




WHAT YOU'LL LEARN
Understand the importance of collaborative care in cataract surgery
Learn which information is most important for a surgeon to know
Practice methods for explaining cataract surgery and IOL options to patients
Introduction
Why care about collaborative care?
As optometrists, it is imperative to cultivate symbiotic relationships with local cataract surgeons in order to provide our patients with the best possible outcomes. It is also important for us to keep up with the newest technology and be educated on products, procedures and protocols in order to promote the best option for each individual patient. The optometrist and ophthalmologist each play an important role in the successful evaluation and management of cataract surgery patients. When the care team is able to work together in a collaborative way that is really when we are able to take care to the next level. In order to explore this topic further, we have interviewed three doctors well-versed in collaborative cataract surgical care.
At the Schwartz Laser Eye Center in Phoenix, AZ, Jay L. Schwartz, DO and Marc Bloomenstein, OD, FAAO practice collaborative eyecare treating LASIK, cataract, and other ophthalmic patients. Jeffrey Martin, MD is a managing partner at SightMD in New York state and assistant clinical professor of ophthalmology at SUNY Stony Brook. Drs. Schwartz and Martin are both board-certified ophthalmologists specializing in LASIK and cataract surgery.
*Drs. Schwartz, Martin, and Bloomenstein are paid consultants of Johnson & Johnson Surgical Vision Inc.
Collaborative care and cataract surgery
What is collaborative care in cataract surgery?
Collaborative cataract care refers to the sharing of a patient's care between an optometrist and ophthalmologist, particularly when it comes to cataract patients. Of course, part of this collaborative effort is for the optometrist to identify those patients who would potentially benefit from cataract surgery and partner with a surgeon for referral—but it should not end there! Dr. Martin has had a deep-rooted sense of collaboration between optometry and ophthalmology within his practice since his father, founder of SightMD, had established this type of care from the beginning. Dr. Martin views the optometrist as a primary eye care provider and makes an analogy of cataract surgery to heart surgery; the cardiac surgeon does not then become the primary doctor, the primary care physician remains so after the procedure is complete. Dr. Martin has found the in-house optometrists serve as a bridge to outside optometrists. This has helped him introduce a more successful relationship between like-minded optometrists with the ophthalmologists in the practice. Dr. Schwartz works alongside three optometrists at his practice; he also feels having experience working with in-house optometrists creates a continuum type of experience that is beneficial for the patient.
Three requirements for collaborative care
According to Dr. Martin there are three main points of collaborating in the care of cataract patients. The first being the medical care portion. The second is the compliance and legal portion. The plan for collaborative care needs to be clearly explained to the patient- including how the care will be shared and the fee schedule. If the patient does not understand their own responsibilities related to follow up, this can lead to poor compliance, poor outcomes and potential issues for the involved doctors. The third, and most important, component is that it is the patient’s choice to receive care this way. Not all collaborative care setups are the same and not 100% of patients are going to want it; if the patient does not feel comfortable then it’s not pursued. If it is, there needs to be complete transparency of the plan and each party's responsibilities.
Finding the right collaborative care partner
It is important to find a surgeon who you feel comfortable working with and who you share the same mindset with. Dr. Bloomenstein recommends finding a practice that exhibits the same attitude and mentality as your practice and a surgeon who describes procedures and protocol in a similar manner. He also recommends visiting the surgeon’s office to observe the workflow and process. This allows you to explain it to your patient accurately and ultimately make them more comfortable at the evaluation. If you are comfortable with and confident in the referral the patient will be too!
Once you make the referral, following up with pamphlets or brochures about the technology or the surgeon’s practice is helpful. Dr. Bloomenstein feels this really bolsters these recommendations. It gives the patient some information to consider at home, discuss with their family and have some awareness and understanding of before their consultation.
Lens options
How to discuss lens options with patients
Dr. Bloomenstein enjoys talking about the lens options with patients and getting them excited about the opportunities available. Asking patients questions about their lifestyles and preferences is key: what do they enjoy doing? What is important to them? What is their occupation? Would they be satisfied with some glare at night to have good vision at all ranges? Is night vision more important than being glasses-free at near vision tasks? Do they frequently drive at night?
Additionally, Dr. Bloomenstein notes that it is important to define what “reading” means for the patient—do they read paperback books held close to their face, or a tablet placed on their lap? Do they spend more time doing computer work than reading, and do they work on a laptop or a desktop? The goal is to find a way to personalize the patient’s vision, since individuals do not work the same way. While there may be certain limitations and optometrists should be wary of making specific lens recommendations before the surgeon’s evaluation, optometrists today are in a position to offer more patients reduced spectacle wear post-surgery.
