


“Pink eye” is one of the most common complaints eyecare providers encounter. This is not surprising considering “pink eye” is a catch-all term used to describe red, watery eyes. Likewise, conjunctivitis, the clinical term for “pink eye” is also a broad classification that encompasses many different conditions with varied underlying causes but similar signs and symptoms. Conjunctivitis affects nearly six million people annually in the U.S.1 and accounts for about 1% of all primary care visits and 28% of ER visits.2,3
Table of Contents
Clinical presentation
Clinical presentation
Conjunctivitis specifically refers to the inflammation of the bulbar and palpebral conjunctiva of the eye. This inflammation results in varying degrees of injection and edema, which gives “pink eye” its classic reddish-pink, swollen appearance and is often accompanied by some form of discharge.4 The underlying causes of conjunctivitis vary and include infectious etiologies such as bacterial, viral, fungal, and parasitic infections as well as noninfectious causes like allergies, inflammatory conditions, and mechanical irritation.
Accurately diagnosing the specific cause of conjunctivitis has been shown to be a challenge for providers, as 80% of cases of infectious conjunctivitis are treated with antibiotics, while only 30% of cases are truly bacterial in nature.5 However, while the different forms of conjunctivitis may present in similar fashions, there are key differences, although sometimes subtle, that help differentiate them.
It is critical for eyecare providers (ECPs) to identify these differences quickly and accurately, as the treatments for the various forms of conjunctivitis can differ significantly. Fortunately, there are several hallmark features that make delineating the different causes of conjunctivitis relatively straightforward.
Conjunctivitis can be caused by many underlying factors, but all forms tend to share the basic presentation of red, irritated eyes, with some form of discharge as seen in Figure 1.


Figure 1
Making a diagnosis
Making a diagnosis
Although all forms of conjunctivitis may appear similar at a superficial level, a careful history and thorough examination will often be all that is needed to determine the exact underlying cause.
Two key pieces of information will allow ECPs to quickly categorize the nature of the condition.
1) Is the patient experiencing any discharge?
- If so, is it watery, mucoid, or stringy or ropey?
- What color is the discharge?
2) Is there a reaction of the palpebral conjunctiva?
- Are papillae present?
- Are follicles present?
- Is there a mixed reaction?
These two pieces of information–the quality of discharge and type of palpebral reaction present–will allow providers to broadly categorize the conjunctivitis as bacterial, viral, or allergic in nature, and by adding a few additional pieces of information an even more specific diagnosis can be made.
Download the Conjunctivitis Differential Diagnosis Flowcharts Now!

Conjunctivitis Differential Diagnosis Flowcharts
Use these comprehensive flowcharts to help diagnose the multiple types of conjunctivitis.

If the patient is experiencing watery discharge with a follicular reaction, that points to a viral cause. If the discharge is more mucopurulent and is yellow-green or brownish in color along with a papillary reaction, then it is likely bacterial in nature. And if the discharge is ropey and clear with papillae, then it is likely allergic in origin, which is confirmed by the presence of itching (usually absent in other forms of conjunctivitis). However, if the patient is displaying mucoid discharge with a follicular or mixed reaction, this suggests a more systemic bacterial infection, such as chlamydia.
While the patient’s history and a few targeted questions can often broadly categorize the nature of the conjunctivitis between infectious and noninfectious, and even viral, bacterial, or allergic, clinical exam findings and pertinent patient history will provide the information required to make a specific diagnosis.
Some of the more important elements to examine include:
1) How long has the condition been going on?
- Is it acute or chronic?
2) Is there corneal involvement? If so, what does it look like?
- Are the lesions dendritic? Infiltrative? Ulcerative?
3) Are the lids or lashes involved?
- Are there any lesions on the eyelids?
- Is there any debris or discharge present on the lashes?
4) Are the lymph nodes swollen?
5) Are there any systemic symptoms?
- Does the patient have a fever?
- Does the patient have a rash?
6) Is the patient a contact lens wearer?
- Do they sleep in their lenses?
- Do they swim in their lenses or rinse them with tap water?
These additional pieces of information in conjunction with the previous broad categorization will greatly narrow the possible causes of a case and often lead to a specific diagnosis, such as a herpetic infection or contact lens-induced conjunctivitis.
There are diagnostic tests on the market that aid in differentiating the causes of conjunctivitis, including the QuickVue Adenoviral Conjunctivitis Test (Quidel), which can determine if the condition is viral in nature. While tests like these can be helpful, they may be impractical to perform in the midst of a busy clinic. Therefore, by understanding the key similarities and differences between the different forms of conjunctivitis ECPs can quickly and accurately diagnose the cause of a patient’s condition and initiate the appropriate treatment.
Included below are the broad categories of conjunctivitis such as bacterial, viral, fungal, and parasitic conjunctivitis, in addition to noninfectious forms such as allergic, inflammatory, and mechanical. These are further broken down into specific forms of conjunctivitis with a description of the hallmark signs and case history that differentiates each type.
Bacterial conjunctivitis
Overview
Bacterial conjunctivitis (BC) is the second leading cause of conjunctivitis in adults, and accounts for an estimated 30% of cases.6,5 BC primarily occurs in the winter and spring months.7 It tends to be more common in children than adults, as it accounts for 50-70% of cases of pediatric conjunctivitis.7 The hallmark sign of BC is mucoid or mucopurulent discharge, which is often colored (creamy-white or yellow-green to brown).8 In addition to eye redness, patients will typically report mild to moderate irritation or pain and light sensitivity, but discharge is routinely the main complaint as these patients will often report waking up with their eyes “crusted shut”.
Patients will also display a papillary reaction, and occasionally lid edema or chemosis. It is recommended that all cases involving copious, purulent discharge be cultured.9 There are numerous potential bacterial species that can cause conjunctivitis, but two of the most common are Haemophilus influenzae (a gram-negative bacterium), especially in children, and Staphylococcal species (gram-positive bacteria), which are more common in adults.10,11 The most common bacteria responsible for acute bacterial conjunctivitis include Haemophilus influenzae, Streptococcus pneumoniae, Pseudomonas aeruginosa, Neisseria gonorrhoeae, and Neisseria meningitides.11-13
Staphylococcus aureus and Moraxella lacunata are most frequently responsible for chronic bacterial conjunctivitis.14 Other potential bacterial species that are less commonly encountered include Streptococcus, Moraxella catarrhalis, Chlamydia trachomatis, Corynebacterium diphtheriae, and Mycobacterium tuberculosis.12,15,16
There are several potential avenues by which a bacterial infection can develop, such as touching an object or surface contaminated with bacteria and then touching or rubbing the eyes. Likewise, sharing contaminated towels, bedding, or makeup can also result in inoculation.7 Contact lens wearers are at greater risk of developing BC due to potential contamination of the lens, lens case or fingers when inserting or removing the lens.17 Another route of infection to be aware of, especially in younger adults, is oculo-genital contact that may occur during sexual activity.9
In other cases, bacterial infections arise from an overgrowth of normal microflora or transmission of bacteria between the sinuses and nasal mucosa to the conjunctiva.18 Acute cases of BC can develop within hours to days, while chronic forms take 2-7 days to develop and last at least 4 weeks.7,14
While most cases of BC are self-limiting and resolve in 1-2 weeks,6 some hyperacute forms involving particularly virulent bacteria pose significant risk and require urgent treatment.6 The use of topical antibiotics is helpful in quickening resolution and alleviating symptoms. A wide array of antibiotics can be utilized depending on the suspected organism responsible for the infection, though broad-spectrum antibiotics, such as fourth generation fluoroquinolones, are recommended to cover against a wide range of pathogens. Patients are also encouraged to launder all bedding and towels, discard any makeup, and dispose of contact lenses, lens cases, and solutions if the patient is a contact lens wearer.
As Figure 2 demonstrates, bacterial conjunctivitis is characterized by redness, papillae, and mucopurulent discharge.


Figure 2
Acute bacterial conjunctivitis
Acute bacterial conjunctivitis can be caused by a number of bacterial species. The most common causes in children are H. influenzae, S. pneumoniae, and Moraxella catarrhalis.11 In adults, Staphylococcal species and Streptococcus pneumoniae are more common, with H. influenzae a potential culprit as well.11 Acute BC is relatively uncommon in adults and is much more likely in children.7
The typical signs and symptoms of acute BC include papillae on the palpebral conjunctiva, a scant to moderate amount of colored discharge, and mild to moderate irritation or pain and photophobia. Patients will often report waking up with their lids “crusted shut” and residual discharge may be noted on the lashes and lid margin as well.
These cases of conjunctivitis are usually self-limiting and resolve within 7-10 days;7 however, treatment with topical antibiotics can speed resolution and help alleviate symptoms.6 There are numerous antibiotics that can be successfully used to treat the condition and many broad-spectrum antibiotics are equally efficacious, so the antibiotic chosen often comes down to the suspected underlying pathogen, medication cost, availability, dosing, and any allergy concerns.
Polytrim (polymyxin B/trimethoprim) dosed QID for 7 days is an excellent option, especially for children, as are fluoroquinolones such as ciprofloxacin 0.3%, ofloxacin 0.3%, and moxifloxacin 0.5%, which have broad coverage and are also dosed QID for 7 days. These antibiotics have good coverage against both gram-positive and gram-negative bacteria, such as Staph and H. influenzae respectively, as well as relatively low dosing frequency which makes them appropriate first-line treatments.
If a significant amount of inflammation is present, a soft steroid, such as loteprednol etabonate 0.5%, dosed BID-QID for 7 days can also be used. Bacitracin or ciprofloxacin 0.3% ointment can also be used QHS as adjunct therapy to increase contact time with the ocular surface. Patients should also wash all bedding and towels and discard any makeup. It is important to note if the patient is a contact lens wearer, they should discontinue contact lens use and dispose of their lenses, lens case, and solution as each may be a potential source of contamination.
These patients should also be treated with a broad-spectrum antibiotic with good gram-negative coverage, ideally a fourth-generation fluoroquinolone, like moxifloxacin 0.5%, as they are at a higher risk of pseudomonas infection, which poses a risk to the cornea including ulceration and perforation if left untreated.19
Many consider steroid use contraindicated in the presence of infection, due to the risk of prolongment and potential worsening of the condition. However, it has been shown that when topical steroids are used for a short duration (2 weeks or less) in the treatment of bacterial conjunctivitis, these concerns are primarily theoretical and topical steroids can be used safely and effectively.20 However, if there is any sign of corneal ulceration or if the patient is a contact lens wearer, topical steroid use should be avoided.
Additionally, most cases of bacterial conjunctivitis are relatively mild, so the use of a steroid will rarely be needed. But if significant chemosis or inflammation is present, and the patient is highly symptomatic, topical steroids can be an effective adjunct therapy.
As seen in Figure 3, he discharge present in bacterial conjunctivitis is often colored rather than clear and can appear creamy-white, yellow-green, or brown


Figure 3
Chronic bacterial conjunctivitis
Chronic bacterial blepharitis is often caused by an overgrowth of normal microflora, such as Staph bacteria. The most common causes of chronic BC are Staphylococcus aureus (and other Staph species), Moraxella lacunata, and enteric bacteria.14 These cases of conjunctivitis persist for 4 weeks or longer.14 Chronic cases may display less discharge than acute cases, but patients will often report persistently red eyes, a gritty or foreign body sensation, and crusting of the lids and lashes (scurf or debris will often be observed), especially upon waking.
A papillary reaction is also usually present. In cases of infections due to Staph bacteria patients frequently describe a burning sensation, often at the corners of the eyes. This may be due to bacterial exotoxins pooling and draining at the puncta, as the Staph bacteria that normally exist on the lids and lashes release exotoxins and waste onto the ocular surface. Cases of Staphylococcal blepharoconjunctivitis are considered noninfectious, as they are caused by the overgrowth of normal microflora (as opposed to the presence of a foreign organism).
Another sign that helps differentiate Staph conjunctivitis from other forms of conjunctivitis is the presence of saponification of the tear film. Staph bacteria produce lipases that break down the lipid layer of the tear film and give the tears a “frothy” or “foamy” appearance.21 These cases have a strong inflammatory component, so the use of a topical antibiotic-steroid combination drop such as TobraDex (dexamethasone 0.1 %/tobramycin 0.3 % ophthalmic suspension) or Zylet (loteprednol etabonate 0.5 %/tobramycin 0.3 % ophthalmic suspension, Bausch & Lomb) dosed QID for 7 days can be an excellent choice. Also, as these cases are noninfectious, the use of a topical steroid is safe in addition to being effective. While the use of a topical combination drop can successfully clear the signs and symptoms of staph blepharitis in the short-term, the condition will also require long-term treatment due to its chronic nature.
The use of hypochlorous acid sprays, such as HyClear (hypochlorous acid 0.01%, Contamac) or Avenova (hypochlorous acid 0.01%, NovaBay Pharmaceuticals) applied twice daily is the treatment of choice in these cases as it directly addresses the underlying cause of staph conjunctivitis. Hypochlorous acid is produced by the leukocytes of the immune system naturally, and it carries antiseptic and anti-inflammatory properties22 and is safe for long-term use. Application of hypochlorous acid to the lids and lashes kills the Staph bacteria present, reducing the bacterial burden, which in turn reduces the amount of exotoxin and lipase released thereby addressing the source of inflammation.
Additionally, performing in-office or at home lid debridement, such as with BlephEx (Alcon) or NuLids (NuSight Medical), respectively, can successfully remove proinflammatory debris and biofilm present in staph blepharoconjunctivitis.23
Figure 4 demonstrates the presence of “foamy” or “frothy tears,” known as saponification, is a sign of chronic blepharoconjunctivitis due to staph bacterial overgrowth.


Figure 4
Phlyctenular keratoconjunctivitis
Phlyctenular keratoconjunctivitis (PKC) is a form of chronic conjunctivitis that is considered noninfectious in nature but is triggered by the response to a bacterial pathogen.16,24 It is thought that PKC is actually a form of Type IV hypersensitivity reaction to the presence of a bacterial antigen, rather than a direct bacterial infection.25
The most common cause of PKC in the U.S. is staphylococcus aureus, however it can also be caused by mycobacterium tuberculosis,16,26 so patients should be questioned about potential exposure to tuberculosis (TB) (such as travel to regions where TB is endemic, stays in homeless shelters or prisons), and signs and symptoms of TB assessed (including chronic cough or significant weight loss).
The condition can also be caused by chlamydia trachomatis and streptococcus viridians.25,27 It has been shown to be associated with ocular rosacea and Staph blepharitis.24,25 PKC primarily affects the pediatric population, with females being more affected than males.16 PKC also tends to be more common in the spring.28,29 The classic sign of PKC is the presence of raised, nodular lesions known as phlyctenules on the conjunctival or corneal surface. These nodular lesions are typically found near the limbus.16 The phlyctenules are prone to ulceration, often pick up stain, and display prominent injection around the lesions.
Ultimately the nodules can migrate onto the corneal surface which can lead to neovascularization and scarring.25 While conjunctival lesions typically only result in mild irritation, corneal phlyctenules often cause significant pain.24
Additionally, mucoid discharge and photophobia are a common sign and symptom of PKC, and it is worth noting that PKC due to TB tends to display more severe photophobia than that caused by staph.24 PKC is typically treated with topical steroids or steroid sparing agents, such as cyclosporine for long-term management, as inflammation is the primary driver of the condition.30 If any ulceration is noted, the concomitant use of a broad-spectrum topical antibiotic is warranted.
Lid hygiene, such as the use of hypochlorous acid, is also beneficial to decrease the number of bacteria present on the lids and lashes. Patients with high suspicion for TB should receive a Mantoux tuberculin skin test, QuantiFERON-gold testing, or chest x-ray to rule out TB as the potential cause of infection. It is also recommended the patient be tested for chlamydia if suspected. Additionally, any concomitant conditions such as ocular rosacea or staph blepharitis should be addressed.
PKC, as seen in Figure 5, displays nodules, known as phlyctenules, that appear on the conjunctiva or cornea but are often found in the limbal region.

