



What are flame hemorrhages?
Flame hemorrhages are a subset of retinal hemorrhages occurring within the retinal nerve fiber layer.1 They are related to pathologies of the superficial retinal capillary plexus,1 including hypertensive retinopathy and retinal venous occlusion.2,3
In general, hemorrhages are precipitated by breakdown of vessel walls; wall instability etiologies can include: physical pressure from trauma or surgery, increased pressure within the vessels, wall inflammation, weak connective tissue, and/or systemic coagulation pathologies.4
Flame hemorrhages on exam
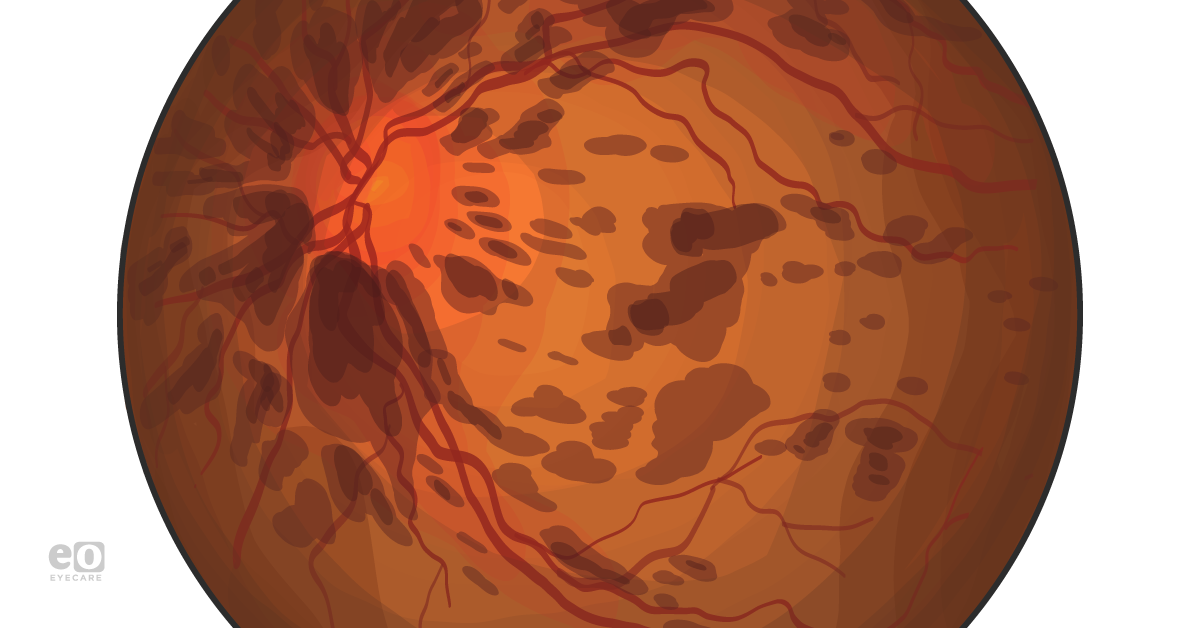
On exam, flame hemorrhages are usually found in the posterior pole of the retina;4 they may be around the optic nerve in diseases such as glaucoma.2 However, they are uncommon in the periphery of the retina, unlike another form of retinal hemorrhages called “dot and blot” hemorrhages.5
Flame hemorrhages are typically red in color and elliptical or “lozenge” shaped.4 The outer rim of flame hemorrhages is not completely smooth; some parts will be serrated4 or feathery in appearance.2
Flame hemorrhages should not be confused with other retinal hemorrhages of the retinal nerve fiber layer: Roth spots and disc hemorrhages. Roth spots have a white center and their shape is rounder. Disc hemorrhages have a splinter shape that becomes narrower as its ends approach the optic disc.1
Flame hemorrhage formation pathophysiology
The more elongated, linear shape of these hemorrhages is produced by the pattern of blood movement as it infiltrates the nerve fiber layer. The blood mirrors the parallel arrangement of the axons5 of the retina in an arching pattern on both sides of the fovea in accordance with the positioning of the retinal nerve fiber bundles.6
Differential diagnosis of flame hemorrhage
When a flame hemorrhage is found on exam, it can be difficult to determine its underlying etiology because there are many possibilities. While this is not an exhaustive list, some conditions that should be kept in mind, based on current literature and case reports, are as follows:
Infectious etiologies
- Acute bacterial endocarditis1
- Dengue fever7
- Hemolytic uremic syndrome8
- Post-fever retinitis
- Potential consequence of systemic infections such as West Nile fever, Rickettsiosis, Typhoid fever and Rubella. Researchers are not sure whether the retinitis here is infection or immune-mediated (or both).9
- Acquired Immunodeficiency Syndrome (AIDS)10
Microvascular etiologies
- Hypertensive retinopathy,1, including underlying issues such as:
- malignant hypertension11
- hypertensive emergencies12
- pregnancy-induced hypertension13
- Glaucoma14
- Aneurysmal subarachnoid hemorrhage15
- Branch retinal vein occlusions5
- Papilledema16
- Collagen vascular disease16
Autoimmune etiologies
- Diabetic retinopathy17
- Systemic sarcoidosis18
- Lupus19
- IRVAN (idiopathic retinal vasculitis, aneurysms, and neuroretinitis syndrome) with p-ANCA positivity20
Hematologic etiologies
- Hematologic cancers
- Leukemia1
- Multiple myeloma21
- Anemias21
- Aplastic anemia
- Pernicious anemia
- Iron deficiency anemia
- Megaloblastic anemia
- Hemolytic anemia
- COVID, with high D-dimer22
- Thrombocytopenia16
- Anoxia16
- Coagulopathies16
Traumatic etiologies
- Birthing-mediated traumas (e.g., instrument-assisted)23
- Dental procedures (ie., that can lead to branch retinal artery occlusion)24