Dr. Martin recommends that optometrists familiarize themselves with the lens options and procedure choices to give an introduction to what will be discussed in more detail at the cataract evaluation. It is beneficial to the ophthalmologist when the optometrist has been working with the patient for some time and has an idea of the patient’s desires, personality, or hobbies as well as knowledge of their ocular history. Dr. Martin feels that an optometrist making a “strong recommendation” based on these factors assists his decision-making process. Similarly, Dr. Schwartz appreciates if the optometrist introduces the options and concepts; however, he warns that setting expectations that are too specific can lead to patient disappointment and distrust.

Visit https://www.jnjvisionpro.com/Eyhance to learn more.
How optometrists can make a recommendation
Optometrists can make a strong recommendation by getting to know the patient and collecting information that would be beneficial in the decision making process. For example, hobbies, occupation, time spent reading versus night driving, anxious or laid back personality. Having the patient demonstrate where they habitually read and keep their computer is helpful as well.
There are several important components of patient education for the optometrist to cover. First, making sure the patient understands their refractive condition (especially presbyopia and astigmatism) and the basics about cataracts. For patients who might not know that they have astigmatism, it’s especially important to explain why that might be the case. Astigmatism can occur on the cornea or the lens in such a way that nullifies the magnitude of the astigmatism. However, when discussing cataract surgery, it’s crucial to define the corneal astigmatism to patients since we are removing the lenticular astigmatism. In cases like this, corneal topography can be used to show patients their corneal astigmatism and what they can expect postoperatively.
This should be followed up by a discussion of the options relevant to their refractive status, such as a toric lens for astigmatism, laser treatments to nullify some of the corneal astigmatism, or a combination of both. This introduces the concepts and terms the surgeon will later bring up. This is an opportunity for the optometrist to set expectations at an appropriate level so there is still room for the surgeon to maneuver in making an appropriate lens choice without disappointing the patient.
The tools we have in our toolbox include monofocal IOLs, accommodating IOLs, multifocal IOLs, and extended depth of focus IOLs. All of these options now have toric versions available. Current research suggests that while ⅓ of patients have greater than 1D of cylinder, only about 25% are receiving toric IOLs.5 This is an opportunity for optometrists to really educate patients since residual astigmatism can hinder success with IOLs in general. Presenting the options for astigmatic correction, LRI or arcuate incision, toric IOLs, or postoperative glasses or contacts, lays the foundation for incorporating the proper refractive correction into the surgical plan.
Lens choice and surgical options
How ophthalmologists identify the “right” lens
Dr. Schwartz makes his intraocular lens choices based on a patient's desires and ocular history. Patients with greater degrees of astigmatism and regular astigmatism are candidates for toric IOLs, which are specially designed to correct astigmatism through different powers in different meridians of the intraocular lens. During surgery, the lens is aligned in the eye so that the lens is oriented appropriately.
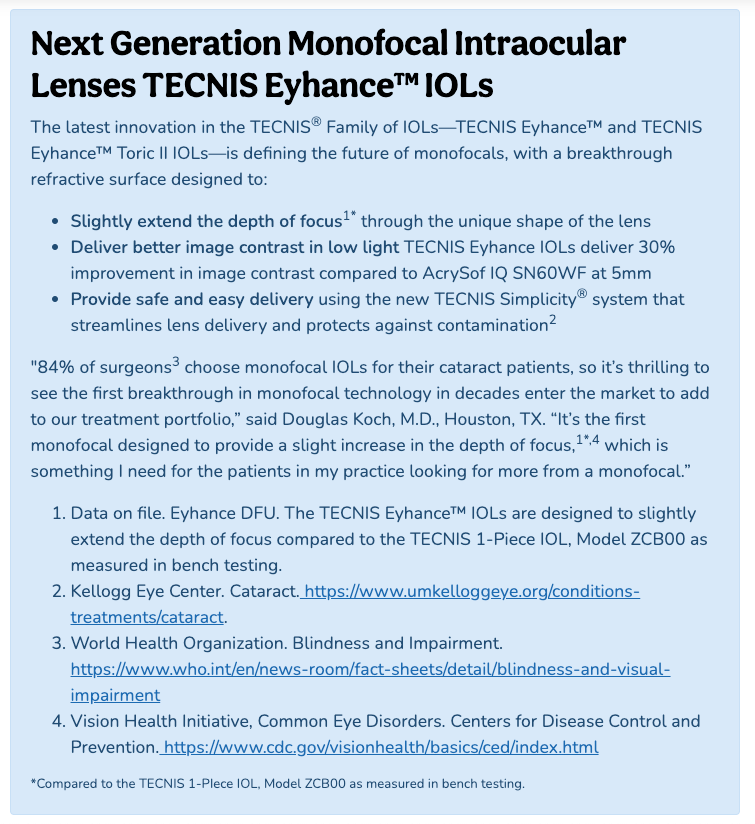
As an additional example, a patient with macular degeneration may not be the best candidate for a certain multifocal lens, while a patient with an immaculate macula and an interest in maintaining reading vision might find a multifocal or extended depth of focus (EDOF) to be a great option.

