


An estimated 35 million people in the United States suffer from dry eye disease (DED), with prevalence increasing every year.1-3 Considering the steadily aging population, increases in polypharmacy, and digital device use, this rising prevalence is not surprising. Though the highest rates remain in elderly populations, it is more often being diagnosed in younger age groups.1 Researchers and practitioners in the eyecare community suggest that the COVID-19 pandemic has exacerbated symptoms of DED, with excessive evaporation of tear fluid from increased visual display use and air dispersed around the eyes from prolonged mask usage.4-6 DED contributes to considerable humanistic and economic burden,2 and can have a wide-reaching impact on quality of life, including physical discomfort, pain, and negative effects on visual functioning.7,8 Patients with DED may also experience loss in work-related productivity, especially those with prolonged use of visual displays.9 Although considered a challenging disease area, our experience suggests early diagnosis can contribute to more successful management.
Meibomian gland dysfunction (MGD), a multifactorial disorder of the ocular surface caused by obstructed meibomian glands, is the leading cause of DED and a common problem encountered in an optometric practice (Figure 1).10 In my clinic at Eye Surgeons of Indiana, about 90% of patients evaluated for DED present with some degree of MGD. As MGD is asymptomatic in its early stages, proactive measures for early diagnosis are critical for early intervention. For this reason, every new patient at the clinic is screened for DED and MGD, regardless of their chief complaint for seeking eyecare services, with routine screening thereafter.

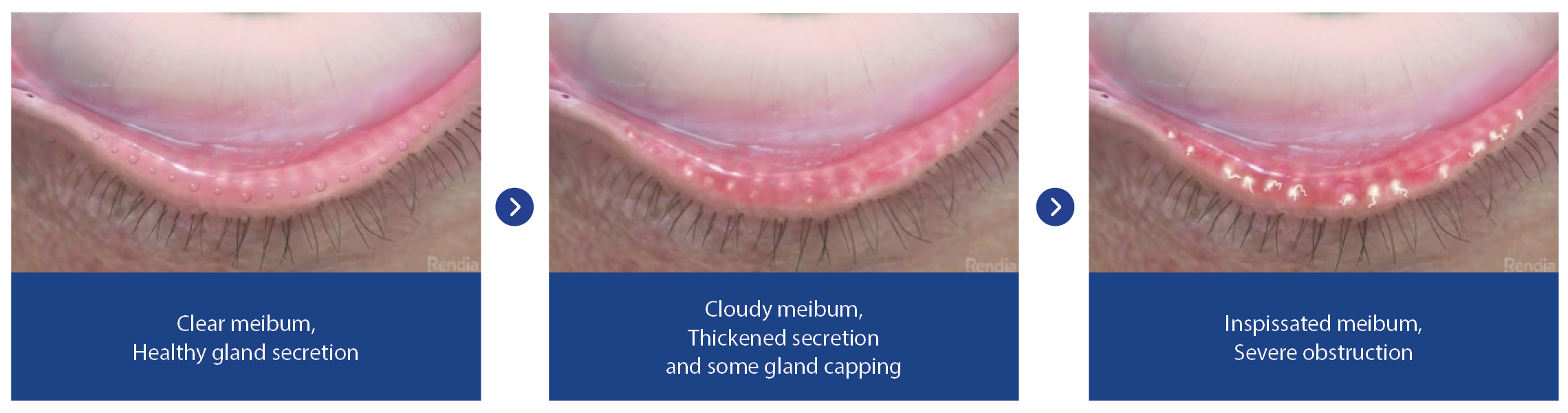
Figure 1. Meibomian gland dysfunction disease progression.
The screening process involves the Standardized Patient Evaluation of Eye Dryness (SPEED) questionnaire followed by tests to assess signs of DED and MGD (Figure 2). Regardless of symptom presentation, patients are subsequently screened for MGD, which involves manual pressure on the eyelid to determine gland obstruction and oil health. If signs or symptoms are present, we evaluate potential issues with their tear film, obtain baseline meibography images, and administer additional point-of-care diagnostic tests. Following a diagnosis, tear osmolarity, Matrix Metallopeptidase 9 (MMP9), and meibomian gland evaluation are repeated at every follow-up visit to assess disease status objectively. Objective measurements are critical for determining if a patient’s condition is progressing or regressing. Patients who had no signs or symptoms of DED or MGD at first screening undergo the screening process at every comprehensive examination. With early diagnosis and a proactive approach to treatment, patients with MGD, regardless of symptom presence, can take steps to promote normal functioning of their meibomian glands in an effort to alleviate symptoms dry eye.