- Coronary artery bypass graft (possible relation to ischemic optic neuropathy, for instance)25
- Shaken baby syndrome26
- Blunt trauma16
Miscellaneous etiologies
- Retinopathy of prematurity27
- After certain medications
- One case report described flame hemorrhages in a patient after beginning fingolimod for Multiple Sclerosis28
- Thiamine deficiency-induced Wernicke encephalopathy29
- Radiation16
Management
Because most flame hemorrhages do not involve the fovea, they will not lead to blindness and can just be observed.1 This is particularly true if there is a single flame hemorrhage found on exam; in that case, further ocular-specific management can focus on watching for progression, signs of ischemia, and neovascularization.1
The main focus will then be on determining the basis of the flame hemorrhage. Most flame hemorrhages will typically resolve after addressing the systemic predispositions in a patient. Thus, it is critical to use an interprofessional team to assess and treat the patient.1
An important aspect of determining how to determine follow-up in patients is getting a thorough history. Discussion questions should address social history, medications, any trauma, or recent changes in vision, for example.1
After a history, a typical ophthalmic examination for evaluation of flame hemorrhages should involve: slit lamp examination, dilated fundoscopy, and intraocular pressure measurements.1
In terms of further workup to rule out any systemic conditions, referrals should be made so that the patient can have etiology-specific labs drawn. For example, patient levels of serum lipids, plasma proteins, and plasma glucose should be checked to evaluate for metabolic syndrome.1
Blood viscosity should be evaluated via measurement of hemoglobin, hematocrit, and fibrinogen. If there is a concern for an autoimmune basis to hyperviscosity, measurements of protein C, protein S, factor V leiden, homocysteine, and antithrombin III should be performed.30 Coagulation factors and M-type globulins can also be checked to evaluate for hemorrhages in the setting of multiple myeloma.31
If flame hemorrhages are suspected to be secondary to hypertension, blood urea nitrogen, workup for basic electrolyte levels, creatinine clearance, urine samples, and renal imaging is reasonable.31 In cases of retinopathy in the setting of hypertensive crises, labetalol is typically the first line for management.32
Birth trauma-induced retinal hemorrhages in newborns can be managed conservatively; they typically normalize in 2-4 weeks. However, if the patient is younger than 3 years and has retinal hemorrhages in addition to an intracranial injury, there should be high suspicion for child abuse.1
References
- Kanukollu VM, Ahmad SS. Retinal Hemorrhage. [Updated 2020 Aug 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560777
- Kaiser, P. K., MD, Friedman, N. J., MD, & Pineda II, R., MD. (2014). Hemorrhages. In The Massachusetts Eye and Ear Infirmary Illustrated Manual of Ophthalmology (4th ed., pp. 331-332). Elsevier.
- Emerson, G. G., MD, Francis, P. J., MD, Wilson, D. J., MD, & Garner, A., MD. (2008). Vascular Diseases. In 1256457220 929903031 G. K. Klintworth MD & 1256457221 929903031 A. Garner MD (Authors), Garner and Klintworth's pathobiology of ocular disease (3rd ed., p. 1445). New York, NY: Informa Healthcare.