While a multifocal IOL works by splitting light between two distinct focal points, an EDOF lens, TECNIS Symfony™, distributes light across a range of distances. This is what creates the extended depth of focus with a continuous range of clear vision. If an EDOF lens is being considered, it's essential to have a discussion about neuroadaptation. With this type of lens the brain needs some time to acclimate to the optics. By explaining the technology to the patient in advance we are setting up for better success postoperatively.


* TECNIS Multifocal IOLs provide distance and near vision (ZLB00 and ZMB00) or distance and intermediate vision (ZKB00). In combination, the lenses can provide a full range of vision.
Understanding laser cataract surgery
According to its proponents, femtosecond laser technology is a customized treatment plan that is more precise, and more gentle than the manual procedure. In FSL assisted cataract surgery (FLACS), the laser does the work of a surgical blade, making incisions in the tissue on either side of the cornea to access the cataract. In FLACS, the femtosecond laser breaks the lens up before entering the eye for easier phacoemulsification, which breaks up the cataract and vacuums the pieces out of the eye. Because it requires less energy for lens fracturing, FLACS causes less inflammation and allows for faster recovery.6
Overall, laser cataract surgery offers a smoother procedure and tends to give patients more confidence in the surgical outcome. When discussing the difference between laser and traditional cataract surgery, Dr. Martin will explain the options and the precision of laser cataract surgery, and will discuss the costs associated with astigmatic correction of laser cataract surgery. According to Dr. Martin, most cataract cases benefit from laser cataract surgery, like the CATALYS® Precision Laser System, and really the only time it would not be as beneficial is in a patient with historical corneal pathology, where the prognosis is guarded to begin with.7,8
The CATALYS® Precision Laser System
When Dr. Martin approaches the subject of laser cataract surgery versus manual, he explains the aforenoted benefits but lets the patient know it's “okay” to still choose the manual route. For some patients, the financial burden is just not doable and he lets them know that manual cataract surgery is still a safe and effective procedure. As he puts it for his patients “laser didn’t make a bad procedure good, it made a good procedure better.”7
Videos like this one are excellent tools for patient education, particularly if they can be made available to patients to view at their leisure.
Preoperative and postoperative care
The role of the optometrist
In collaborative care, an optometrist’s role extends beyond the referral to cataract surgery. As mentioned earlier, the referring optometrist’s knowledge of their patient’s history and needs is crucial information to relay to their surgeon; additionally, the optometrist plays a crucial role in postoperative care.
From preoperative
The surgeon’s preoperative evaluation usually involves a thorough ocular health exam on top of the refractive portion and lens selection. Dr. Schwartz does rely on findings provided by the referring optometrist; however, he still repeats most testing to make himself more comfortable with the case. Dr. Martin also performs a thorough ocular health exam on the patient, focusing on any areas the optometrist has pinpointed on the referral form. After the thorough evaluation, a conversation of risks, benefits and options takes place.
To postoperative
Dr. Martin will continue to follow the patient until he feels like it’s safe to transfer care to the optometrist. The common postoperative follow-up schedule is one day, one week, one month, three months, six months, and one year. Dr. Schwartz generally likes to see the one-day and one-week postoperative patients himself. In particular to check their intraocular pressure, lens position, and level of pain. The vision can fluctuate since there is still swelling, especially one day after surgery. One-month and three-month postoperative follow-ups are generally performed by the managing optometrist. At this time, the majority of healing has occurred and if there is any residual inflammation it can be treated and managed by the optometrist (with surgeon consultation as needed). If post-surgical cystoid macular edema is present or the refractive error needs major adjusting, then the optometrist will send the patient back to the surgeon. Dr. Bloomenstein suggests discussing with the surgeon how and when they plan to make any adjustments; for example, do they like to have the patient acclimate for 30 days then re-visit? It may also be helpful to know at which point your surgeon prefers to do YAG-Capsulotomy if and when the time comes.
Treating OSD before surgery
It is especially important for both the optometrist and ophthalmologist to do a thorough preoperative exam for premium IOL cases to help avoid unexpected outcomes. Any treatable ocular health issues need to be addressed before going forward in order to increase the success rate. Ocular surface disease, including meibomian gland dysfunction, is a big one. This will need to be well-controlled before surgery in order to obtain accurate readings for topography, keratometry etc. This can be done by creating a regimen of lubrication, lid hygiene, and considering TearScience® LipiFlow® treatment if needed.