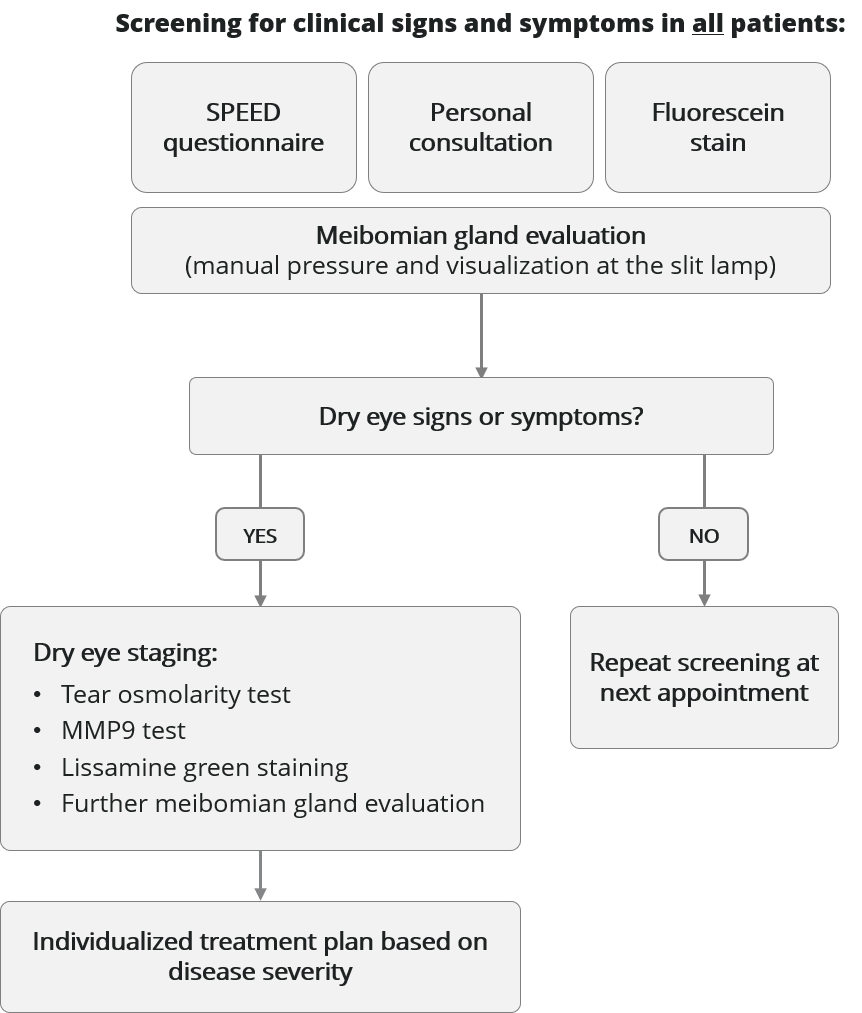
Figure 2. Screening procedure used at Eye Surgeons of Indiana.
1, 2, 3: Inflammation, Biofilm, Obstruction
In our practice, we formulate an individualized treatment plan per patient, based on disease stage and symptom severity, starting with a more comprehensive strategy, and then scaling back for maintenance. Inflammation can play an important role for many dry eye patients, which can be addressed with a variety of methods, such as topical steroids, topical immunomodulators, nutritional supplements, and/or other interventions. Lid margin biofilm, when present, can be addressed with an in-office lid debridement and exfoliation, and daily at-home lid hygiene. In the presence of MGD, the meibomian gland obstruction can be treated using thermal pulsation therapy. Thorough screening and diagnosis are very important, as patients with asymptomatic MGD may benefit from early management of their gland obstruction with thermal pulsation. It is important to educate patients on the chronic, progressive nature of MGD and why early management of the root cause of dry eye symptoms is critical.