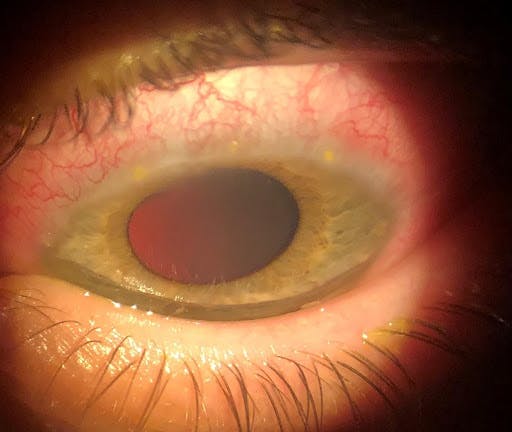
Figure 5
An uncommon form of chronic BC is angular blepharoconjunctivitis. This can be caused by both Staph and Moraxella lacunata and results in a scaly appearance and ulceration of the corners of the eyelid skin near the canthi, usually at the temporal canthus, in addition to conjunctival injection and mild discharge.31 When caused by moraxella, the condition can be difficult to treat and slow to heal.32 Topical fluoroquinolones are the treatment of choice in cases of angular blepharitis, especially ciprofloxacin 0.3% ointment which can be applied directly to the affected areas, providing prolonged contact time and a protective barrier for the irritated skin, which promotes healing.
Hyperacute conjunctivitis (gonococcal conjunctivitis)
Hyperacute conjunctivitis (Gonococcal conjunctivitis) is caused by Neisseria gonorrhoeae or Neisseria meningitidis and requires urgent treatment. It typically incubates over a period of 1-7 days (it remains contagious during this time as well) and then presents with a rapid onset, usually in less than 24 hours, for which it receives its name.33 The pathognomonic sign is copious, purulent milky-white discharge. This heavy discharge is often accompanied by a papillary reaction, significant conjunctival chemosis, corneal infiltrates, and lid edema.
Additionally, the eye will be tender and painful. Neisseria species are capable of perforating intact corneal tissue, and carry a risk for endophthalmitis, making urgent treatment critical.13 It is typically transmitted through sexual contact but can also be passed from infected mothers to newborns during birth which is referred to as gonococcal ophthalmia neonatorum.
Patients experiencing gonococcal conjunctivitis will require intramuscular or intravenous antibiotics depending on the degree of corneal involvement. If no ulceration is present, a patient can receive a single dose of 1 g ceftriaxone on an outpatient basis plus a topical fourth-generation fluoroquinolone, such as moxifloxacin 0.5%, dosed every waking hour until resolution (typically 5-7 days). If corneal ulceration is present, the patient will require hospital admission and should receive 1 g ceftriaxone IV twice a day for 3 days in addition to a topical fourth-generation fluoroquinolone dosed at least every waking hour (with consideration of dosing every hour around the clock for the first 1-3 days or until the ulcer has healed).
In cases of a penicillin allergy, a single dose of 2 g IM spectinomycin can be administered or an oral fluoroquinolone, such as ciprofloxacin 500 mg or ofloxacin 400 mg BID, can be given for 5 days. Patients should be instructed to frequently irrigate their eyes to reduce the bacterial burden on the ocular surface by removing the bacteria-laden discharge. It is also recommended that the patient should be treated prophylactically for chlamydial infection due to a high concomitance between the two conditions.34 The patient should also notify all sexual partners and it is recommended they be screened for other potential sexually transmitted infections (STIs), such as syphilis and HIV, as well.
Adult inclusion conjunctivitis and trachoma (chlamydial conjunctivitis)
Adult inclusion conjunctivitis (AIC) is caused by Chlamydia trachomatis (serotypes D through K).35 It accounts for 1.8 to 5.6% of cases of conjunctivitis6 and is transmitted through sexual contact, with 54% of males and 74% of females displaying concomitant genital infections.36 Chlamydial conjunctivitis is unique among BC cases as it presents more similarly to viral conjunctivitis than other bacterial infections. Both AIC and viral conjunctivitis present with follicles and both can cause preauricular lymphadenopathy and corneal subepithelial infiltrates (SEIs).37 However, AIC tends to produce thicker, colored discharge whereas viral discharge is more serous in nature. Additionally, viral conjunctivitis will resolve on its own within a few weeks whereas AIC will persist.38 The follicular reaction observed in AIC tends to develop on the lower lid. These are often giant follicles and may coexist with papillae creating a mixed reaction.39
Given its similar presentation to viral conjunctivitis, AIC often goes misdiagnosed. Additionally, it does not respond to topical antibiotics due to its underlying systemic etiology, so even when a bacterial cause is suspected standard treatment with topical antibiotics is ineffective. Given the potential difficulty of diagnosing the condition and the fact only 50-75%36 of patients have other systemic signs and symptoms, AIC often leads to chronic conjunctivitis. For this reason, in any case of chronic conjunctivitis or conjunctivitis that does not respond to topical antibiotics, especially in patients in young adulthood and in the presence of a follicular reaction, AIC should be suspected.
While cultures can be performed to confirm the diagnosis, suspected cases can be successfully treated with oral antibiotics. Treatment options include a single dose of 1 g oral azithromycin (however some patients have difficulty tolerating this high dose) or a 7-day course of doxycycline 100 mg BID, tetracycline 250 mg QID, or erythromycin 500 mg QID. Similar to hyperacute conjunctivitis, patients should also contact their sexual partners as they will also need treatment and receive testing for other concomitant STIs as well.
Trachoma is also caused by Chlamydia trachomatis, but it is caused by serotypes A through C.35 Trachoma is rare in the U.S., but it is the leading cause of infectious blindness worldwide.40 It is more common in Northern Africa and the Middle East and affects 40 million people globally.41 Infection is transmitted by flies and spread through poor hygiene conditions as well.42 Like AIC, trachoma leads to a chronic conjunctivitis with a follicular reaction. However, the follicles present in trachoma tend to appear on the upper lid as opposed to the lower lid in AIC.39
Other signs of trachoma include linear scars on the superior palpebral conjunctiva due to chronic inflammation known as Arlt’s Lines, Herbert’s Pits which are depressions in the limbus due to apposition to the superior follicles, and eventually trichiasis due to entropion secondary to the scarring of the lids which can lead to corneal scarring and opacification.39 The treatment regimen for trachoma is referred to by the acronym SAFE, which stands for surgery for advanced/scarring cases, Antibiotics for active infection (the same as those used to treat AIC), facial cleanliness, and environmental hygiene practices.43
Figure 6 demonstrates chronic follicular or mixed follicular-papillary reaction in the presence of mucoid discharge is a sign of chlamydial conjunctivitis.


Figure 6
Parinaud oculoglandular syndrome
Parinaud oculoglandular syndrome (POGS) is a zoonotic form of granulomatous follicular conjunctivitis that occurs along with lymphadenopathy.44 The most common cause of POGS is the bacterium Bartonella henselae, which is associated with cat scratch disease. Francisella tularensis (tularemia) and Sporothrix schenckii (sporotrichosis) are two other potential causative bacteria.44 An estimated 5-7% of patients with cat scratch disease develop POGS.45,46 Bartonella henselae is excreted by fleas of which cats can be a carrier. When flea feces is transmitted to humans through an open wound (such as a cat scratch, for which the condition is named) or directly to the ocular surface via contaminated fingers, infection can occur.
After inoculation, the disease incubates for 3 to 21 days before developing into a follicular conjunctivitis.47 POGS conjunctivitis can also mimic viral conjunctivitis as it produces a follicular reaction, mild lid edema, and often watery discharge, however POGS conjunctivitis exhibits an identifying conjunctival nodule or granuloma that is the hallmark sign of the condition.48 POGS also causes lymphadenopathy that can result in swelling of lymph nodes at several sites. Patients may also experience a mild fever.47
POGS often self-resolves without treatment, however it can take weeks to months for the granuloma and lymphadenopathy to clear.49 Therefore, treatment involves supportive therapies including artificial tears and cool compresses. The nodular lesion can also ulcerate, so topical antibiotics can be used prophylactically in these cases to prevent any superinfection.
Rocky Mountain spotted fever
Rocky Mountain spotted fever (RMSF) is a zoonotic disease caused by the bacterium Rickettsia and is spread via tick bite. RMSF is more common in the spring and summer months when ticks are more active.50,51 It is most common in the west south-central region of the United States for which it received its name,52 There are an estimated 500-2,500 documented cases yearly in the U.S.53 RMSF is identified by a fever accompanied by its distinctive maculopapular rash that can develop over most of the body. Conjunctivitis develops later in the disease course and tends to create a petechial conjunctivitis with small pinpoint bleeds that sets it apart from other forms of conjunctivitis.54
RSMF can also affect other parts of the eye resulting in uveitis, chorioretinitis, and optic neuropathy.55 RMSF can be potentially fatal due to its ability to affect multiple organ systems and the central nervous system.52 The standard treatment for RSMF is doxycycline 100 mg BID for 7-10 days. Treatment is usually discontinued 48 hours after the patient’s fever has resolved.55
If a patient presents with a body rash, as seen in Figure 7, in addition to conjunctivitis, it is important to consider tick-borne infections, such as RMSF, especially if they have a history of outdoor activities such as hiking or hunting.


Figure 7
Lyme disease
Lyme disease is another zoonotic tick-borne infectious disease that can result in conjunctivitis. Hunters, hikers, and those who spend time outdoors have a higher risk due to increased tick exposure, and outbreaks tend to occur in the spring through the fall.56 The condition is more common in the Northeast U.S. and Upper Midwest.57 There are an estimated 30,000 cases of Lyme Disease per year in the U.S., but new research suggests it may be as high as 300,000.58,59
Lyme Disease is caused by the bacterium Borrelia burgdorferi. Lyme Disease causes a follicular conjunctivitis in about 10% of cases.60 If left untreated the condition can affect nearly every part of the eye resulting in uveitis, chorioretinitis, and optic neuropathy.60 The pathognomonic sign of Lyme Disease is a rash that develops in a “bull’s eye” pattern at the site of infection, however in 20-30% of cases this rash does not develop making diagnosis difficult61. While the rash self-resolves over several weeks, if left untreated the disease can become chronic and affect numerous parts of the body and organ systems including the heart, joints, and central nervous system.62,63
The condition can be diagnosed through laboratory testing including an ELISA or Western Blot.64 Oral antibiotics are the first-line of treatment for Lyme Disease. Doxycycline 100 mg dosed BID for 10-21 days is typically the standard treatment, however amoxicillin 500 mg (25-50 mg/kg per day for children) TID or cefuroxime 500 mg (30 mg/kg per day for children) taken for 14-21 days can also be used.
Make sure to download the Differential Diagnosis Flowcharts!
Overview
Viral conjunctivitis (VC) is the most common form of conjunctivitis, accounting for almost 80% of all acute cases,65,66 and is the most common cause of conjunctivitis in adults.6 Of these viral cases, 65-90% are due to adenoviruses.66 Other pathogens include the herpes viruses. VC tends to occur more during the summer months7 and has an incubation period of 5-12 days.38 VC presents with a follicular reaction on the palpebral conjunctiva and clear, watery discharge. Viral cases may also include corneal infiltrates and some patients will report itching. In severe cases, patients may also develop membranes or pseudomembranes and 50% of patients will display swollen lymph nodes.66
Viral conjunctivitis is highly contagious with a transmissibility risk of 10-50%7,67 and remains communicable for 10-14 days.68 VC can be contracted through contact with a contaminated surface or object or by transmitting the virus to the eyes with contaminated fingers. Sharing towels, bedding, or makeup can also act as routes of inoculation. Similar to bacterial conjunctivitis, contact lens wear also poses an increased risk as handling lenses with contaminated fingers or contamination of the lens case can be potential sources of infection.
It is common to encounter VC in patients who work in schools, daycares, or gyms where there is ample opportunity to contact contaminated surfaces or contagious individuals.
Most cases of VC are self-limiting and resolve without treatment, however some forms of VC, like epidemic keratoconjunctivitis and herpetic conjunctivitis, benefit greatly from treatment as they pose risks such as conjunctival and corneal scarring. While there is no definitive or consensus treatment for VC (other than for herpetic infections), there are several effective options to alleviate symptoms and potentially shorten the course of the condition. Palliative treatments include artificial tears, cold compresses, and topical antihistamines to relieve itching if present. However, povidone-iodine and topical steroids can be effective treatments in managing even severe cases of VC.
Figure 8 illustrates the typical presentation of viral conjunctivitis, which includes a “pink” eye with clear, watery discharge and palpebral follicles.


Figure 8
Adenoviral conjunctivitis is the most common form of viral conjunctivitis, comprising 65-90% of cases of VC.66 There are numerous serotypes of adenoviral conjunctivitis, with the specific serotype of the infective agent determining its severity.69 Serotypes 1 and 11 are common forms of VC that are confined primarily to the eye and produce a mild follicular conjunctivitis.70 Adenoviral conjunctivitis typically presents with conjunctival injection (normally not quite as red as a bacterial infection, giving it more of a “pink” appearance), palpebral follicles, watery discharge, mild irritation, and light sensitivity. Patients may also experience conjunctival chemosis and pruritus as well.
It is common for affected patients to have recently experienced a mild cold or upper respiratory infection and will often have swollen preauricular lymph nodes. While adenoviral conjunctivitis is self-limiting, patients can be treated with artificial tears or cold compresses to increase comfort, and topical antihistamines can address itching if present. Additionally, topical steroids can be helpful in reducing inflammation.
While topical steroids may theoretically prolong the course of the infection,71,72 this does not appear to be a major concern in practice,73 so their use can be especially helpful in relieving symptoms. While not commercially available, a highly effective treatment is a compounded topical solution of povidone-iodine 0.4% or 0.6% and dexamethasone 0.1%.74,75 Povidone-iodine has broad antimicrobial activity and can effectively neutralize viral particles on the ocular surface.76
Therefore, by combining the antimicrobial properties of povidone-iodine with the anti-inflammatory properties of a steroid, the combination treatment can alleviate symptoms while also potentially shortening the course of infection as well as the transmissibility period through reduction of the viral load on the ocular surface.74,75 Povidone-iodine-dexamethasone can be dosed QID for 7 days and can then be used TID for an additional 3 days if needed, but dosing should not exceed 10 days as prolonged povidone-iodine use can be irritating to the ocular surface.
It is also critical that affected patients wash all towels and bedding, discard any makeup, and replace contact lenses, lens cases and solutions if the patient is a contact lens wearer. Patients should also remain home from work or school and avoid close physical contact with others as adenoviral conjunctivitis is highly contagious.
Figure 9 shows pronounced follicles in a case of viral conjunctivitis.