Additionally, an intact corneal surface aids in the healing process. Dr. Martin notes that this is a point of collaborative care like anything else. He will confer with the referring optometrist about how they would like to handle the treatment plan. Dr. Bloomenstein makes sure ocular surface disease is treated before proceeding and explains to patients that we can make the best lenses and do the safest surgery but if the ocular surface isn’t clear, it is “muddling” all the other hard work. A healthy ocular surface allows ophthalmologists to identify and utilize the best lens for the patient’s desired outcome.
Even simply identifying OSD prior to surgery can make the surgical experience much smoother for both patient and surgeon—not to mention bolstering trust in the patient-doctor relationships, including between that of patient and optometrist.
Unhappy surgical patients
What causes unhappy surgical patients?
The biggie—unrealistic expectations! The surgeon can fully and thoroughly explain the risks, benefits and limitations of every technology and sometimes that still just isn’t enough. This can be a combination of the patient not listening or simply being overwhelmed by the amount of information.
One step Dr. Schwartz takes regarding this, that optometrists can do as well, is to take detailed notes of what was discussed during the consultation to reference later on in a “remember when we talked about? I jotted it down in my notes . . . ” fashion. One particular example he mentioned was when utilizing a premium lens in a patient who had an essentially perfect surgical and visual outcome. This particular patient still didn’t feel “quite right” despite having been educated on halos at night and neuroadaptation after the procedure (up to a year after surgery). Dr. Schwartz took time to re-educate and have a discussion with the patient, who then decided to wait it out a bit longer to see how he adapts.

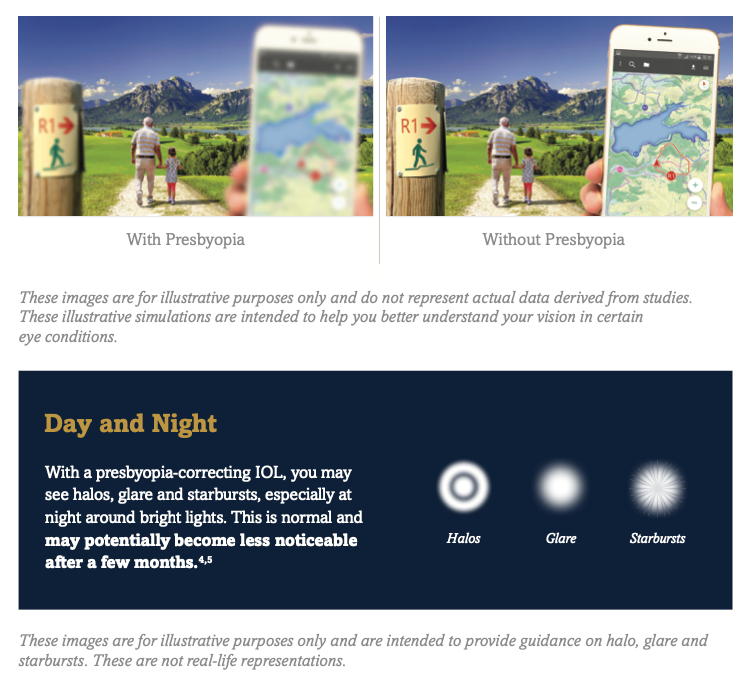
Providing patient education materials that illustrate possible visual symptoms helps prepare them for their recovery and neuroadaptation following surgery.6,7
Medically speaking, patients can also have valid reasons to be unhappy including capsular opacification, residual astigmatism, OSD, cystoid macular edema or poor IOL centration. Any of which can be detected in a thorough follow up exam and addressed accordingly.
Problem solving
If a postoperative patient is having a concern, the ophthalmologist will take time to discuss best solutions for the patient. This might mean a lens exchange or LASIK or PRK for adjustments or monovision correction. Dr. Schwartz feels that most of the time, once you sit, talk to the patient and explain things that can solve most of the problems! Dr. Martin will often do LASIK free of charge if the patient is unhappy with the refractive outcome for any reason. Dr. Bloomenstein feels it's important to validate the patient's concern. Sometimes it's helpful to demonstrate their vision before and after to really show them the areas that they have improved. As long as you don't abandon the patient and are willing to sit down and discuss solutions, you can usually find a way to solve the problem successfully.
Conclusion
Keeping open communication
Good collaborative care requires defined roles, doctors who have similar care philosophies and are willing to communicate readily. According to Dr. Martin, collaborative care of cataract patients is not difficult “as long as you’re a kind, compassionate, knowledgeable person and you open up lines of communication.”
