR or whether a more functional system may exist despite being a separate program.
Step 11: Determine a fee schedule.
As in a private setting, it is recommended to set your fee schedule for exams, special testing, and procedures to be at least what Medicare will reimburse for your area. You can determine the Center for Medicare and Medicaid Services (CMS) reimbursement based on the current procedural terminology (CPT) code for your area
here.
The optometrist and CFO or COO should work together on this. Low-income patients without insurance should also be able to apply for a sliding fee scale for their exam services. Consider offering a sliding fee package rate for special testing, for example, a “glaucoma testing package.”
Conclusion
Optometrists provide vital primary eyecare services to a significant portion of the population. Community health centers are lacking in providing these services to their patients who have a high percentage of
systemic disease which puts them at risk for permanent vision loss.
By providing in-house comprehensive eyecare services, community health centers can enhance the quality of life of their patients, increase their revenue, and improve GPRA and HEDIS measures.
Resources for those involved or interested in CHCs
Are you a health center administrator or Board Member? An optometrist with a passion for serving in your community?
Here are some resources for connecting and creating on-site eyecare services within a CHC:
- Report by the AOA and Association of Clinicians for the Underserved: "Integrating Eye Health and Vision Care for Underserved Populations into Primary Care Settings," found here.
- National Institutes of Health: List of programs that offer free eye exams, glasses, and surgeries for those who qualify.
- Eyes on Access: A three-part webinar series hosted by the Association of Clinicians for the Underserved, the National Association of Community Health Centers, and Prevent Blindness America.
- Part I: "Introduction to Comprehensive Vision Services in Health Centers"
- Part II: "Steps for Integrating Comprehensive Eye Health and Vision Services into Health Centers"
- Part III: "We’ve Decided to Offer Vision Services in Our Health Center, Now What?"
- Association of Clinicians for the Underserved: Vision Services Readiness Assessment.
- Association of Clinicians for the Underserved: Optometry Equipment Budget.