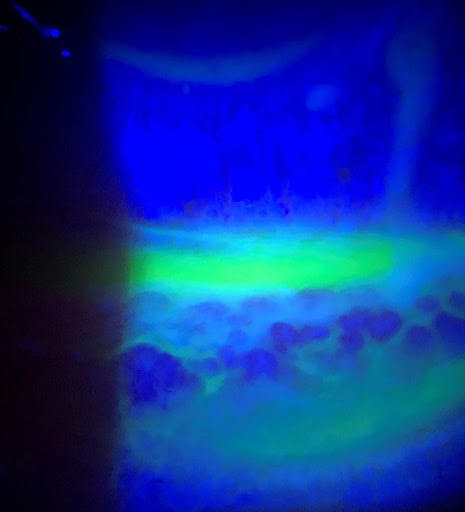
Figure 9
Epidemic keratoconjunctivitis
Epidemic keratoconjunctivitis (EKC) is a severe form of adenoviral conjunctivitis marked by the presence of significant inflammation leading to the development of membranes (sheets of inflammatory material that bleed when removed) and pseudomembranes (which do not bleed upon removal).77 It is caused by adenoviral serotypes 8, 19, and 37.68
EKC tends to cause SEIs that can persist for weeks to months after the infection resolves in addition to the follicular reaction and preauricular lymphadenopathy observed in other adenoviral infections.78,79 While other forms of viral conjunctivitis tend to self-resolve without issue, EKC should be actively treated as the rampant inflammation and membranes present can cause scarring, including symblepharon formation, if left unchecked.78 If membranes or pseudomembranes are present, they should be removed with forceps or a cotton swab to prevent scar formation.
Beyond membrane removal, the treatment of choice for EKC involves the off-label use of a Betadine (povidone-iodine 5% ophthalmic solution, Alcon Laboratories) wash with adjunct topical steroid support. The broad antimicrobial activity of the povidone-iodine neutralizes the virus present on the ocular surface and reduces the viral load which greatly decreases any further inflammation and reduces transmissibility.76 However, this treatment is significantly irritating, so it is crucial to inform patients ahead of time that their eyes will be uncomfortable for the initial period after the treatment.
The treatment itself involves instilling a drop of anesthetic into each eye prior to adding several drops of Betadine to the eye. The patient should then be instructed to close their eyes and roll them around for 1-2 minutes and the lids and lashes can be swabbed with a Betadine-soaked cotton swab to neutralize any viral particles on these surfaces, after which time the eyes should be thoroughly rinsed with sterile saline to remove as much Betadine as possible to reduce further post-treatment irritation.72 A soft steroid such as loteprednol etabonate 0.5% dosed QID for 1 week is an appropriate supportive treatment.
While initially uncomfortable, this treatment rapidly improves the condition which if left untreated can persist for weeks. If SEIs are present they often require a slow steroid taper as they can take several weeks to months, and even years, to completely resolve.78,79 These SEIs can be visually significant,80,67 so treatment can be tailored to their severity.
EKC is especially contagious, so patients should be instructed to wash all towels and bedding, dispose of makeup, discard contact lenses, lens cases and solution if applicable, and avoid physical contact with others until the condition has resolved.
Subepithelial infiltrates (SEIs), as seen in Figure 10, can occur in cases of viral conjunctivitis, especially EKC. These infiltrates can last from weeks to years and may impact vision.

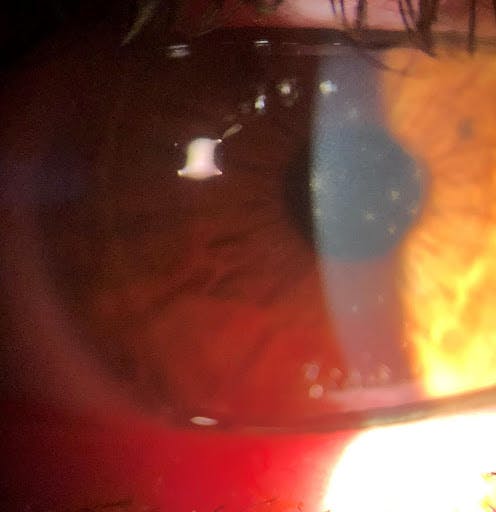
Figure 10
Figure 11 demonstrates membrane formation in a case of EKC. Any membranes or pseudomembranes should be removed as they can result in scarring and symblepharon formation if left untreated.

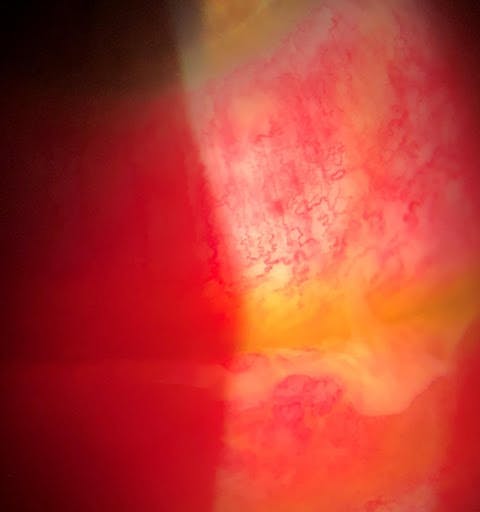
Figure 11
Pharyngoconjunctival fever
Pharyngoconjunctival fever (PCF) is another form of adenoviral conjunctivitis that presents with the same follicular reaction and watery discharge as other forms of VC but is characterized by its associated fever and sore throat.81 It is caused by HAdV types 3, 4, and 7.68 PCF can also cause preauricular lymphadenopathy, and SEIs in some cases. Another unique feature of PCF is a propensity for subconjunctival hemorrhages.82 It has also been associated with swimming pool use.83 PCF is treated in the same manner as other forms of adenoviral conjunctivitis, with the use of artificial tears, cold compresses, topical steroids, or steroid-povidone-iodine combination drops, and hygiene.
Herpes virus conjunctivitis
Herpes simplex virus (HSV) conjunctivitis accounts for an estimated 1-5% of cases of acute conjunctivitis.84-87 It is usually caused by HSV-1, which affects a large proportion of the population as an estimated 67% of people under the age of 50 carry HSV-1.88 Primary HSV infection typically results in a follicular conjunctivitis and rarely affects the cornea.89 HSV-1 is also responsible for cold sores and often spreads from the skin or nasal mucosa to the sensory nerves and remains dormant in the trigeminal ganglion of Cranial Nerve V after the primary infection has occurred.
Whenever patients experience a suppressed immune system, often due to illness or stress, the virus can reactivate and travel along the ophthalmic branch of the trigeminal nerve to the nasociliary nerve and then on to the terminal ends of the corneal nerves where it can result in dendritic corneal lesions pathognomonic to HSV.90
HSV-2, which is associated with genital herpes, can also cause HSV conjunctivitis, but this is less common.89 HSV conjunctivitis is usually unilateral and is associated with a moderate to significant pain that is often described as a stabbing sensation, follicles, redness, photophobia, lid edema, and minimal watery discharge. The hallmark sign of a reactivated HSV infection is the presence of corneal dendrites, which are branching ulcerative lesions that have terminal end bulbs and stain with fluorescein.89 Vesicular lesions may also be noted on the lids of patients with HSV conjunctivitis.89
Herpes zoster virus (HZV) conjunctivitis is associated with Herpes Zoster Ophthalmicus (HZO). The HZV virus is the same virus responsible for chickenpox and shingles and affects 10-20% of the population.91 HZO refers to HZV infection of the ophthalmic branch of the trigeminal nerve, in which the eye itself is affected in 50% of cases.92 Like HSV, it remains dormant in a sensory ganglion after primary infection, including the trigeminal ganglion, and can reactivate in periods of immunosuppression in patients with a previous history of chickenpox or shingles.92
HSV conjunctivitis presents unilaterally and is associated with a painful rash that follows the dermatome and is usually preceded by a prodromal tingling sensation of the skin.92 If the rash occurs on the eyelids or the tip of the nose (known as Hutchinson's sign), in 85% of cases the eye proper will also be affected.93 When ocular involvement occurs patients usually experience redness, pain, and photophobia.
Eyelid edema is also common in HZO, especially if the rash has spread to the lids. If a palpebral reaction occurs, it is follicular in nature.94 The cornea will also display branching lesions similar to HSV, however these lesions are raised rather than ulcerated, so they will not pick up stain or only stain lightly, and these lesions also lack terminal end bulbs, so they are referred to as pseudodendrites.92
The treatments for HSV and HZV share some similarities but also some critical differences. While the first-line therapy for both is oral antivirals, the difference relates to the use of topical treatments. While topical antivirals such as Zirgan (ganciclovir 0.15% ophthalmic gel, Bausch & Lomb) are helpful in cases of HSV, they are not indicated for use in cases of HZV. However, there is evidence that off-label use of Zirgan can be helpful in managing HZV. The greatest difference in treatment exists in the use of topical steroids.
Topical steroids should be avoided in cases of HSV with active dendrites as this can worsen the condition and lead to the development of a geographic ulcer.90 However, topical steroids are a mainstay treatment of HZV. It is also critical to initiate treatment of HZV within 72 hours to reduce the likelihood of post-herpetic neuralgia.95
There are several options for oral antiviral treatment for HZV including: acyclovir 800 mg 5 times per day, valacyclovir 1000 mg TID, and famciclovir 500 mg TID each used for 7 days. The same antivirals can be used to treat HSV, but the doses are halved (acyclovir 400 mg 5 times per day, valacyclovir 500 mg TID, and famciclovir 250 mg TID each used for 7 days).
Valacyclovir is an excellent treatment of choice as it is relatively inexpensive and has a lower dosing frequency compared to acyclovir. If topical antivirals are used, Zirgan is dosed 5 times per day until the cornea is re-epithelialized and then TID for 7 days. If Viroptic (trifluridine 1 % ophthalmic solution, Pfizer) is used, it is dosed every 2 hours with maximum dosing of nine times per day until the cornea is re-epithelialized, and then 5 times per day for 7 days. Viroptic should not be dosed longer than 21 days as it has significant surface toxicity and can induce substantial surface disruption and irritation.96
It is worth noting that while topical antivirals can be effective treatments, their use is often not necessary to treat HSV as oral antivirals alone can manage the condition (however they may require dosing beyond the initial 7-day period). This is a relevant point as Zirgan, although very effective, can be difficult to acquire and can be prohibitively expensive for some patients, and the surface toxicity associated with Viroptic makes its use less than ideal.
COVID conjunctivitis
COVID conjunctivitis is caused by the SARS-CoV-2 virus.97 Conjunctivitis caused by the coronavirus presents with a follicular reaction, redness, and watery discharge like other viral forms of conjunctivitis. Additionally, in late stages of the infection patients can develop SEIs as well.98 COVID can be spread to the ocular surface directly as viral particles can infect mucus membranes such as the conjunctiva. Conjunctivitis is the most common ocular manifestation of COVID and may be the primary sign of infection or occur alongside other symptoms.98 Conjunctivitis has been shown to occur in about 1 in 10 patients hospitalized for the infection99 and 1-6% of COVID patients overall.100
Given the current state of the COVID pandemic, all patients presenting with conjunctivitis, especially those appearing viral in nature, should have COVID as a differential diagnosis. Patients displaying signs and symptoms of viral conjunctivitis should have their temperatures taken and recorded and be asked if they have recently been in contact with infected individuals or those who may be affected. They should also be screened for constitutional symptoms including fatigue, alteration to sensation of taste or smell, or other flu-like symptoms. If they answer yes to any of these questions, display any of these symptoms, or the exact etiology of their conjunctivitis remains uncertain, the patient should be tested for COVID.
Additionally, even if they answer no to all screening questions, testing is still strongly encouraged as conjunctivitis can be the sole presenting sign of COVID infection.101 Individuals found to be infected should follow quarantine guidelines, which is typically recommended for 14 days102, or seek emergency medical attention if other serious symptoms, such as difficulty breathing, occur.103
Fungal conjunctivitis
Fungal conjunctivitis
Fungal forms of conjunctivitis are rare, and when they occur it is usually in conjunction with fungal keratitis. Fungal keratitis is most frequently associated with contact lens misuse or trauma with organic matter, as 40% of cases involve trauma.104-106 It is more common in warm, humid climates.107 Different fungal species can cause fungal keratoconjunctivitis, but the most common are Fusarium (67%), Aspergillus (10.5%), and Candida (10%).106 Fungal infections are more likely in immunocompromised individuals.104,105 Fusarium infections are often associated with contact lens wear, including a notable outbreak linked to contact lens solution-related contamination in 2005-2006.108
The conjunctivitis elements of fungal infection are the same redness, irritation, chemosis, follicles, and mucoid discharge seen in other types of conjunctivitis. The differentiating factor is the form of corneal lesions that accompany the conjunctivitis. Fungal infections produce characteristic ulcers with feathery borders and multiple smaller satellite lesions.107
Additionally, there is usually development of a significant anterior chamber reaction including hypopyon formation. Initially, fungal ulcers can be difficult to differentiate from bacterial ulcers, so a nonresponse to antibiotic treatment is a red flag that the infection may be fungal in nature. Fungal keratoconjunctivitis is notoriously difficult to treat and the treatments involved carry significant side-effects.
Natacyn (natamycin 5% suspension, Eyevance Pharmaceuticals) is the only FDA-approved topical ophthalmic treatment available and is dosed once every hour around the clock for 3-4 days, then 6-8 times per day and slowly tapered for up to 8 weeks. Amphotericin B can also be used, but there is no commercial preparation available, so it must be compounded, typically as a 0.15% dilution. Oral antifungals are used as adjunct therapies, such as voriconazole 400 mg BID until two weeks after resolution. Voriconazole can also be compounded as a 1% dilution for topical use.
Parasitic conjunctivitis
Demodex blepharokeratoconjunctivitis
Demodex blepharokeratoconjunctivitis is caused by the ectoparasitic mites demodex folliculorum and demodex brevis that live in hair follicles and sebaceous glands, respectively.109 Demodex are normal microfauna found on the skin, but if there is an overpopulation of the mites it can elicit an inflammatory response resulting in conjunctivitis, blepharitis, and meibomian gland dysfunction.110 Demodex blepharokeratoconjunctivitis exhibits similar nonspecific signs and symptoms shared by all forms of conjunctivitis including redness, irritation, and tearing.
The key finding that signals the presence of a potential demodex over-infestation is sleeve-like collarettes at the base of the eyelashes.111 While there is no FDA-approved treatment for demodex, 50% tea tree oil (TTO) has been shown to be effective at reducing the number of mites present. There are multiple forms of TTO available such as lid scrubs and facial washes, all of which can be used effectively. Regardless of the form of TTO used, it is recommended that the product be used BID for at least 6 weeks as this will ensure treatment through two life cycles of the mites.109 It can then be used prophylactically with daily use. Another potential treatment that is currently under investigation is lotilaner 0.25% ophthalmic solution, which would be the first FDA-approved treatment for demodex.112
As seen in Figure 12, sleeve-like collarettes at the base of the eyelashes are a sign of Demodex infestation that can lead to blepharoconjunctivitis.