From the optometrist standpoint, communication starts with patient education and sending a referral letter to the surgeon. Information should flow both ways throughout the process. After the initial evaluation, the surgeon should send correspondence back to the referring doctor with updates. By following this guidance and the best practices discussed above, optometrists and ophthalmologists can establish a smooth continuum of care. After all, we are a team with a common interest-to care for our patient and give them the best vision and visual opportunities possible.
References
- Data on file. Eyhance DFU Z311524E: TECNIS Eyhance IOL with TECNIS Simplicity Delivery System.
- TECNIS Monofocal IOL with TECNIS Simplicity® Delivery System (package insert, DFU DCB00 (Z311063P Rev. D).
- Market Scope 2020 Global IOL Report.
- Data on file. Eyhance DFU.
- Market Scope, Data as of 2013. Comprehensive Report on Global IOL Market.
- Conrad-Hengerer I, Al Juburi M, Schultz T, Hengerer FH, Dick HB. Corneal endothelial cell loss and corneal thickness in conventional compared with femtosecond laser–assisted cataract surgery: three-month follow-up. J Cataract Refract Surg 2013; 39:1307–1313.
- Day AC, Gartry DS, Maurino V, Allan B, Stevens JD. Efficacy of anterior capsulotomy creation in femtosecond laser-assisted cataract surgery. J Cataract Refract Surg 2014; 40:2031-2034.
- Krueger R, Talamo J, Lindstrom, R. Textbook of Refractive Laser-Assisted Cataract Surgery (ReLACS). 2013. 10.1007/978-1-4614-1010-2.
Important Safety Information
INDICATIONS AND IMPORTANT SAFETY INFORMATION for the TECNIS® Family of 1-Piece IOLs
Rx Only
INDICATIONS and IMPORTANT SAFETY INFORMATION for TECNIS Symfony™ and TECNIS Symfony™ TORIC EXTENDED RANGE OF VISION IOLs
The TECNIS Symfony Extended Range of Vision IOL, Model ZXR00, is indicated for primary implantation for the visual correction of aphakia, in adult patients with less than 1 diopter of pre-existing corneal astigmatism, in whom a cataractous lens has been removed. The TECNIS Symfony Toric Extended Range of Vision IOLs, Models ZXT150, ZXT225, ZXT300, and ZXT375, are indicated for primary implantation for the visual correction of aphakia and for reduction of residual refractive astigmatism in adult patients with greater than or equal to 1 diopter of preoperative corneal astigmatism, in whom a cataractous lens has been removed. These models of IOLs, ZXR00, ZXT150, ZXT225, ZXT300, and ZXT375, mitigate the effects of presbyopia by providing an extended depth of focus. Compared to an aspheric monofocal IOL, these models of IOLs provide improved intermediate and near visual acuity, while maintaining comparable distance visual acuity. These models of IOLs are intended for capsular bag placement only.
INDICATIONS and IMPORTANT SAFETY INFORMATION for TECNIS Symfony™ OPTIBLUE™ and TECNIS Symfony™ TORIC II OPTIBLUE™ EXTENDED RANGE OF VISION IOLs
The TECNIS Symfony™ OptiBlue™ Extended Range of Vision IOL, Model ZXR00V, is indicated for primary implantation for the visual correction of aphakia in adult patients with less than 1 diopter of pre-existing corneal astigmatism, in whom a cataractous lens has been removed. The TECNIS Symfony™ Toric II OptiBlue™ Extended Range of Vision IOLs, Models ZXW150, ZXW225, ZXW300, ZXW375, are indicated for primary implantation for the visual correction of aphakia and for reduction of residual refractive astigmatism in adult patients with greater than or equal to 1 diopter of preoperative corneal astigmatism, in whom a cataractous lens has been removed. These models of IOLs, ZXR00V, ZXW150, ZXW225, ZXW300, ZXW375, mitigate the effects of presbyopia by providing an extended depth of focus. Compared to an aspheric monofocal IOL, these models of IOLs provide improved intermediate and near visual acuity, while maintaining comparable distance visual acuity. These models of IOLs are intended for capsular bag placement only.
INDICATIONS FOR THE TECNIS® 1-PIECE MONOFOCAL IOLS
TECNIS 1-piece lenses are indicated for the visual correction of aphakia in adult patients in whom a cataractous lens has been removed by extracapsular cataract extraction. These devices are intended to be placed in the capsular bag.