Thermal Pulsation Therapy
In our experience at Eye Surgeons of Indiana, treatment with thermal pulsation is an effective option for management of obstruction from MGD. Thermal pulsation systems have been offered at our clinics for the past five years, first with the integration of the LipiFlow® device (Johnson & Johnson), then with Systane® iLux® (Alcon Vision, LLC) and TearCare® (Sight Sciences). The LipiFlow® and Systane® iLux® devices work well for meibomian gland obstruction and symptomatic MGD, with Systane® iLux® allowing for direct visualization of the glands during the procedure. The dominant device selected by our optometrists has been Systane® iLux®, primarily due to its compact, portable design and ease of implementation (Figure 3).


Figure 3. The Systane® iLux® device.
As a battery-operated hand-held unit, Systane® iLux® does not require connection to a console or a dedicated procedure room. In addition to its portability, other benefits include its disposable tips allowing for sterile use and easy sanitization. It has been clinically demonstrated to reduce the signs and symptoms of MGD,11 and is an efficient treatment in the market of FDA-approved options. Reduced chair time and the portability contribute substantially to patient throughput. Further to that, the Systane® iLux® device is used by our care providers for patients with challenging lid anatomy. The device uniquely offers direct visualization of the treatment area, enabling confirmation that the meibum has been liquified and the obstruction cleared.
We observe an improvement in dry eye symptoms in about 80% of patients within the first month of thermal pulsation therapy. Depending on disease severity, a single treatment can provide relief. I recommend patients continue with a home care regimen including lid hygiene and warm compress therapy. I have achieved a conversion rate of approximately 70% when recommending thermal pulsation treatment to my patients. While it is a highly effective management option, it is important to communicate to patients that it is not a cure, and that follow-up is important to manage this chronic disease effectively. Frequency of follow-up depends on disease severity, but our preference is to evaluate patients at two months to assess changes in symptoms, and every four to six months thereafter to determine when a repeat procedure may be necessary.
From a practice perspective, another aspect of value for the Systane® iLux® device is the Dry Eye Excellence Program (DEEP™) provided by the manufacturer (Alcon Vision, LLC) (Figure 4). This program provides critical tools for integration of the technology into the clinic: educational materials for patients, optometrists, and other staff, as well as help with developing a protocol and proper messaging. Given its ease-of-use, multiple technicians at our clinic have been trained to perform thermal pulsation procedures with Systane® iLux®, and with the help of the DEEP™ program, I plan to expand this training to additional personnel.


Figure 4. The Dry Eye Excellence Program (DEEP™)
Next to refractive error, dry eye is one of the most common ocular issues encountered by eye care professionals.12 As such, delivering dry eye services to patients is necessary for any optometry practice wanting to deliver comprehensive care. Given its increasing prevalence, negative impact on quality of life, and high proportion of asymptomatic disease, eyecare professionals should embrace screening for DED and MGD as an essential part of every routine exam. Finally, as professionals serious about ocular health, it is incumbent upon us to deliver an effective strategy for screening, diagnosis, and treatment.
IMPORTANT PRODUCT INFORMATION
Indication: The Systane® iLux® device is indicated for the application of localized heat and pressure therapy in adult patients with chronic disease of the eyelids, including Meibomian Gland Dysfunction (MGD), also known as evaporative dry eye.
Contraindications:
Do NOT use the Systane® iLux® device in patients with the following conditions: Patients whose pupils have been pharmaceutically dilated; patients who have undergone ocular surgery within prior 12 months; patients with ocular injury or trauma, chemical burns, or limbal stem cell deficiency (within prior 3 months); patients with active ocular herpes zoster or simplex of eye or eyelid or a history of these within prior 3 months; patients with cicatricial lid margin disease; patients with active ocular infection, active ocular inflammation or history of chronic, recurrent ocular inflammation within prior 3 months; patients with an ocular surface abnormality that may compromise corneal integrity; patients with lid surface abnormalities that affect lid function in either eye; patients with aphakia; or patients with permanent makeup or tattoos on their eyelids.