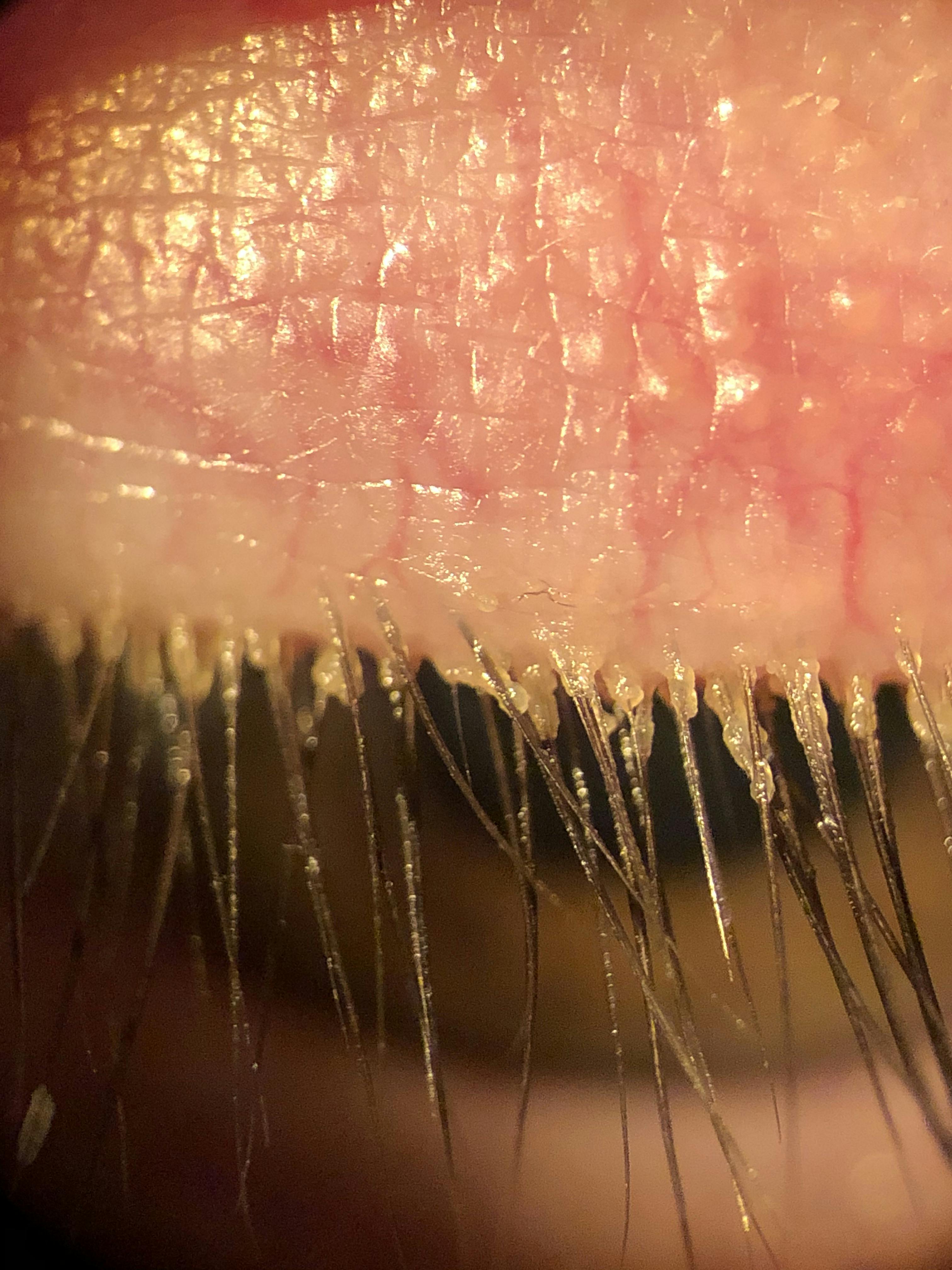
Figure 12
Acanthamoeba
Acanthamoeba keratitis is a condition caused by a parasitic infection that can also result in conjunctivitis. Acanthamoeba is a free-living parasitic amoeba that lives in water including lakes, pools, hot tubs, tap water, and contaminated contact lens solution.113 Infections are routinely associated with contact lens wearers (80% of cases)114 who are exposed to a water source containing the amoeba. For this reason, it is critical for contact lens wearers to never rinse or store their lenses in tap water or “top off” solution and are advised to avoid swimming or showering in their lenses to decrease the risk of infection.
Corneal trauma is another potential risk factor. AK infections start out with a mild conjunctivitis involving redness,115 irritation or foreign body sensation, chemosis, and photophobia as well as other nonspecific signs like corneal epithelial irregularity.116 The hallmark sign of AK that sets it apart from other infections is its propensity to cause pain (often described as being a “10/10”) out of proportion to its signs, which suggest perhaps a mild conjunctivitis.117
As the infection progresses, corneal infiltrates begin to develop that can resemble pseudodendrites.118 If left untreated, the infiltrates will coalesce into a perineural ring infiltrate that will ultimately form a characteristic ring ulcer that can cause permanent scarring and opacification.118
The proclivity for the infection to develop around the nerves is thought to be a potential source of the intense pain experienced by these patients. An anterior chamber reaction with hypopyon often occurs as well. Cultures should be taken if AK is suspected, and confocal microscopy or PCR testing can also be used to confirm the diagnosis.118
Early treatment is crucial for AK, but unfortunately diagnosis is difficult and often not made until nonresponse to other treatments, such as antibiotics or hallmark signs, such as a ring infiltrate develop, by which time the infection has already taken a firm hold. Acanthamoeba infections are infamously difficult to treat due to the pathogen’s anatomy and life cycle. The amoeba exists in both an active trophozoite and dormant cyst form that has an incredibly durable double wall structure that can resist high heat, freezing, and even irradiation.119 Therefore, treatment for AK and any associated conjunctivitis is highly involved and prognosis is poorer than for other infections.
There is no specific treatment indicated for AK, so a mix of antiparasitic, antifungal, antibiotic and antiviral medications are used. Many of the treatments are not commercially available making obtaining them difficult. A compounded form of swimming pool disinfectant, PHMB (polyhexamethylene 0.02% biguanide), is used in conjunction with Brolene (propamidine 0.1%) with each drop being administered hourly and staggered by 30 minutes. Chlorhexidine can be substituted for PHMB if not readily available. Oral voriconazole and topical neomycin-polymyxin B-gramicidin can be used as adjunct therapies. Treatment often lasts 6-12 months due to the difficulty in killing the cystic forms of the amoeba.
A lesser used off-label treatment involves the use of Impavido(miltefosine), an oral antiparasitic indicated for the treatment of leishmaniasis. The potential benefit of Impavido is it carries significant cysticidal activity,120 which is the most challenging aspect of managing the condition. Its use for AK involves dosing the medication at 50 mg BID (for patients 30–44 kg) or TID (for patients >45 kg) for 2 months.121 Due to the difficulty involved in treating the condition, many patients ultimately require a corneal transplant.
Onchocerciasis
Onchocerciasis, also known as River Blindness, is caused by the parasitic nematode Onchocerca volvulus. Onchocerciasis starts as a systemic infection that can develop ocular manifestations including chronic conjunctivitis and can ultimately result in blindness. A key sign of onchocerciasis is the presence of subcutaneous nodules.122 Though rare in the U.S., it is the second leading cause of infectious blindness worldwide affecting 18-37 million people and is most common in African and Latin American countries.123
The nematode is transmitted exclusively by the Simulium black fly which is found near fast moving bodies of water such as rivers and streams.124 A bite from the fly transmits the larval form of the nematode into its human host where it then develops into a mature form over 6-12 months.125 Female nematodes form fibrous capsules in the facial tissue where males migrate to fertilize the females, forming the subcutaneous nodules that are pathognomonic for onchocerciasis.125 The fertilization of the female nematodes results in millions of microfilariae forms of the parasite that spread throughout the body including the eye.125
These microfilariae can be visualized behind the slit lamp and look like motile S- or C-shaped elements moving in the cornea or anterior chamber.126,127 The first signs of ocular infection are typically a chronic conjunctivitis displaying redness, chemosis, and corneal lesions along with eyelid nodules.128 The infection then can spread to any ocular tissue and cause uveitis, glaucoma, optic neuropathy, and chorioretinitis.128,129 The ocular manifestations associated with Onchocerciasis usually appear years after initial infection.130,131
While the diagnosis of Onchocerciasis can be made definitively with laboratory testing including an ELISA or Western Blot, the diagnosis can be made clinically with the presence of subcutaneous nodules and the visualization of nematodes in the cornea or anterior chamber.132,133 Onchocerciasis is treated with the antiparasitic drug ivermectin 150 µg/kg dosed once every 6-12 months over a 10-year period.132 In areas where the condition is endemic, ivermectin is often administered prophylactically.134
Noninfectious conjunctivitis
Keratoconjunctivitis sicca (dry eye disease)
Keratoconjunctivitis Sicca, commonly referred to as dry eye, is a chronic condition that can affect the entire ocular surface. It is estimated that up to 34% of the population suffers from dry eye disease (DED).135 Dry eye is a multifactorial disease that ultimately relates to a disruption of homeostasis of the ocular surface and tear film.136 DED presents with several nonspecific signs and symptoms including redness, irritation (foreign body sensation, burning, stinging), and blurred or fluctuating vision.
Unlike other forms of conjunctivitis there is usually no marked palpebral reaction (though some cases may exhibit mild papillae) and there is no discharge present, although some dry eye patients may experience epiphora.
The most common cause of DED is dysfunction of the tear film, and the most common driver of this dysfunction is meibomian gland dysfunction (MGD) which is present in 86% of all cases of dry eye.137 MGD leads to disruption of the outer lipid layer of the tear film which causes breakdown of the underlying tear structure as the lipid layer acts as a protective barrier.
Sjogren’s Syndrome is another condition that leads to dry eye. While Sjogren’s Syndrome is estimated to affect 1-4 million people in the U.S.,138 it is less frequently observed and even in Sjogren’s related DED cases MGD usually occurs concomitantly. There are myriad dry eye treatments available, but the primary goal of treatment is targeting the underlying causes of tear film dysfunction.
Foundational treatments often include artificial tears (a preservative free, lipid-based tear such as Refresh Optive Mega-3 (Allergan)is recommended) for comfort, omega 3 supplementation to support quality meibum production, lid hygiene (such as hypochlorous acid to address any Staph blepharitis component), and blink exercises to encourage proper blinking mechanics. Anti-inflammatory drops that are safe for long-term use, such as Xiidra (lifitegrast 5% ophthalmic solution, Novartis), Cequa (cyclosporine 0.09% ophthalmic solution, Sun Pharmaceuticals), or Restasis (cyclosporine 0.05% ophthalmic emulsion, Allergan) can be used BID in cases where inflammation is a major contributing factor.
Additionally, in-office treatments such as Intense Pulsed Light (IPL) and thermal pulsation, including LipiFlow (Johnson & Johnson) or iLux (Alcon), are effective treatments that address multiple underlying mechanisms of DED.
Rosacea conjunctivitis
Rosacea conjunctivitis is a form of ocular rosacea, which is a subtype of rosacea that affects the eyelids and ocular surface.139 Rosacea is an inflammatory condition due to hypersensitivity to normal environmental stimuli, such as cold weather or spicy food, that results in the abnormal development of telangiectatic blood vessels that are prone to flushing and inflammation.140-143 Rosacea affects up to 5% of the population,144 and 58-72% of rosacea patients also have ocular rosacea.145,146
Ocular rosacea (OR) is characterized by telangiectatic blood vessels on the eyelids and eyelid margin with concomitant blepharitis and MGD present in most cases. These abnormal vessels can also develop on the conjunctiva resulting in severely injected eyes, along with photophobia, watery discharge, and irritation often described as a burning sensation. OR is chronic, unlike most infectious forms of conjunctivitis which are usually self-limiting. Rosacea conjunctivitis is also characterized by flares associated with certain triggers like alcohol consumption or emotional stress.
The treatment for rosacea conjunctivitis is multifaceted and usually involves avoiding triggering stimuli, an oral antibiotic such as doxycycline (dosed 50-100 mg QD-BID for 1-3 months), short courses of steroids including loteprednol etabonate 0.5% (dosed BID-QID for 1-2 weeks), long-term inflammation management with Xiidra or Cequa (dosed BID), lid hygiene (hypochlorous acid used BID or TTO applied daily), and supportive therapies for concomitant MGD such as Omega 3 supplementation. Additionally in office procedures such as IPL and thermal pulsation treatment can be utilized to treat the condition.
OR is characterized by the development of lid margin telangiectasia as visible in Figure 13.


Figure 13
Contact lens-associated red eye
Contact Lens-Associated Red Eye (CLARE) is a catch-all term for noninfectious, inflammatory keratoconjunctivitis associated with contact lens wear. CLARE presents with diffuse redness, usually more pronounced in the limbal region, a papillary reaction, and mild to moderate irritation and photophobia, which can be significant.147 It is also common to observe noninfectious corneal infiltrates in the periphery and midperiphery.148,149 CLARE can be unilateral or bilateral, and these symptoms improve with contact lens removal and worsen with contact lens wear.150
While the ultimate underlying cause of CLARE is unknown, the condition is associated with sleeping in lenses and lens overwear.148,151 It is thought the condition is caused by the release of endotoxins by gram-negative bacteria that colonize the lens surface including H. influenzae and Pseudomonas resulting in inflammation.152 It is also believed that ill-fitting tight lenses are a contributing factor as they can induce hypoxia.151 CLARE most commonly occurs with extended wear hydrogel contact lenses which have lower oxygen permeability, as 34% of extended hydrogel wearers experience CLARE, and it occurs rarely with extended silicone hydrogel lens use (only 1% of silicone hydrogel wearers).153-155
The treatment of CLARE involves managing any inflammation present and addressing the underlying cause. A topical antibiotic-steroid combination, such as Zylet or TobraDex dosed QID for 1 week is a standard treatment. Separate topical broad-spectrum antibiotics, like moxifloxacin 0.5%, and topical steroids, such as loteprednol etabonate 0.5% or prednisolone acetate 1%, each dosed QID for 1 week can also be utilized. Patients should discontinue contact lens wear during the course of treatment and should be refit into a lens of a different material and modality to address the underlying cause. This refitting is critical, as an estimated 50-70% of CLARE patients experience a recurrence of the condition if they resume extended hydrogel wear.156
Switching to a daily disposable silicone hydrogel lens is the option of choice for these patients as this addresses both hypoxia and bacterial endotoxin production. Silicone hydrogels have greater oxygen transmissibility thereby reducing hypoxic stress and daily replacement of the lenses reduces bacterial colonization of the lens surface.
Giant papillary conjunctivitis
Giant papillary conjunctivitis (GPC) presents with its namesake giant papillae similar to the papillary reaction observed in forms of allergic conjunctivitis. However, even though it has a similar presentation and often is categorized as an allergic reaction, it is not a true allergy.157,158 The underlying cause of GPC is mechanical trauma due to friction between the upper lid and deposits on the contact lens surface or the lens edge157,159. This friction results in the development of giant papillae on the palpebral conjunctiva of the superior lid. Therefore, it is more accurately described by its lesser used name of contact lens-induced papillary conjunctivitis (CLPC). Any contact lens or contact lens material can result in development of GPC160.
While GPC displays a papillary reaction, redness, foreign body sensation, and ropey discharge like allergic conjunctivitis, it lacks the itching that is the hallmark sign of true allergic cases. Also, the papillae present in GPC tend to be smaller (~0.3mm) than those observed in vernal keratoconjunctivitis and atopic keratoconjunctivitis (larger than 1 mm).157
Therefore, the presence of giant papillae and the absence of itching in a contact lens wearer suggests a diagnosis of GPC. The treatment of GPC involves resolving the underlying mechanical issue. This typically entails switching lens brands, materials, or wearing schedules. Daily disposable lenses are often the best choice for patients with GPC as replacing lenses daily reduces the number of deposits on the lens surface and degradation of the lens itself.
Additionally, a course of topical steroids, such as loteprednol etabonate 0.5% QID for 1-2 weeks along with a contact lens “wash out” period, where the patient temporarily discontinues lens wear, are helpful in resolving the disorder. However, GPC is a chronic condition, and it may take a significant length of time for the papillae to resolve. In persistent cases, a stronger steroid with a longer taper, such as prednisolone acetate 1% dosed QID and then tapered over 4 weeks may be required to get the condition under control.
Figure 14 illustrates how GPC develops when friction occurs between the superior palpebral conjunctiva and deposits on the surface of a contact lens or the lens edge.