INDICATIONS FOR THE TECNIS® Multifocal 1-Piece AND TECNIS® MULTIFOCAL TORIC II IOLS
The TECNIS® Multifocal 1-Piece intraocular lenses are indicated for primary implantation for the visual correction of aphakia in adult patients with and without presbyopia in whom a cataractous lens has been removed by phacoemulsification and who desire near, intermediate, and distance vision with increased spectacle independence. The TECNIS® Multifocal Toric II lens models ZKU150, ZKU225, ZKU300, ZKU375 and ZLU150, ZLU225, ZLU300, ZLU375 are indicated for primary implantation for the visual correction of aphakia and for reduction of residual refractive astigmatism in adult patients with or without presbyopia, with greater than or equal to 1 diopter of preexisting corneal astigmatism, in whom a cataractous lens has been removed in order to provide near, intermediate and distance vision. The IOLs are intended for capsular bag placement only.
INDICATIONS FOR THE TECNIS® TORIC II 1-PIECE AND TECNIS® TORIC 1-PIECE IOLS:
The TECNIS® Toric II 1-Piece and TECNIS® Toric 1-Piece IOL posterior chamber lens is indicated for the visual correction of aphakia and pre-existing corneal astigmatism of one diopter or greater in adult patients with or without presbyopia in whom a cataractous lens has been removed by phacoemulsification and who desire improved uncorrected distance vision, reduction in residual refractive cylinder, and increased spectacle independence for distance vision. The device is intended to be placed in the capsular bag.
INDICATIONS FOR THE TECNIS EYHANCE™ AND TECNIS EYHANCE™ TORIC II IOLS:
The TECNIS Eyhance™ IOL, Model ICB00 is indicated for the visual correction of aphakia in adult patients in whom a cataractous lens has been removed by extracapsular cataract extraction. The lens is intended to be placed in the capsular bag.
The TECNIS Eyhance™ Toric II IOLs, Models ICU150-ICU600, are indicated for the visual correction of aphakia and pre-existing corneal astigmatism of one diopter or greater in adult patients with or without presbyopia in whom a cataractous lens has been removed by phacoemulsification and who desire reduction in residual refractive cylinder. The lens is intended to be placed in the capsular bag.
WARNINGS: Physicians considering lens implantation under any of the conditions described in the Directions for Use should weigh the potential risk/benefit ratio prior to implanting a lens that could increase complications or impact patient outcomes. Do not place the lens in the ciliary sulcus. Inform patients about the possibility that a decrease in contrast sensitivity and an increase in visual disturbances may affect their ability to drive a car under certain environmental conditions, such as driving at night or in poor visibility conditions.
Rotation of the TECNIS® Toric, TECNIS® Toric II 1-Piece, TECNIS Eyhance™ Toric II and TECNIS Symfony™ Toric II OptiBlue™ IOLs away from its intended axis can reduce its astigmatic correction. Misalignment greater than 30° may increase postoperative refractive cylinder. If necessary, lens repositioning should occur as early as possible, prior to lens encapsulation. All preoperative surgical parameters are important when choosing a toric lens for implantation. Carefully remove all viscoelastic and do not over-inflate the capsular bag at the end of the case.
Precautions: Prior to surgery, inform prospective patients of the possible risks and benefits associated with the use of this device and provide a copy of the patient information brochure to patient. The long-term effects of intraocular lens implantation have not been determined. Secondary glaucoma has been reported occasionally in patients with controlled glaucoma who received lens implants. Do not reuse, resterilize or autoclave.
ADVERSE EVENTS: The most commonly reported adverse events that occurred during the clinical trials of the TECNIS 1-Piece lenses was macular edema and secondary surgical re-intervention.
ATTENTION: Reference the Directions for Use for a complete listing of Indications and Important Safety Information.
INDICATIONS AND IMPORTANT SAFETY INFORMATION for TearScience® LIPIFLOW® Thermal Pulsation System
Rx Only
INDICATIONS
The TearScience® LipiFlow® Thermal Pulsation System is intended for the application of localized heat and pressure therapy in adult patients with chronic cystic conditions of the eyelids, including meibomian gland dysfunction (MGD), also known as evaporative dry eye or lipid deficiency dry eye.
CONTRAINDICATIONS
Do not use the TearScience® LipiFlow® System in patients with the following conditions. Use of the device in patients with these conditions may cause injury. Safety and effectiveness of the device have not been studied in patients with these conditions.