Warnings/Precautions:
Federal law restricts this device to sale by or on the order of a licensed healthcare practitioner.
The Disposable may not fit all eyes, such as eyes with small palpebral fornices. Use of the Systane® iLux® device is NOT recommended in patients with the following conditions: moderate to severe allergic, vernal or giant papillary conjunctivitis; severe eyelid inflammation; systemic disease conditions that cause dry eye; in patients who are taking medications known to cause dryness; or patients with punctal plugs.
Potential Adverse Reactions:
Potential adverse effects may include eyelid/eye pain requiring discontinuation of the treatment procedure, eyelid irritation or inflammation, temporary reddening of the skin, ocular surface irritation or inflammation (e.g., corneal abrasion, conjunctive edema or conjunctival injection (hyperemia)), and ocular symptoms (e.g., burning, stinging, tearing, itching, discharge, redness, foreign body sensation, visual disturbance, sensitivity to light).
Attention: Please refer to the User Manual for a complete list of contraindications, instructions for use, warnings and precautions for the Systane® iLux® device.
© 2021 Alcon Inc. 04/21 US-ILU-2100040
References
- Dana R, Bradley JL, Guerin A, Pivneva I, Stillman I et al. (2019) Estimated Prevalence and Incidence of Dry Eye Disease Based on Coding Analysis of a Large, All-age United States Health Care System. Am J Ophthalmol 202 47-54.
- Stapleton F, Alves M, Bunya VY, Jalbert I, Lekhanont K et al. (2017) TFOS DEWS II Epidemiology Report. Ocul Surf 15 (3): 334-365.
- US Census Bureau (2020). Annual Estimates of the Resident Population for Selected Age Groups by Sex for the United States: April 1, 2010 to July 1, 2019 (NC-EST2019-AGESEX). Available online at: https://www.census.gov/newsroom/press-kits/2020/population-estimates-detailed.html. Accessed:
- Giannaccare G, Vaccaro S, Mancini A, Scorcia V (2020) Dry eye in the COVID-19 era: how the measures for controlling pandemic might harm ocular surface. Graefes Arch Clin Exp Ophthalmol 258 (11): 2567-2568.
- Moshirfar M, West WB, Jr., Marx DP (2020) Face Mask-Associated Ocular Irritation and Dryness. Ophthalmol Ther 9 (3): 397-400.
- Pandey SK, Sharma V (2021) Mask-associated dry eye disease and dry eye due to prolonged screen time: Are we heading towards a new dry eye epidemic during the COVID-19 era? Indian J Ophthalmol 69 (2): 448-449.
- Dana R, Meunier J, Markowitz JT, Joseph C, Siffel C (2020) Patient-Reported Burden of Dry Eye Disease in the United States: Results of an Online Cross-Sectional Survey. Am J Ophthalmol 216 7-17.
- Hossain P, Siffel C, Joseph C, Meunier J, Markowitz JT et al. (2021) Patient-reported burden of dry eye disease in the UK: a cross-sectional web-based survey. BMJ Open 11 (3): e039209.
- Uchino M, Uchino Y, Dogru M, Kawashima M, Yokoi N et al. (2014) Dry eye disease and work productivity loss in visual display users: the Osaka study. Am J Ophthalmol 157 (2): 294-300.
- Geerling G, Baudouin C, Aragona P, Rolando M, Boboridis KG et al. (2017) Emerging strategies for the diagnosis and treatment of meibomian gland dysfunction: Proceedings of the OCEAN group meeting. Ocul Surf 15 (2): 179-192.
- Tauber J, Owen J, Bloomenstein M, Hovanesian J, Bullimore MA (2020) Comparison of the iLUX and the LipiFlow for the Treatment of Meibomian Gland Dysfunction and Symptoms: A Randomized Clinical Trial. Clin Ophthalmol 14 405-418.
- Bradley JL, Özer Stillman I, Pivneva I, Guerin A, Evans AM et al. (2019) Dry eye disease ranking among common reasons for seeking eye care in a large US claims database. Clin Ophthalmol 13 225-232.