Figure 14
Superior limbic keratoconjunctivitis
Superior limbic keratoconjunctivitis (SLK) is a relatively rare condition that causes localized inflammation and conjunctivitis on the superior aspect of the conjunctiva, limbus, and cornea. It affects women more than men and typically occurs in the sixth decade of life.161 SLK is characterized by a sectoral wedge-like region of injection on the superior bulbar conjunctiva, micro-papillae, superior limbal thickening, superior filaments, and pronounced superior ciliary injection.161 The conjunctiva in this area tends to be loose and redundant and picks up stain, as does the thickened limbal tissue. These findings support the proposed underlying mechanism of the condition stemming from mechanical friction between the loose conjunctiva and the superior lid.162
Symptoms include foreign body or burning sensation, and in some cases itching.163 Dry eye is a common comorbidity,163 and it is also recommended that all patients diagnosed with SLK have thyroid function evaluated as nearly 30% of SLK patients have thyroid dysfunction.164-166 SLK tends to have a relapsing-remitting pattern and some cases self-resolve with age while others remain persistent.167
In Figure 15, SLK exhibits as a sectoral, wedge-like area of injection on the superior bulbar conjunctiva.

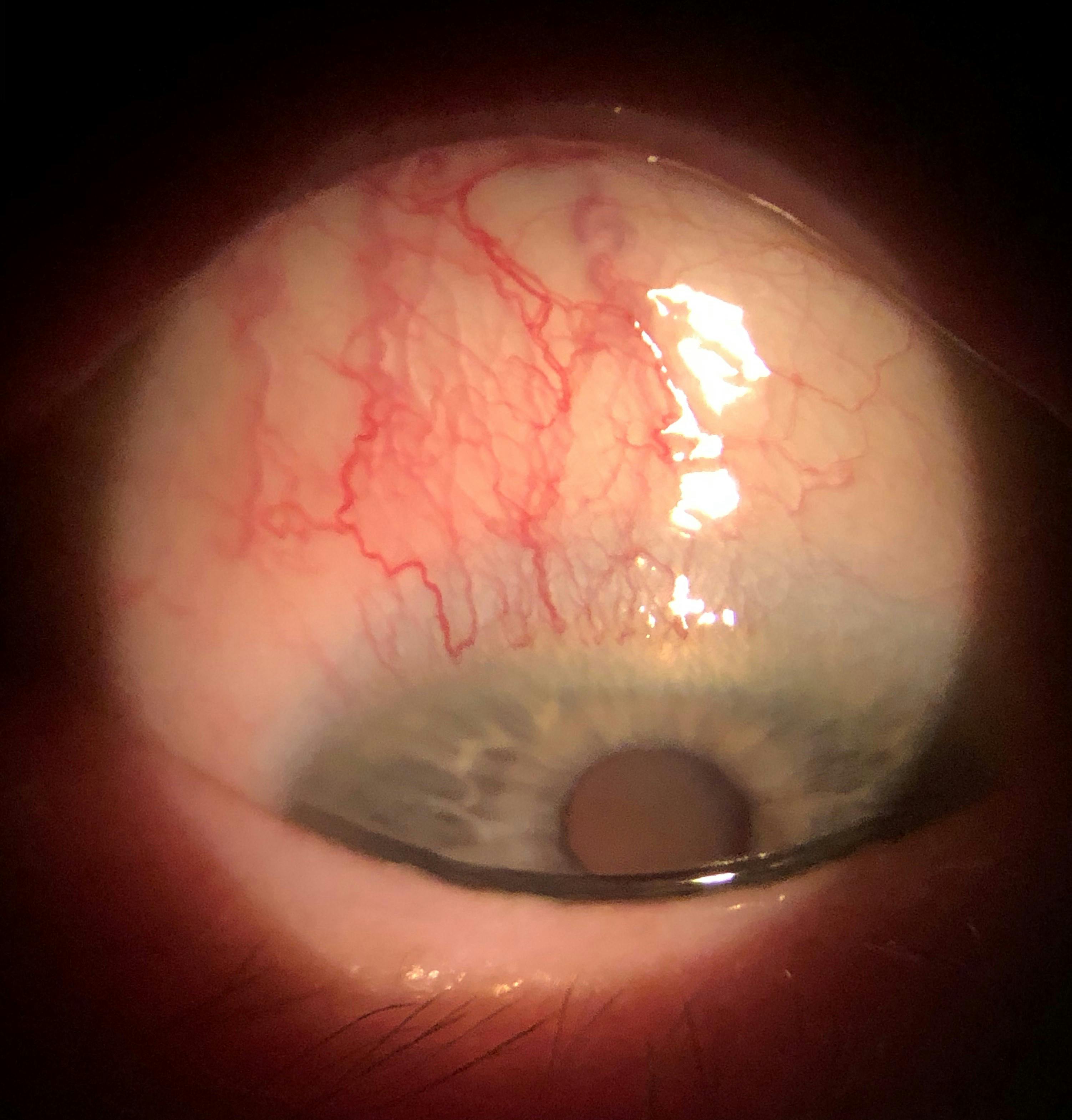
Figure 15
There is no consensus treatment for SLK, but the primary goals of treatment are to decrease inflammation and reduce mechanical friction between the bulbar conjunctiva and the superior lid. Options for inflammation control include a short course of topical steroids (loteprednol etabonate 0.5% QID for 1-2 weeks) and cyclosporine, such as Cequa, or Xiidra BID for long-term inflammation management. Treatments aimed at relieving friction include soft bandage contact lenses,168 artificial tears for lubrication (thicker gels such as Siccaforte (carbomer 0.2%, AGEPHA Pharma) work well for this purpose), or the use of topical silver nitrate applied to the superior conjunctiva.161
The use of silver nitrate essentially acts as a form of chemical cauterization to the redundant conjunctival tissue reducing the underlying source of friction. Topical vitamin A has been shown to help in some cases of SLK, making Optase Hylo Night (SCOPE) ointment an excellent choice as it contains vitamin A and provides significant lubrication as well.169
Floppy eyelid syndrome
Floppy eyelid syndrome (FES) is a commonly overlooked condition that results in chronic papillary conjunctivitis. FES refers to increased lid laxity, usually bilateral, that causes increased mechanical friction between the superior lid and ocular surface.170 Patients may also report that their lid easily “flips” or everts, especially while sleeping with their face against a pillow. The condition also tends to be more pronounced on the side the patient sleeps on.170
In addition to redness, stringy discharge, and the papillary reaction (papillae tend to be small and fine, giving a “velvety” appearance), these patients are also prone to inferior SPK, corneal abrasions, and recurrent corneal erosions due to nocturnal exposure. There is a significant association between sleep apnea and FES,171 so any patients reporting sleep apnea should be evaluated for FES and any patients found to have FES should be questioned about sleep apnea (Do they snore? Do they wake up feeling tired even after a full night of sleep?) and a sleep study ordered.
FES is also associated with obesity,172 Down Syndrome,173 and keratoconus,174 which may be caused by the mechanical rubbing of the lid against the cornea resulting in thinning. FES is diagnosed clinically based on signs and symptoms, especially excessive lid laxity which can easily be tested by simply lifting the lids. If FES is present, the lids will easily “stretch” and pull away from the globe.
Prevention of mechanical friction and addressing any underlying associations are keys to managing FES. To prevent rubbing and nocturnal exposure during sleep, some form of eyelid cover is recommended. This can take the form of sleep goggles, such as the EYESEALS 4.0 Hydrating Sleep Mask (EyeEco), or lid taping in individuals who struggle to wear goggles. However, many patients find taping their lids closed cumbersome and ineffective, so in these cases the use of adhesive eyepatches, such as the Nexcare Opticlude (3M) eye patches, which are typically used for amblyopia patching, tend to be more comfortable options that also create a better seal.
Additionally, patients can use a nighttime ointment or gel to help keep the ocular surface lubricated throughout the night. Optase Hylo Night (SCOPE) is an excellent choice as it is preservative free and contains vitamin A, which can promote surface healing.175 Another option is Siccasan (dexpanthenol 5%, AGEPHA Pharma), which is a lighter gel which some patients prefer as it is less blurring than ointments. Topical antihistamine-mast cell stabilizers such as olopatadine can be used if significant itching is present.
Treating associated sleep apnea is a crucial aspect of managing FES as CPAP use has been shown to improve FES, and more importantly untreated sleep apnea can lead to life-threatening conditions such as hypertension and congestive cardiomyopathy.176
FES is caused by excess laxity of the lids and results in a chronic mechanical conjunctivitis. shown in Figure 16.


Figure 16
Mucus fishing syndrome
Mucus fishing syndrome (MFS) refers to a condition where repeated mechanical eye rubbing or extraction of mucus from the eye, usually at the nasal or lateral canthus, results in further mucus production. Therefore, MSF is not so much an isolated entity as it is a sequala to a previous condition. MSF usually starts with a patient experiencing some form of conjunctivitis or related condition that produces mucus. The patient then attempts to remove the mucus, often digitally, and in the process causes irritation to the ocular surface. The surface then responds to this insult by producing mucus to lubricate and protect the affected area, which in turn causes the patient to repeat the mucus removal leading to a vicious cycle.177
These patients will display injection, often localized to the site of routine mucus extraction, and associated staining in that region, and often self-report ropey discharge. When patients present with these signs and symptoms ask them if they tend to “dig” at their eyes to get mucus out as an affirmative answer will confirm the diagnosis.
MFS is treated by addressing the underlying initiating condition, such as dry eye or allergic conjunctivitis, and providing palliative care while advising the patient to discontinue the “fishing” behavior and avoid touching the eyes. Typically, a short course of steroids, a topical antihistamine-mast cell stabilizer, such as olopatadine, and artificial tears are effective at keeping the patient comfortable while the condition resolves.
Allergic conjunctivitis
Overview
Allergic conjunctivitis (AC) is a common condition that can affect anyone of any age, but usually affects children to young adults more than the elderly.178,179 It is estimated that up to 40% of the US population suffers from ocular allergies.180 AC is most common in spring and summer, which is associated with seasonal allergies.7
The classic hallmark signs and symptoms of the condition are itching, hyperemia, epiphora, mild photophobia, papillary reaction, and ropey or stringy discharge.178,179,181-184 The redness observed is typically mild, giving the eye a pink appearance. The fine papillae on the palpebral conjunctiva can result in a “velvety” appearance, but in chronic cases the papillae can grow to over 1 mm in size which are referred to as giant or cobblestone papillae.
In acute cases the allergic reaction is often accompanied by chemosis and occasionally swelling of the lids.178,179,182,183 The underlying mechanism of AC is a Type I hypersensitivity reaction178,179,181-184 and involves a sensitization and activation phase.182 Typically, a person encounters some environmental allergen, such as pollen or animal dander, which begins the process. This first allergen exposure does not trigger an allergic response, but rather sensitizes the person to the allergen, as the allergen causes the body to develop IgE-receptors on mast cells.182
Upon second exposure to the allergen, the allergen binds to the IgE antibodies which in turn bind to mast cells. This complexing of IgE-bound allergens and mast cells trigger an influx of calcium into the cell which results in the degranulation of histamine. Histamine is a potent vasodilator and triggers cytokines involved in the inflammatory cascade.178,179 The result of this process is red, itchy eyes with stringy discharge.
The driving factor behind the inflammation present in AC is histamine. Histamine acts on the H1 and H2 receptors of blood vessels which causes vasodilation and increased vascular permeability resulting in the hyperemia, itching, swelling and inflammation seen in AC as blood vessels dilate and inflammatory mediators are activated.178,179,182 Therefore, treatments for all types of AC are aimed at addressing the underlying mechanisms of the allergic response. Antihistamines block H1 receptors and prevent the direct effects of histamine, however they do not prevent further histamine degranulation from mast cells.179,181-183
However, mast cell stabilizers block IgE receptors on the cells, so histamine is prevented from being released, but this does not address the histamine that has already been degranulated. Therefore, a combination antihistamine-mast cell stabilizer is ideal as it inhibits the effects of histamine while preventing further degranulation by blocking binding of the allergen-IgE complex to the mast cell surface in a single drop.179,183,185
The effect of the antihistamine should be experienced immediately, but mast cell stabilization takes longer to occur. There are numerous topical antihistamines and mast cell stabilizers, but olopatadine has long been the gold standard.179 However, alcaftadine has been shown to potentially be more efficacious as it blocks both H1 and H2 receptors rather than just H1.179 A notable side-effect for drugs containing antihistamines is mydriasis, due to their similar chemical structure to anticholinergics.186
Associated edema and inflammation are often managed with a mild steroid,179,181,182,184 as steroids block the inflammatory cascade triggered by histamine. Mild steroids are especially helpful with managing the chemosis and inflammation commonly seen in acute cases179,181,182,184 and provide rapid improvement in signs and symptoms and promote comfort.
Other palliative options, such as artificial tears and cold compresses can be used as well.181 It is advised that contact lens wearers discontinue lens wear during an acute reaction to reduce possible re-exposure to irritating antigens that may be adhered to the lens surface.181
As seen in Figure 17, allergic conjunctivitis is characterized by red eyes, a papillary reaction, and ropey discharge along with its hallmark symptom of itching.