- Ocular surgery within prior 3 months, including intraocular, oculo-plastic, corneal or refractive surgery procedure
- Ocular injury within prior 3 months
- Ocular herpes of eye or eyelid within prior 3 months
- Active ocular infection (e.g., viral, bacterial, mycobacterial, protozoan, or fungal infection of the cornea, conjunctiva, lacrimal gland, lacrimal sac, or eyelids including a hordeolum or stye)
- Active ocular inflammation or history of chronic, recurrent ocular inflammation within prior 3 months (e.g., retinitis, macular inflammation, choroiditis, uveitis, iritis, scleritis, episcleritis, keratitis)
- Eyelid abnormalities that affect lid function (e.g., entropion, ectropion, tumor, edema, blepharospasm, lagophthalmos, severe trichiasis, severe ptosis)
- Ocular surface abnormality that may compromise corneal integrity (e.g., prior chemical burn, recurrent corneal erosion, corneal epithelial defect, Grade 3 corneal fluorescein staining, or map dot fingerprint dystrophy)
PRECAUTIONS
The Activator or Activator II (Disposable) may not fit all eyes, such as eyes with small palpebral fornices.
Use of the TearScience® LipiFlow® System in patients with the following conditions may result in reduced treatment effectiveness because these conditions may cause ocular symptoms unrelated to cystic meibomian glands and require other medical management. Safety and effectiveness of the device have not been studied in patients with these conditions.
- Moderate to severe (Grade 2-4) allergic, vernal or giant papillary conjunctivitis
- Severe (Grade 3 or 4) eyelid inflammation (e.g., blepharochalasis, staphylococcal blepharitis or seborrheic blepharitis). Patients with severe eyelid inflammation should be treated medically prior to device use.
- Systemic disease conditions that cause dry eye (e.g., Stevens-Johnson syndrome, vitamin A deficiency, rheumatoid arthritis, Wegener’s granulomatosis, sarcoidosis, leukemia, Riley-Day syndrome, systemic lupus erythematosus, Sjögren's syndrome)
- Taking medications known to cause dryness (e.g., isotretinoin (Accutane®) and systemic antihistamines)
- Esthetic eyelid and eyelash procedures (e.g., blepharoplasty, lash extensions, eyelid tattooing)
In addition, the treatment procedure may loosen previously inserted punctal plugs, which may worsen the patient’s dry eye symptoms.
ADVERSE EFFECTS
Potential adverse effects that may occur as a result of the procedure include, but are not limited to, the onset or increase in:
- Eyelid/eye pain requiring discontinuation of the treatment procedure;
- Eyelid irritation or inflammation (e.g., edema, bruising, blood blister, dermatitis, hordeolum or chalazion);
- Ocular surface irritation or inflammation (e.g., corneal abrasion, conjunctival edema or conjunctival injection (hyperemia)); and
- Ocular symptoms (e.g., burning, stinging, tearing, itching, discharge, redness, foreign body sensation, visual disturbance, sensitivity to light).
Potential serious adverse events (defined as permanent impairment or damage to a body structure or function or necessitates medical or surgical intervention to preclude permanent impairment or damage to a body structure or function) that are not anticipated because of the device mitigations to prevent occurrence include:
- Thermal injury to the eyelid or eye, including conjunctiva, cornea or lens;
- Physical pressure-induced injury to the eyelid; and
- Ocular surface (corneal) infection.
ATTENTION
Reference the TearScience® LipiFlow Thermal Pulsation System Instructions for Use for a complete listing of indications, warnings, and precautions.
Reference the TearScience® LipiFlow Thermal Pulsation System Instructions for Use for a complete listing of indications, warnings, and precautions.
INDICATION & IMPORTANT SAFETY INFORMATION FOR THE CATALYS® Precision Laser System
Rx Only
Indications
The CATALYS® Precision Laser System is indicated for use in patients undergoing cataract surgery for removal of crystalline lens. Intended uses in cataract surgery include anterior capsulotomy, phacofragmentation, and the creation of single plane and multi-plane arc cuts/incisions in the cornea, each of which may be performed either individually or consecutively during the same procedure.
Contraindications
The CATALYS® System is contraindicated in patients with corneal ring and/or inlay implants, sever corneal opacities, corneal abnormalities, significant corneal edema or diminished aqueous clarity that obscures OCT imaging of the anterior lens capsule, patients younger than 22 years of age, descemetocele with impending corneal rupture, and any contraindications to cataract surgery.
Warnings
Prior to INTEGRAL GUIDANCE System imaging and laser treatment, the suction ring must be completely filled with sterile buffered saline solution. If any air bubbles and/or a meniscus appear on the video image before treatment, do not initiate laser treatment. Before initiating laser treatment, inspect images created from the OCT data, surface fits, and overlaid pattern in both axial and sagittal views, and review the treatment parameters on the Final Review Screen for accuracy. Safety margins for all incisions are preserved only if Custom Fit Adjustments to ocular surface(s) are applied in accordance with the instructions for use. Purposeful misuse of the Custom Fit Adjustment to ocular surfaces can result in patient injury and complication(s), and therefore must be avoided. Standard continuous curvilinear capsulorhexis (CCC) surgical technique must be sued for surgical removal of the capsulotomy disc. The use of improper capsulotomy disc removal technique may potentially cause or contribute to anterior capsule tear and/or a noncircular, irregularly shaped capsulotomy. Verify that the suction ring is correctly connected to the disposable lens component of the LIQUID OPTICS Interface during the initial patient docking procedure.