- Kaur, B., & Taylor, D. (1990). Retinal haemorrhages. Archives of disease in childhood, 65(12), 1369–1372. https://doi.org/10.1136/adc.65.12.1369
- Muraoka, Y., Uji, A., Tsujikawa, A., Murakami, T., Ooto, S., Suzuma, K., Takahashi, A., Iida, Y., Miwa, Y., Hata, M., & Yoshimura, N. (2016). Association between retinal hemorrhagic pattern and macular perfusion status in eyes with acute branch retinal vein occlusion. Scientific reports, 6, 28554. https://doi.org/10.1038/srep28554
- Eagle, R. C., MD. (2011). Retina. In Eye Pathology: An Atlas and Text (2nd ed., p. 138). Wolters Kluwer Health/Lippincott Williams & Wilkins.
- Chuah, K. H., Ng, C. W., Zabri, K., & Wong, C. L. (2017). Unusual presentation of severe dengue: Dengue maculopathy. The Medical journal of Malaysia, 72(1), 73–74.
- Geraissate, J. C., Yamamoto, R. E., Isaac, D. L., & Ávila, M. P. (2014). Hemorrhagic retinopathy in an infant with hemolytic-uremic syndrome. Arquivos brasileiros de oftalmologia, 77(6), 397–399. https://doi.org/10.5935/0004-2749.20140099
- Sundar M, D., Chawla, R., Balaji, A., Garg, I., Kalathil, R., Hasan, N., Vikas, S. J., & Kumar, A. (2020). Clinical features, optical coherence tomography findings and treatment outcomes of post-fever retinitis. Therapeutic advances in ophthalmology, 12, 2515841420979111. https://doi.org/10.1177/2515841420979111
- Igor Kozak, J. Allen McCutchan, William R. Freeman, Chapter 81 - HIV-Associated Infections, Editor(s): Stephen J. Ryan, SriniVas R. Sadda, David R. Hinton, Andrew P. Schachat, SriniVas R. Sadda, C.P. Wilkinson, Peter Wiedemann, Andrew P. Schachat,Retina (Fifth Edition), W.B. Saunders,2013,Pages 1441-1472, ISBN 9781455707379,https://doi.org/10.1016/B978-1-4557-0737-9.00081-3. (https://www.sciencedirect.com/science/article/pii/B9781455707379000813)
- Januszewicz, A., Guzik, T., Prejbisz, A., Mikołajczyk, T., Osmenda, G., & Januszewicz, W. (2016). Malignant hypertension: new aspects of an old clinical entity. Polskie Archiwum Medycyny Wewnetrznej, 126(1-2), 86–93.
- Van den Born, B. J., Beutler, J.J., Gaillard, C.A., de Gooijer, A., van den Meiracker, A. H., & Kroon, A.A. (2011). Dutch guideline for the management of hypertensive crisis--2010 revision. The Netherlands journal of medicine, 69(5), 248-255.
- Bakhda R. N. (2016). Clinical study of fundus findings in pregnancy induced hypertension. Journal of family medicine and primary care, 5(2), 424–429. https://doi.org/10.4103/2249-4863.192364
- Ozturker, Z. K., Munro, K., & Gupta, N. (2017). Optic disc hemorrhages in glaucoma and common clinical features. Canadian Journal of Ophthalmology, 52(6), 583-591. doi:10.1016/j.jcjo.2017.04.011
- Obuchowska, I., Turek, G., Mariak, Z., & Mariak, Z. (2014). Early Intraocular Complications of Subarachnoid Haemorrhage after Aneurysm Rupture. Neuro-ophthalmology (Aeolus Press), 38(4), 199–204. https://doi.org/10.3109/01658107.2014.911918
- Witkin, A. (2012). Retinal Hemorrhage. In 1256410775 929875626 J. I. Maguire MD, 1256410776 929875626 A. P. Murchison MD, MPH, & 1256410777 929875626 E. A. Jaeger MD (Eds.), Willis Eye Institute 5-Minute Ophthalmology Consult (p. 37). Philadelphia, PA: Lippincott Williams & Wilkins.