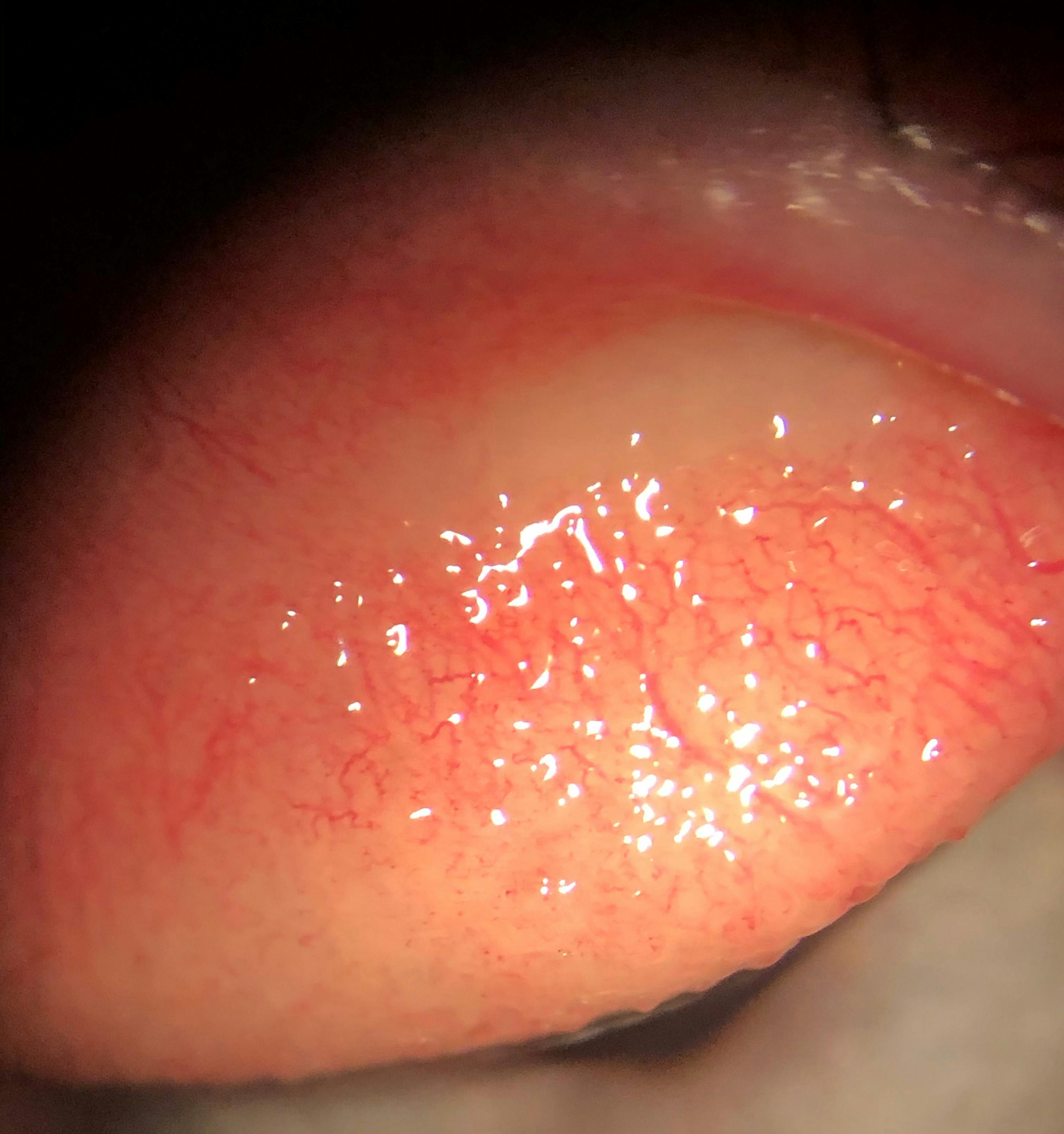
Figure 17
Acute and chronic allergic conjunctivitis
Seasonal and perennial allergic conjunctivitis are Type I hypersensitivities. Seasonal allergic conjunctivitis usually results in acute AC caused by contact with transient allergens such as pollen and plant matter that waxes and wanes seasonally, whereas perennial allergic conjunctivitis is chronic and is caused by persistent allergens such as pet dander or dust mites.180 Both produce red, itchy eyes with papillae and ropey discharge, however the signs and symptoms in perennial AC can be more subtle.179
As both forms are mediated by a Type I hypersensitivity reaction, both are treated with topical antihistamines and mast cell stabilizers.178,179,181-184 While there are many topical drops to choose from, olopatadine is considered the drop of choice. Until recently olopatadine 0.7% was only available with a prescription but is now available in an over-the-counter formulation as Pataday Once Daily Relief Extra Strength (olopatadine hydrochloride 0.7% ophthalmic solution, Alcon Laboratories). Pataday Once Daily Relief Extra Strength is an excellent choice for managing both acute and chronic AC as it has a rapid onset and prolonged duration of action, taking effect within minutes and lasting up to 24 hours with a single drop.
Other options include Lastacaft (alcaftadine 0.25% ophthalmic solution, Allergan) also dosed QD, and Alaway (ketotifen fumarate 0.035% ophthalmic solution, Bausch & Lomb) which is dosed BID but also comes in a preservative free formulation which makes it an excellent choice for patients who have sensitivity to preservatives or ocular surface disease.
If the patient also displays significant inflammation or chemosis, a topical steroid is an effective adjunct therapy. Typically, a soft steroid such as loteprednol etabonate 0.5% dosed BID-QID for 1 week resolves any inflammation. Cold compresses and artificial tears can also be used as supportive palliative therapies.
Figure 18 demonstrates a significant papillary reaction in a case of allergic conjunctivitis.


Figure 18
Figure 19 illustrates ropey or stringy discharge is a key finding that indicates allergic conjunctivitis.

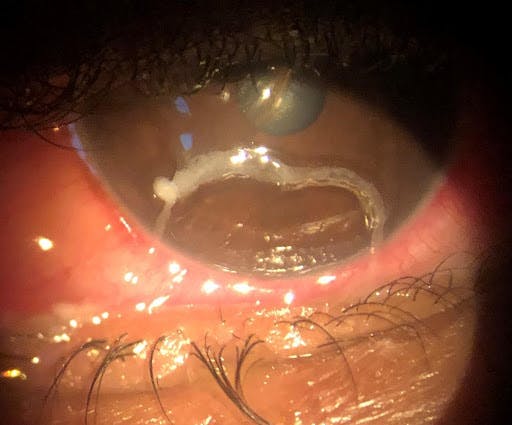
Figure 19
Vernal keratoconjunctivitis
Vernal keratoconjunctivitis (VKC) is an atopic form of AC most commonly observed in young males178,179,181 and typically occurs in warm climates and tends to be more problematic in the spring.187-189 It involves Type I IgE-mediated hypersensitivity, eosinophilic activity, and Type IV T-cell mediated hypersensitivity.190-191 The condition has variable severity but is often self-limiting and typically resolves as the patient ages, especially post puberty.189,190
The hallmark signs of VKC are severe itching, giant cobblestone papillae present on the superior tarsus, and circular white lesions consisting of eosinophils and epithelial debris at the limbus referred to as Trantas dots.190 In rare cases (3-11%), corneal ulcers, referred to as shield ulcers, develop due to inflammation and mechanical friction from contact with the cobblestone papillae.188 The eyelids themselves are typically unaffected by VKC.192
The condition is treated with the same antihistamine-mast cell stabilizers used in other forms of AC such as olopatadine 0.7%. However, considering there is typically significant inflammation associated with VKC the use of steroids is often necessary. For long-term inflammatory control both tacrolimus 0.1% ophthalmic ointment and topical cyclosporine, such as Cequa, both dosed BID have been shown to be effective while sparing the potential side-effects of long-term steroid use.
The combination of topical antihistamine-mast cell stabilizer and an anti-inflammatory like cyclosporine is often necessary to address both the Type I and IV hypersensitivity elements of the condition, as antihistamine-mast cell stabilizers address the IgE-driven histamine response of Type I hypersensitivity and cyclosporine and tacrolimus inhibit T-cell activity which drives Type IV hypersensitivity.193
In Figure 20, cobblestone papillae on the superior palpebral conjunctiva are indicative of VKC.

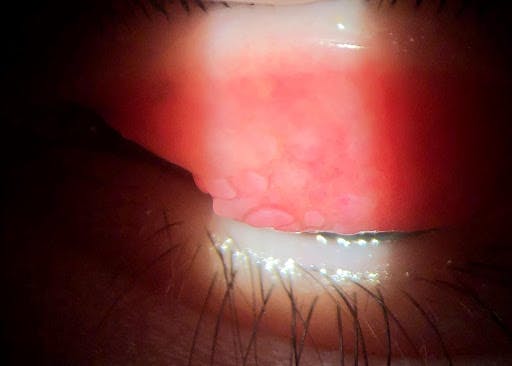
Figure 20
Figure 21 shows trantas Dots, which are collections of eosinophils and epithelial debris commonly observed in VKC.

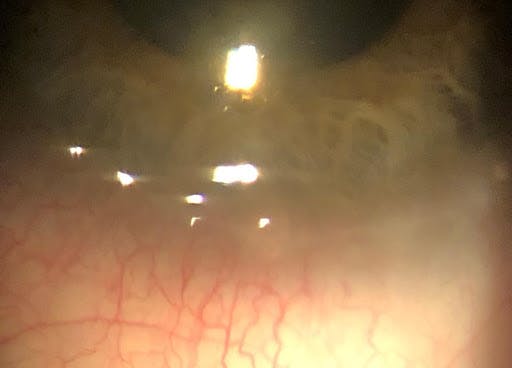
Figure 21
Atopic keratoconjunctivitis
Atopic keratoconjunctivitis (AKC) is another form of atopic AC that is typically associated with asthma or eczema1.94,195 AKC is driven by T-cell mediated Type IV hypersensitivity and Type I hypersensitivity.196,197 Like VKC, AKC presents with severe itching, significant injection, and giant papillae. However, AKC tends to affect the eyelids and lid skin as well, displaying periorbital edema, atopic dermatitis (dry, flaky, erythematous lid skin) and large papillae on the inferior, rather than the superior, palpebral conjunctiva1.79,181
There may also be the presence of an allergic “shiner”, which refers to the bluish hue of the skin below the eye due to venous congestion.198 It is worth noting the prominent atopic appearance of the eyelids themselves is a key differentiator between AKC and VKC, as VKC tends to spare the lids.192 Atopic keratoconjunctivitis is often seen in teens or middle-aged adults, whereas VKC tends to affect young children, and AKC does not tend to resolve with age.191 Additionally, AKC tends to lack seasonality while VKC is generally associated with the spring and summer months.199
Inflammation control is a crucial element to AKC management, as unchecked inflammation can lead to ocular surface scarring including symblepharon development. In mild cases, topical antihistamine-mast cell stabilizers like olopatadine 0.7% can be used to manage the condition. But in moderate to severe cases topical steroids and steroid sparing agents, such as tacrolimus 0.1% ophthalmic ointment or topical cyclosporine, such as Cequa, dosed BID are often required.
Because AKC is a chronic condition, tacrolimus and cyclosporine are often the best choice for managing AKC as the long-term use of steroids is likely to lead to side-effects such as cataract formation or increased intraocular pressure. In fact, AKC has been linked to the development of anterior and posterior subcapsular cataract development, which may be partially due to the chronic use of steroids commonly observed with AKC treatment.200 The use of tacrolimus to treat the atopic dermatitis and maceration of the eyelids also avoids the potential side-effects of topical steroid ointment and cream use, such as depigmentation and thinning of the skin.
Like VKC, AKC requires the use of both a topical antihistamine-mast cell stabilizer and an anti-inflammatory, like cyclosporine, to address the IgE-mediated Type I hypersensitivity and T-cell mediated Type IV hypersensitivity, respectively. In severe cases where the condition is unresponsive to topical treatment, oral immunosuppressants such as oral corticosteroids or cyclosporine may be required.199 These oral treatments carry significant side-effects, so patients must be monitored closely.
It is worth noting both AKC and VKC have been associated withkeratoconus development, which is thought to be related to the chronic eye rubbing secondary to the itching observed in the two conditions which can ultimately lead to corneal thinning.
An allergic “shiner,” in Figure 22, refers to the blueish coloration of the skin around the eye caused by venous congestion due to a chronic allergic reaction.