Precautions
The CATALYS® System has not been adequately evaluated in patients with a cataract greater than Grade 4 (via LOCS III); therefore no conclusions regarding either the safety or effectiveness are presently available. Cataract surgery may be more difficult in patients with an axial length less than 22 mm or greater than 26 mm, and/or an anterior chamber depth less than 2.5 mm due to anatomical restrictions. Use caution when treating patients who may be taking medications such as alpha blockers (e.g. Flomax) as these medications may be related to Intraoperative Floppy Iris Syndrome (IFIS); this condition may include poor preoperative dilation, iris billowing and prolapse, and progress intraoperative miosis. These conditions may require modification of surgical technique such as the utilization of iris hooks, iris dilator rings, or viscoelastic substances. Surgical removal of the cataract more than 30 minutes after the laser capsulotomy and laser lens fragmentation has not been clinically evaluated. The clinical effects of delaying surgical removal more than 30 minutes after laser anterior capsulotomy and laser lens fragmentation are unknown. The LIQUID OPTICS Interface is intended for single patient use only. Full-thickness corneal cuts or incisions should be performed with instruments and supplies on standby, to seal the eye in case of anterior chamber collapse or fluid leakage. Patients who will undergo full-thickness corneal incisions with the CATALYS® System should be given the same standard surgical preparation as used for patients undergoing cataract surgery for the removal of the crystalline lens. During intraocular surgery on patients who have undergone full-thickness corneal incisions with the CATALYS® System, care should be taken if an eyelid speculum is used, in order to limit pressure from the speculum onto the open eye. Patients who will be transported between the creation of a full-thickness corneal incision and the completion of intraocular surgery should have their eye covered with a sterile rigid eye shield, in order to avoid inadvertent eye injury during transport. Patients must be able to lie flat and motionless in a supine position and able to tolerate local or topical anesthesia.
Adverse Effects
Complications associated with the CATALYS® System include mild Petechiae and subconjunctival hemorrhage due to vacuum pressure of the LIQUID OPTICS Interface Suction ring. Potential complications and adverse events generally associated with the performance of capsulotomy and lens fragmentation, or creation of partial-thickness or full-thickness cut or incision of the cornea, include: Acute corneal clouding, age-related macular degeneration, amaurosis, anterior and/or posterior capsule tear/rupture, astigmatism, capsulorhexis notch during phacoemulsification, capsulotomy/lens fragmentation or cut/incision decentration, cells in anterior chamber, choroidal effusion or hemorrhage, conjunctival hyperemia/injection/erythema/chemosis, conjunctivitis (allergic/viral), corneal abrasion/depithelization/epithelial defect, corneal edema, cystoid macula edema, Descemet’s detachment, decentered or dislocated intraocular lens implant, diplopia, dropped or retained lens, dry eye/superficial punctate keratitis, edema, elevated intraocular pressure, endothelial decompensation, floaters, glaucoma, halo, inflammation, incomplete capsulotomy, intraoperative floppy iris syndrome, iris atrophy/extrusion, light flashes, meibomitis, ocular discomfort (e.g., pain, irritation, scratchiness, itching, foreign body sensation), ocular trauma, petechiae, photophobia, pigment changes/pigment in corneal endothelium/ foveal region, pingueculitis, posterior capsule opacification, posterior capsule rupture, posterior vitreous detachment, posteriorly dislocated lens material, pupillary contraction, red blood cells in the anterior chamber (not hyphema), residual cortex, retained lens fragments, retinal detachment or hemorrhage, scar in Descement’s membrane, shallowing or collapsing of the anterior chamber, scoring of the posterior corneal surface, snailtrack on endothelium, steroid rebound effect, striae in Descement’s, subconjunctival hemorrhage, thermal injury to adjacent eye tissues, toxic anterior shock syndrome, vitreous in the anterior chamber, vitreous band or loss, wound dehiscence, wound or incision leak, zonular dehiscence.
Caution
Federal law (USA) restricts this device to sale by or on the order of a physician. The system should be used only by qualified physicians who have extensive knowledge of the use of this device and have been trained or certified.
Attention
Reference the Directions for Use for a complete listing of indications, warnings, and precautions.