- Nghiem, A.Z., Nderitu, P., Lukic, M., Khatun, M., Largan, R., Kortuem, K., Balaskas, K. and Sim, D. (2019), Comparing diabetic retinopathy lesions in scanning laser ophthalmoscopy and colour fundus photography. Acta Ophthalmol, 97: e1035-e1040. https://doi.org/10.1111/aos.14106
- Hiraoka M. (2020). Severe visual impairment due to an optic neuropathy and central retinal vein occlusion in a sarcoidosis patient. Journal of ophthalmic inflammation and infection, 10(1), 6. https://doi.org/10.1186/s12348-020-0198-3
- Shrestha, R., Kharel Sitaula, R., Karki, P., Joshi, S. N., & Rawal, S. (2019). Combined Intravitreal Bevacizumab And Dexamethasone In Bilateral Lupus Retinopathy. International medical case reports journal, 12, 329–333. https://doi.org/10.2147/IMCRJ.S220499
- Nourinia, R., Montahai, T., Amoohashemi, N., Hassanpour, H., & Soheilian, M. (2011). Idiopathic retinal vasculitis, aneurysms and neuroretinitis syndrome associated with positive perinuclear antineutrophil cytoplasmic antibody. Journal of ophthalmic & vision research, 6(4), 330–333.
- Holt, J. M., & Gordon-Smith, E. C. (1969). Retinal abnormalities in diseases of the blood. The British journal of ophthalmology, 53(3), 145–160.
- Lani-Louzada, R., Ramos, C., Cordeiro, R. M., & Sadun, A. A. (2020). Retinal changes in COVID-19 hospitalized cases. PloS one, 15(12), e0243346. https://doi.org/10.1371/journal.pone.0243346
- Watts, P., Maguire, S., Kwok, T., Talabani, B., Mann, M., Wiener, J., . . . Kemp, A. (2013). Newborn retinal hemorrhages: A systematic review. Journal of American Association for Pediatric Ophthalmology and Strabismus, 17(1), 70-78. doi:10.1016/j.jaapos.2012.07.012
- Oğurel, T., Onaran, Z., Oğurel, R., Örnek, N., Büyüktortop Gökçınar, N., & Örnek, K. (2014). Branch Retinal Artery Occlusion following Dental Extraction. Case reports in ophthalmological medicine, 2014, 202834. https://doi.org/10.1155/2014/202834
- Dorecka, M., Miniewicz-Kurkowska, J., Romaniuk, D., Gajdzik-Gajdecka, U., & Wójcik-Niklewska, B. (2011). Anterior ischemic optic neuropathy after conventional coronary artery bypass graft surgery. Medical science monitor : international medical journal of experimental and clinical research, 17(6), CS70–CS74. https://doi.org/10.12659/msm.881798
- Levin, A. V., MD. (2007). Child Abuse. In 1256446490 929896883 A. V. Levin MD & 1256446491 929896883 T. W. Wilson MD (Eds.), The Hospital for Sick Children's Atlas of Pediatric Ophthalmology and Strabismus. Philadelphia, PA: Lippincott, Williams & Wilkins
- Daniel, E., Ying, G. S., Siatkowski, R. M., Pan, W., Smith, E., Quinn, G. E., & e-ROP Cooperative Group (2017). Intraocular Hemorrhages and Retinopathy of Prematurity in the Telemedicine Approaches to Evaluating Acute-Phase Retinopathy of Prematurity (e-ROP) Study. Ophthalmology, 124(3), 374–381. https://doi.org/10.1016/j.ophtha.2016.10.040
- Ueda, N., & Saida, K. (2015). Retinal hemorrhages following fingolimod treatment for multiple sclerosis; a case report. BMC ophthalmology, 15, 135. https://doi.org/10.1186/s12886-015-0125-9
- Wei-Yi Yeh, Li-Ming Lian, Anna Chang, Cheng-Kuo Cheng, Thiamine-deficient optic neuropathy associated with Wernicke's encephalopathy in patients with chronic diarrhea, Journal of the Formosan Medical Association, Volume 112, Issue 3, 2013, Pages 165-170, ISSN 0929-6646, https://doi.org/10.1016/j.jfma.2012.10.010. (https://www.sciencedirect.com/science/article/pii/S0929664612005086)
- Thomas, D., MRCOphth, & Graham, E. M., FRCP, FRCOphth. (2004). Ocular Disorders Associated With Systemic Diseases. In 1256471652 929911668 P. Riordan-Eva & 1256471653 929911668 J. P. Whitcher (Eds.), Vaughan & Asbury's General Ophthalmology (17th ed.). McGraw Hill.
- Karring, H., PhD, Meller-Pedersen, T., PhD, Enghild, J. J., PhD, & Klintworth, G. K., MD. (2008). Ocular Proteins and Proteomics. In 1256457220 929903031 G. K. Klintworth MD & 1256457221 929903031 A. Garner MD (Authors), Garner and Klintworth's pathobiology of ocular disease (3rd ed., p. 817). New York, NY: Informa Healthcare.
- H., & Kroon, A. A. (2011). Dutch guideline for the management of hypertensive crisis -- 2010 revision. The Netherlands journal of medicine, 69(5), 248–255.