Figure 22
Uveitis: A special mention
Uveitis: A special mention
It is worth noting that a differential for all forms of “red eye”or “pink eye” is uveitis. If a patient presents with redness, photophobia, and eye pain, but lacks discharge or a papillary or follicular reaction, then uveitis is suspected. In these cases, a diagnosis of uveitis will be confirmed by an anterior chamber reaction with the presence of cells and/or flare. Also, patients experiencing uveitis tend to report pain rather than irritation when describing their discomfort.
Additionally, this pain will be “deeper” than that experienced in conjunctivitis and will be more of an ache rather than a burning or foreign body sensation. Also, photophobia tends to be more severe in uveitis than in conjunctivitis.
A quick way to differentiate between surface pain and the deeper pain associated with uveitis is to instill a drop of topical anesthetic. If the irritation improves upon instillation, the source of the pain is the ocular surface. If the pain persists, it is likely due to a deeper inflammation that the topical anesthetic does not reach, suggesting uveitis. However, some forms of conjunctivitis also are associated with uveitis, such as herpetic infections, so the two conditions are not always mutually exclusive. The takeaway is that uveitis should be ruled out in any patient presenting with a “red” or “pink” eye as their chief complaint.
Summary
Summary
Conjunctivitis is a broad clinical term that encompasses numerous infectious and noninfectious conditions. The underlying causes of these conditions can include bacterial, viral, fungal, and parasitic infections, as well as noninfectious sources such as allergies, inflammatory conditions, and mechanical irritation. Despite their different origins, the various forms of conjunctivitis all display the similar signs and symptoms of eye redness, irritation, and some form of discharge, making a specific diagnosis challenging.
There are key features to each type of conjunctivitis that makes narrowing down the differential and reaching the ultimate diagnosis possible. A few pieces of case history, the patient’s symptoms, their clinical signs, and some targeted questions will allow for timely and accurate assessment of the condition. Broadly, infectious versus noninfectious cases can be differentiated by the nature of the discharge present plus the presence of papillae or follicles on the palpebral conjunctiva.
- If the discharge is mucoid and a creamy-white or yellow-green to brown color, and papillae are present, then the source is likely bacterial. If the discharge is watery and clear in the presence of a follicular reaction, then the condition is likely viral.
- If the discharge happens to be ropey or stringy with a papillary reaction, then it is likely allergic conjunctivitis which is confirmed by the presence of itching. These two pieces of information alone can aid tremendously in determining the overarching nature of the condition.
By collecting a few more elements through clinical examination and patient history, such as corneal involvement or contact lens wearing habits, an even more specific diagnosis can be made. By keeping in mind the broad starting elements, while also recognizing the specific areas to investigate after general categorization has been made, ECPs can quickly and accurately diagnose the various forms of conjunctivitis they encounter.
Don't forget to download the Conjunctivitis Differential Diagnosis Flowcharts!
References
References
- Udeh BL, Schneider JE, Ohsfeldt RL. Cost effectiveness of a point-of-care test for adenoviral conjunctivitis. Am J Med Sci. 2008;336(3):254-264.
- Shields T, Sloane PD. A comparison of eye problems in primary care and ophthalmology practices. Fam Med. 1991;23(7):544-546.
- Channa R, Zafar SN, Canner JK, Haring RS, Schneider EB, Friedman DS. Epidemiology of eye-related emergency department visits. JAMA Ophthalmol. 2016;134(3):312-319.
- Leibowitz HM. The red eye. N Engl J Med. 2000;343(5):345-351.
- van Weert HCPM, Tellegen E, Ter Riet G. A new diagnostic index for bacterial conjunctivitis in primary care. A re-derivation study. Eur J Gen Pract. 2014;20(3):202-208.
- Azari AA, Barney NP. Conjunctivitis: a systematic review of diagnosis and treatment. JAMA. 2013;310(16):1721-1729.
- Høvding G. Acute bacterial conjunctivitis. Acta Ophthalmol. 2008;86(1):5-17.
- Rietveld RP, van Weert HCPM, ter Riet G, Bindels PJE. Diagnostic impact of signs and symptoms in acute infectious conjunctivitis: systematic literature search. BMJ. 2003;327(7418):789.
- American Academy of Ophthalmology. Cornea/External Disease Panel. Preferred Practice Pattern Guidelines: Conjunctivitis-Limited Revision. Presented at: American Academy of Ophthalmology; San Francisco, CA: 2011.
- Bingen E, Cohen R, Jourenkova N, Gehanno P. Epidemiologic study of conjunctivitis-otitis syndrome. Pediatr Infect Dis J. 2005;24(8):731-732.
- Epling J, Smucny J. Bacterial conjunctivitis. Clin Evid. 2005;(14):756-761.
- Seal DV, Barrett SP, McGill JI. Aetiology and treatment of acute bacterial infection of the external eye. Br J Ophthalmol. 1982;66(6):357-360.
- Mannis MJ, Plotnik RD. Bacterial conjunctivitis. In: Tasman W, Jaeger EA, editors. Duanes Ophthalmology on CD-ROM. Lippincott Williams & Wilkins; 2006
- Yannof J, Duker JS, editors. Disorders of the conjunctiva and limbus. In: Ophthalmology. 2nd ed. Spain: 2004:397–412.
- Chandler JW, Milam DF. Diphtheria corneal ulcers. Arch Ophthalmol. 1978;96(1):53-56.
- Thygeson P. The etiology and treatment of phlyctenular keratoconjunctivitis. Am J Ophthalmol. 1951;34(9):1217-1236.
- Tarabishy AB, Jeng BH. Bacterial conjunctivitis: a review for internists. Cleve Clin J Med. 2008;75(7):507-512.
- O’Callaghan RJ. The pathogenesis of staphylococcus aureus eye infections. Pathogens. 2018;7(1):E9.
- Eby AM, Hazlett LD. Pseudomonas keratitis, a review of where we’ve been and what lies ahead. Journal of Microbial & Biochemical Technology. 2015;08(01). doi:10.4172/1948-5948.1000254
- Holland EJ, Fingeret M, Mah FS. Use of topical steroids in conjunctivitis: a review of the evidence. Cornea. 2019;38(8):1062-1067.
- Epstein AB. Beyond the Meibomian Glands. Ophthalmology Management. 2015;19.
- Epitropoulos AT. Lid hygiene product helps reduce blepharitis, MGD symptoms. Ophthalmology Times. November 15, 2015. Accessed September 30, 2021.
- Sanford K. Comprehending, Catching and Correcting MGD. Review of Optometry. March 2021.
- Ostler HB, Lanier JD. Phlyctenular keratoconjunctivitis with special reference to the staphylococcal type. Presented at: Transactions of the Pacific Coast Oto-Ophthalmologic Society Annual Meeting. 1974;55:237-252.
- Culbertson WW, Huang AJ, Mandelbaum SH, Pflugfelder SC, Boozalis GT, Miller D. Effective treatment of phlyctenular keratoconjunctivitis with oral tetracycline. Ophthalmology. 1993;100(9):1358-1366.
- Rohatgi J, Dhaliwal U. Phlyctenular eye disease: a reappraisal. Jpn J Ophthalmol. 2000;44(2):146-150.
- Juberias JR, Calonge M, Montero J, Herreras JM, Saornil MA. Phlyctenular keratoconjunctivitis a potentially blinding disorder. Ocul Immunol Inflamm. 1996;4(2):119-123.
- Beauchamp GR, Gillette TE, Friendly DS. Phlyctenular keratoconjunctivitis. J Pediatr Ophthalmol Strabismus. 1981;18(3):22-28.
- Abu el Asrar AM, Geboes K, Maudgal PC, Emarah MH, Missotten L, Desmet V. Immunocytological study of phlyctenular eye disease. Int Ophthalmol. 1987;10(1):33-39.
- Doan S, Gabison E, Gatinel D, Duong M-H, Abitbol O, Hoang-Xuan T. Topical cyclosporine A in severe steroid-dependent childhood phlyctenular keratoconjunctivitis. Am J Ophthalmol. 2006;141(1):62-66
- Joseph S, Depaolis M. Managing Lid Disease in Lens Wearers. Review of Optometry. 2002;139:09(9/15/02).
- Whitcher JP, Cevallos V. Moraxella, down but not out--the eye bug that won’t go away. Br J Ophthalmol. 2006;90(10):1215-1216.
- Costumbrado J, Ng DK, Ghassemzadeh S. Gonococcal conjunctivitis. In: StatPearls. StatPearls Publishing; 2021.
- Sattar SA, Dimock KD, Ansari SA, Springthorpe VS. Spread of acute hemorrhagic conjunctivitis due to enterovirus-70: effect of air temperature and relative humidity on virus survival on fomites. J Med Virol. 1988;25(3):289-296.
- Thomson NR, Holden MTG, Carder C, et al. Chlamydia trachomatis: genome sequence analysis of lymphogranuloma venereum isolates. Genome Res. 2008;18(1):161-171.
- Postema EJ, Remeijer L, van der Meijden WI. Epidemiology of genital chlamydial infections in patients with chlamydial conjunctivitis; a retrospective study. Genitourin Med. 1996;72(3):203-205.
- Coppens I, Abu el-Asrar AM, Maudgal PC, Missotten L. Incidence and clinical presentation of chlamydial keratoconjunctivitis: a preliminary study. Int Ophthalmol. 1988;12(4):201-205.
- Roat MI. Adult inclusion conjunctivitis - eye disorders. Merck Manuals Professional Edition. https://www.merckmanuals.com/professional/eye-disorders/conjunctival-and-scleral-disorders/adult-inclusion-conjunctivitis. Published April 2021. Accessed October 3, 2021
- Ahmad B, Patel BC. Trachoma. In: StatPearls. StatPearls Publishing; 2021.
- Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82(11):844-851.
- Hu VH, Harding-Esch EM, Burton MJ, Bailey RL, Kadimpeul J, Mabey DCW. Epidemiology and control of trachoma: systematic review. Trop Med Int Health. 2010;15(6):673-691.
- Trachoma. World Health Organization. https://www.who.int/news-room/fact sheets/detail/trachoma. Published May 9, 2021. Accessed October 3, 2021
- Mariotti SP, Pruss A. The SAFE strategy. Preventing trachoma: a guide for environmental sanitation and improved hygiene. https://www.who.int/blindness/SAFE_en.pdf. Published 2001. Accessed October 3, 2021.
- Mannis MJ, Holland EJ. Cornea. 4th ed. St. Louis, Mo: Elsevier Inc.; 2015:518-525.
- Carithers HA. Cat-scratch disease. An overview based on a study of 1,200 patients. Am J Dis Child. 1985;139(11):1124-1133.
- Murakami K, Tsukahara M, Tsuneoka H, et al. Cat scratch disease: analysis of 130 seropositive cases. J Infect Chemother. 2002;8(4):349-352.
- Cat-scratch disease | sahealth - sahealth.sa.gov.au. Cat-scratch disease - including symptoms, treatment and prevention. https://www.sahealth.sa.gov.au/wps/wcm/connect/Public+Content/SA+Health+Internet/Conditions/Infectious+Diseases/Cat+scratch+disease/Cat-Scratch+Disease+-+Including+Symptoms+Treatment+And+Prevention. Published September 4, 2021. Accessed September 30, 2021.
- Menezes AS, Ribeiro D, Lima AF. Cat-scratch disease with parinaud’s oculoglandular syndrome. Turk Arch Otorhinolaryngol. 2020;58(1):48-51.
- Gok SE, Kocagul Celikbas A, Baykam N, et al. Evaluation of tularemia cases focusing on the oculoglandular form. J Infect Dev Ctries. 2014;8(10):1277-1284.
- Parola P, Raoult D. Rickettsioses éruptives. EMC Maladies infectieuses. 1998:24.
- McDade JE. Rickettsial diseases. In: Hausler WJ, Sussman M, eds. Topley and Wilson’s Microbiology and Microbial Infections, 9th ed. London: Arnold 1998:995-1011.
- Rocky Mountain Spotted Fever. NORD (National Organization for Rare Disorders). https://rarediseases.org/rare-diseases/rocky-mountain-spotted-fever/. Published 2009. Accessed October 3, 2021.
- Rocky Mountain Spotted Fever - Epidemiology and statistics. Centers for Disease Control and Prevention. https://www.cdc.gov/rmsf/stats/index.html. Published August 3, 2021. Accessed October 3, 2021.
- Patel S. Rocky Mountain Spotted Fever (RMSF) clinical presentation: History, Physical Examination. Rocky Mountain Spotted Fever (RMSF) Clinical Presentation: History, Physical Examination. https://emedicine.medscape.com/article/228042-clinical#b3. Published July 23, 2021. Accessed October 3, 2021.
- Abroug N, Khochtali S, Kahloun R, Mahmoud A, Attia S, Khairallah M. Ocular Manifestations of Rickettsial Disease. Journal of Infectious Diseases and Therapy. 2014;02(03). doi:10.4172/2332-0877.1000140
- Lyme disease: What you need to know. Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/resources/brochure/lymediseasebrochure-P.pdf. Accessed October 3, 2021.
- Hoen AG, Margos G, Bent SJ, et al. Phylogeography of Borrelia burgdorferi in the eastern United States reflects multiple independent Lyme disease emergence events. Proc Natl Acad Sci U S A. 2009;106(35):15013-15018.
- Lyme Disease Data tables: Historical data. Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/stats/tables.html. Published May 5, 2021. Accessed October 3, 2021.
- How many people get lyme disease? Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/stats/humancases.html. Published January 13, 2021. Accessed October 3, 2021.
- Lesser RL. Ocular manifestations of Lyme disease. Am J Med. 1995;98(4A):60S-62S.
- Signs and symptoms of untreated Lyme disease. Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/signs_symptoms/. Published January 15, 2021. Accessed October 3, 2021.
- Steere AC, Coburn J, Glickstein L. The emergence of Lyme disease. J Clin Invest. 2004;113(8):1093-1101.
- Pachner AR, Steiner I. Lyme neuroborreliosis: infection, immunity, and inflammation. Lancet Neurol. 2007;6(6):544-552.
- Wilske B. Epidemiology and diagnosis of Lyme borreliosis. Ann Med. 2005;37(8):568-579.
- Fitch CP, Rapoza PA, Owens S, et al. Epidemiology and diagnosis of acute conjunctivitis at an inner-city hospital. Ophthalmology. 1989;96(8):1215-1220.
- O’Brien TP, Jeng BH, McDonald M, Raizman MB. Acute conjunctivitis: truth and misconceptions. Curr Med Res Opin. 2009;25(8):1953-1961.
- Kaufman HE. Adenovirus advances: new diagnostic and therapeutic options. Curr Opin Ophthalmol. 2011;22(4):290-293.
- Solano D, Fu L, Czyz CN. Viral conjunctivitis. In: StatPearls. StatPearls Publishing; 2021.
- Sendrowski DP, Maher J. Claim Victory over Viral Conjunctivitis. Reveiw of Optometry. June 2016.
- Ghebremedhin B. Human adenovirus: Viral pathogen with increasing importance. Eur J Microbiol Immunol (Bp). 2014;4(1):26-33.
- Melton R, Thomas R. Current trends in medical management. Presented at: American Academy of Optometry. Seattle, WA 2013.
- Shovlin JP. What’s the Buzz About Betadine? Review of Optometry. September 2011.
- Wilkins MR, Khan S, Bunce C, Khawaja A, Siriwardena D, Larkin DFP. A randomised placebo-controlled trial of topical steroid in presumed viral conjunctivitis. Br J Ophthalmol. 2011;95(9):1299-1303.
- Pelletier JS, Stewart K, Trattler W, et al. A combination povidone-iodine 0.4%/dexamethasone 0.1% ophthalmic suspension in the treatment of adenoviral conjunctivitis. Adv Ther. 2009;26(8):776-783.
- Pepose JS, Narvekar A, Liu W, Haque R. A randomized controlled trial of povidone-iodine/dexamethasone ophthalmic suspension for acute viral conjunctivitis. Clin Ophthalmol. 2019;13:535-544.
- Chronister DR, Kowalski RP, Mah FS, Thompson PP. An independent in vitro comparison of povidone iodine and SteriLid. J Ocul Pharmacol Ther. 2010;26(3):277-280.
- Chintakuntlawar AV, Chodosh J. Cellular and tissue architecture of conjunctival membranes in epidemic keratoconjunctivitis. Ocul Immunol Inflamm. 2010;18(5):341-345.
- Bawazeer A. Epidemic Keratoconjunctivitis (EKC). Background, Patient Education, Etiology. http://emedicine.medscape.com/article/1192751-overview#a0101. Published July 19, 2021. Accessed October 3, 2021.
- Pihos AM. Epidemic keratoconjunctivitis: A review of current concepts in management. J Optom. 2013;6(2):69-74.
- Butt AL, Chodosh J. Adenoviral keratoconjunctivitis in a tertiary care eye clinic. Cornea. 2006;25(2):199-202.
- Mahmood AR, Narang AT. Diagnosis and management of the acute red eye. Emerg Med Clin North Am. 2008;26(1):35-55, vi.
- Scott IU. Pharyngoconjunctival fever (PCF) clinical presentation: History, physical, causes. Pharyngoconjunctival Fever (PCF) Clinical Presentation: History, Physical, Causes. https://emedicine.medscape.com/article/1192323-clinical. Published July 15, 2021. Accessed October 3, 2021.
- Li J, Lu X, Sun Y, et al. A swimming pool-associated outbreak of pharyngoconjunctival fever caused by human adenovirus type 4 in Beijing, China. Int J Infect Dis. 2018;75:89-91.
- Rönnerstam R, Persson K, Hansson H, Renmarker K. Prevalence of chlamydial eye infection in patients attending an eye clinic, a VD clinic, and in healthy persons. Br J Ophthalmol. 1985;69(5):385-388.
- Harding SP, Mallinson H, Smith JL, Clearkin LG. Adult follicular conjunctivitis and neonatal ophthalmia in a Liverpool eye hospital, 1980-1984. Eye (Lond). 1987;1 ( Pt 4):512-521.
- Uchio E, Takeuchi S, Itoh N, Matsuura N, Ohno S, Aoki K. Clinical and epidemiological features of acute follicular conjunctivitis with special reference to that caused by herpes simplex virus type 1. Br J Ophthalmol. 2000;84(9):968-972.
- Woodland RM, Darougar S, Thaker U, et al. Causes of conjunctivitis and keratoconjunctivitis in Karachi, Pakistan. Trans R Soc Trop Med Hyg. 1992;86(3):317-320.
- Looker KJ, Magaret AS, May MT, et al. Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLoS One. 2015;10(10):e0140765.
- Ahmad B, Patel BC. Herpes simplex keratitis. In: StatPearls. StatPearls Publishing; 2021.
- Roozbahani M, Hammersmith KM. Management of herpes simplex virus epithelial keratitis. Curr Opin Ophthalmol. 2018;29(4):360-364.
- Shovlin JP. Got Shingles? Give This a Shot. Review of Optometry. December 2010.
- Minor M, Payne E. Herpes zoster ophthalmicus. In: StatPearls. StatPearls Publishing; 2021.
- Ostler HB, Thygeson P. The ocular manifestations of herpes zoster, varicella, infectious mononucleosis, and cytomegalovirus disease. Surv Ophthalmol. 1976;21(2):148-159.
- Kalogeropoulos CD, Bassukas ID, Moschos MM, Tabbara KF. Eye and periocular skin involvement in herpes zoster infection. Med Hypothesis Discov Innov Ophthalmol. 2015;4(4):142-156.
- Jackson JL, Gibbons R, Meyer G, Inouye L. The effect of treating herpes zoster with oral acyclovir in preventing postherpetic neuralgia. A meta-analysis. Arch Intern Med. 1997;157(8):909-912.
- Viroptic (trifluridine ophthalmic) dosing, indications, interactions, adverse effects, and more. https://reference.medscape.com/drug/viroptic-trifluridine-ophthalmic-343587. Published September 28, 2019. Accessed October 3, 2021.
- Seah I, Agrawal R. Can the coronavirus disease 2019 (COVID-19) affect the eyes? A review of coronaviruses and ocular implications in humans and animals. Ocul Immunol Inflamm. 2020;28(3):391-395.
- Cheema M, Aghazadeh H, Nazarali S, et al. Keratoconjunctivitis as the initial medical presentation of the novel coronavirus disease 2019 (COVID-19). Can J Ophthalmol. 2020;55(4):e125-e129.
- Güemes-Villahoz N, Burgos-Blasco B, García-Feijoó J, et al. Conjunctivitis in COVID-19 patients: frequency and clinical presentation. Graefes Arch Clin Exp Ophthalmol. 2020;258(11):2501-2507.
- Danesh-Meyer HV, McGhee CNJ. Implications of covid-19 for ophthalmologists. Am J Ophthalmol. 2021;223:108-118.
- Ozturker ZK. Conjunctivitis as sole symptom of COVID-19: A case report and review of literature. Eur J Ophthalmol. 2021;31(2):NP161-NP166.
- Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020;172(9):577-582.
- Symptoms of COVID-19. Centers for Disease Control and Prevention. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html#seek-medical-attention. Published February 22, 2021. Accessed October 3, 2021.
- Tuft SJ, Tullo AB. Fungal keratitis in the United Kingdom 2003-2005. Eye (Lond). 2009;23(6):1308-1313.
- Gower EW, Keay LJ, Oechsler RA, et al. Trends in fungal keratitis in the United States, 2001 to 2007. Ophthalmology. 2010;117(12):2263-2267.
- Ibrahim MM, Vanini R, Ibrahim FM, et al. Epidemiologic aspects and clinical outcome of fungal keratitis in southeastern Brazil. Eur J Ophthalmol. 2009;19(3):355-361.
- Castano G, Elnahry AG, Mada PK. Fungal keratitis. In: StatPearls. StatPearls Publishing; 2021.
- Epstein AB. In the aftermath of the Fusarium keratitis outbreak: What have we learned? Clin Ophthalmol. 2007;1(4):355-366.
- Cheng AMS, Sheha H, Tseng SCG. Recent advances on ocular Demodex infestation. Curr Opin Ophthalmol. 2015;26(4):295-300.
- Liu J, Sheha H, Tseng SCG. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol. 2010;10(5):505-510.
- O’Dell L, Sadri E. Collarettes Equal Demodex Blepharitis. Cataract & Refractive Surgery Today. https://crstoday.com/articles/collarettes-equal-demodex-blepharitis/collarettes-equal-demodex-blepharitis-2/. Accessed October 3, 2021.
- Tarsus Pharmaceuticals, Inc. Announces Positive Results of Saturn-1 Pivotal Trial Evaluating TP-03 for the Treatment of Demodex Blepharitis. Tarsus Pharmaceuticals website. https://ir.tarsusrx.com/news-releases/news-release-details/tarsus-pharmaceuticals-inc-announces-positive-results-saturn-1. June 21, 2021. Accessed September 30, 2021.
- Somani SN, Ronquillo Y, Moshirfar M. Acanthamoeba keratitis. In: StatPearls. StatPearls Publishing; 2021.
- Moore MB, McCulley JP, Luckenbach M, et al. Acanthamoeba keratitis associated with soft contact lenses. Am J Ophthalmol. 1985;100(3):396-403.
- Alver O, Baykara M, YÜrÜk M, TÜzemen NÜ. Acanthamoeba keratitis and acanthamoeba conjunctivitis: a case report. Iran J Parasitol. 2020;15(2):272-277.
- Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite. 2015;22:10.
- Clarke DW, Niederkorn JY. The pathophysiology of Acanthamoeba keratitis. Trends Parasitol. 2006;22(4):175-180.
- Maycock NJR, Jayaswal R. Update on acanthamoeba keratitis: diagnosis, treatment, and outcomes. Cornea. 2016;35(5):713-720.
- Aksozek A, McClellan K, Howard K, Niederkorn JY, Alizadeh H. Resistance of Acanthamoeba castellanii cysts to physical, chemical, and radiological conditions. J Parasitol. 2002;88(3):621-623.
- Walochnik J. Collaborative Publishing. WikiGenes. https://www.wikigenes.org/e/ref/e/11850250.html. Accessed October 3, 2021.
- Hirabayashi KE, Lin CC, Ta CN. Oral miltefosine for refractory Acanthamoeba keratitis. Am J Ophthalmol Case Rep. 2019;16:100555.
- Diemert DJ. Tissue Nematode Infections. In: Goldman’s Cecil Medicine. Elsevier; 2011:193-200.
- Pham HH, Mendoza O, Turbert D. What is onchocerciasis? American Academy of Ophthalmology. https://www.aao.org/eye-health/diseases/river-blindness-onchocerciasis. Published November 18, 2020. Accessed October 3, 2021.
- Herricks JR, Hotez PJ, Wanga V, et al. The global burden of disease study 2013: What does it mean for the NTDs? PLoS Negl Trop Dis. 2017;11(8):e0005424.
- Fox LM. Blood and Tissue Nematodes (Filarial Worms). In: Principles and Practice of Pediatric Infectious Diseases. Elsevier; 2009:1312-1317.
- Freedman DO. Onchocerciasis. In: Tropical Infectious Diseases: Principles, Pathogens and Practice. Elsevier; 2005:1176-88.
- Murdoch M. Onchocerciasis. UpToDate. http://www.uptodate.com/contents/onchocerciasis. Published October 26, 2020. Accessed October 3, 2021.
- Tamarozzi F, Halliday A, Gentil K, Hoerauf A, Pearlman E, Taylor MJ. Onchocerciasis: the role of Wolbachia bacterial endosymbionts in parasite biology, disease pathogenesis, and treatment. Clin Microbiol Rev. 2011;24(3):459-468.
- Berger RB, Blackwell NM, Lass JH, Diaconu E, Pearlman E. IL-4 and IL-13 regulation of ICAM-1 expression and eosinophil recruitment in Onchocerca volvulus keratitis. Invest Ophthalmol Vis Sci. 2002;43(9):2992-2997.
- Keiser PB, Reynolds SM, Awadzi K, Ottesen EA, Taylor MJ, Nutman TB. Bacterial endosymbionts of Onchocerca volvulus in the pathogenesis of posttreatment reactions. J Infect Dis. 2002;185(6):805-811.
- Higazi TB, Filiano A, Katholi CR, Dadzie Y, Remme JH, Unnasch TR. Wolbachia endosymbiont levels in severe and mild strains of Onchocerca volvulus. Mol Biochem Parasitol. 2005;141(1):109-112.
- Gyasi ME, Okonkwo ON, Tripathy K. Onchocerciasis. In: StatPearls. StatPearls Publishing; 2021.
- Enk CD. Onchocerciasis--river blindness. Clin Dermatol. 2006;24(3):176-180.
- Richards FO, Boatin B, Sauerbrey M, Sékétéli A. Control of onchocerciasis today: status and challenges. Trends Parasitol. 2001;17(12):558-563.
- Murphy, JJ. Dry eye and inflammation: A discussion with Dr. Michael Lemp. MDLinx.com. https://www.mdlinx.com/ophthalmology/article/846. Published May 4, 2017. Accessed September 30, 2021.
- Craig JP, Nichols KK, Akpek EK, et al. Tfos dews ii definition and classification report. Ocul Surf. 2017;15(3):276-283.
- Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea. 2012;31(5):472-8.
- Sjögren's Syndrome Information Page. National Institute of Neurological Disorders and Stroke. https://www.ninds.nih.gov/Disorders/All-Disorders/Sj%C3%B6grens-Syndrome-Information-Page. Published March 27, 2019. Accessed October 4, 2021.
- Wilkin J, Dahl M, Detmar M, et al. Standard classification of rosacea: report of the national rosacea society expert committee on the classification and staging of rosacea. J Am Acad Dermatol. 2002;46(4):584-587.
- Yamasaki K, Kanada K, Macleod DT, et al. TLR2 expression is increased in rosacea and stimulates enhanced serine protease production by keratinocytes. J Invest Dermatol. 2011;131(3):688-697.
- Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci. 2009;55(2):77-81.
- Del Rosso JQ. Advances in understanding and managing rosacea: part 1: connecting the dots between pathophysiological mechanisms and common clinical features of rosacea with emphasis on vascular changes and facial erythema. J Clin Aesthet Dermatol. 2012;5(3):16-25.
- Baldwin HE. Diagnosis and treatment of rosacea: state of the art. J Drugs Dermatol. 2012;11(6):725-730.
- Elewski BE, Draelos Z, Dréno B, Jansen T, Layton A, Picardo M. Rosacea - global diversity and optimized outcome: proposed international consensus from the Rosacea International Expert Group. J Eur Acad Dermatol Venereol. 2011;25(2):188-200.
- Starr PA, Macdonald A. Oculocutaneous aspects of rosacea. Proc R Soc Med. 1969;62(1):9-11.
- Bakar O, Demircay Z, Toker E, Cakir S. Ocular signs, symptoms and tear function tests of papulopustular rosacea patients receiving azithromycin. J Eur Acad Dermatol Venereol. 2009;23(5):544-549
- Sicks LA. Bringing Clarity to CLARE. Review of Cornea & Contact Lens. April 2015.
- Sweeney DF, Jalbert I, Covey M, et al. Clinical characterization of corneal infiltrative events observed with soft contact lens wear. Cornea. 2003;22(5):435-442.
- Sankaridurg PM, Holden BA, Jalbert I. Adverse events and infections: which ones and how many? In e. Sweeney D, Silicone Hydrogels: Continuous Wear Contact Lenses. Oxford: Butterworth-Heinemann; 2000: 217-274.
- Tompkins A. Contact lens-associated Red Eye: Causes and Corrections. Review of Optometry Continued Education. https://www.revieweducationgroup.com/ce/contact-lens-associated-red-eye. Published November 15, 2017. Accessed October 3, 2021.
- Stapleton F, Keay L, Jalbert I, Cole N. The epidemiology of contact lens related infiltrates. Optom Vis Sci. 2007;84(4):257-272.
- Holden BA, La Hood D, Grant T, et al. Gram-negative bacteria can induce contact lens related acute red eye (Clare) responses. CLAO J. 1996;22(1):47-52.
- Zantos SG, Holden BA. Ocular Changes Associated with Continuous Wear of Contact Lenses. The Australian Journal of Optometry. 1978;61(12):418-26.
- Nilsson SE. Seven-day extended wear and 30-day continuous wear of high oxygen transmissibility soft silicone hydrogel contact lenses: a randomized 1-year study of 504 patients. CLAO J. 2001;27(3):125-136.
- Stapleton F, Ramachandran L, Sweeney DF, Rao G, Holden BA. Altered conjunctival response after contact lens-related corneal inflammation. Cornea. 2003;22(5):443-447.
- Sweeney DF, Grant T, Chong MS, et al. Recurrence of acute inflammatory conditions with hydrogel extended wear. Invest Opthalmol Vis Sc 34:S1008.
- Chin T. GPC: Don’t Call it An Allergic Reaction. Review of Optometry. 2006;143:10(10/15/2006).
- Greiner JV. Giant Papillary Conjunctivitis. In: Abelson MB, ed. Allergic Diseases of the Eye. New York: WB Saunders; 2001:140-60.
- Allansmith MR, Korb DR, Greiner JV, Henriquez AS, Simon MA, Finnemore VM. Giant papillary conjunctivitis in contact lens wearers. Am J Ophthalmol. 1977;83(5):697-708.
- Katelaris CH. Giant papillary conjunctivitis--a review. Acta Ophthalmol Scand Suppl. 1999;(228):17-20.
- Theodore FH. Superior limbic keratoconjunctivitis. Eye Ear Nose Throat Mon. 1963;42:25-28.
- Wright P. Superior limbic keratoconjunctivitis. Trans Ophthalmol Soc UK 1972;92(1):555-560.
- Mendoza-Adam G, Rodríguez-García A. Superior limbic keratoconjunctivitis (SLK) and its association to systemic diseases. Rev. Mex. Oft. 2013;87(2):93-99.
- Theodore FH. Comments on findings of elevated protein-bound iodine in superior limbic keratoconjunctivitis: I. Arch Ophthalmol. 1968;79(4):508.
- Cher I. Clinical features of superior limbic keroconjunctivitis in Australia. A probable association withhyrotoxicosis. Arch Ophthalmol. 1969;82(5):580-586.
- Tenzel RR. Comments on superior limbic filamentous keratitis: II. Arch Ophthalmol. 1968;79(4):508.
- Nelson JD. Superior limbic keratoconjunctivitis (Slk). Eye (Lond). 1989;3 (Pt 2):180-189.
- Mondino BJ, Zaidman GW, Salamon SW. Use of pressure patching and soft contact lenses in superior limbic keratoconjunctivitis. Arch. Ophthalmol 1982;100:1932.
- Ohashi Y,Watanabe H., Kinoshita S, Hosotani H, Umemoto M, and Manabe R. Vitamin A eyedrops for superior limbic keratoconjuntivitis. Am. J. Ophthalmol 1988; 105:523-527.
- Culbertson WW, Ostler HB. The floppy eyelid syndrome. Am J Ophthalmol. 1981;92(4):568-575.
- Chambe J, Laib S, Hubbard J, et al. Floppy eyelid syndrome is associated with obstructive sleep apnoea: a prospective study on 127 patients. J Sleep Res. 2012;21(3):308-315.
- Salinas R, Puig M, Fry CL, Johnson DA, Kheirkhah A. Floppy eyelid syndrome: A comprehensive review. Ocul Surf. 2020;18(1):31-39.
- Tawfik HA. Floppy eyelid associated with Down syndrome. Orbit. 2013;32(5):347.
- Culbertson WW, Tseng SC. Corneal disorders in floppy eyelid syndrome. Cornea. 1994;13(1):33-42.
- Kim EC, Kim TK, Park SH, Kim MS. The wound healing effects of vitamin A eye drops after a corneal alkali burn in rats. Acta Ophthalmol. 2012;90(7):e540-546.
- Naughton MT, Bradley TD. Sleep apnea in congestive heart failure. Clin Chest Med. 1998;19(1):99-113.
- Slagle WS, Slagle AM, Brough GH. Mucus fishing syndrome: case report and new treatment option. Optometry. 2001;72(10):634-640.
- Leonardi A, Doan S, Fauquert JL, et al. Diagnostic tools in ocular allergy. Allergy. 2017;72(10):1485-1498.
- Ackerman S, Smith LM, Gomes PJ. Ocular itch associated with allergic conjunctivitis: latest evidence and clinical management. Ther Adv Chronic Dis. 2016;7(1):52-67.
- Bielory BP, O’Brien TP, Bielory L. Management of seasonal allergic conjunctivitis: guide to therapy. Acta Ophthalmol. 2012;90(5):399-407.
- Takamura E, Uchio E, Ebihara N, et al. Japanese guidelines for allergic conjunctival diseases 2017. Allergol Int. 2017;66(2):220-229.
- Carr W, Schaeffer J, Donnenfeld E. Treating allergic conjunctivitis: A once-daily medication that provides 24-hour symptom relief. Allergy Rhinol (Providence). 2016;7(2):107-14.
- Gonzalez-Estrada A, Reddy K, Dimov V, Eidelman F. Olopatadine hydrochloride ophthalmic solution for the treatment of allergic conjunctivitis. Expert Opin Pharmacother. 2017;18(11):1137-1143.
- Schröder K, Finis D, Meller S, Buhren BA, Wagenmann M, Geerling G. [Seasonal and perennial allergic rhinoconjunctivitis]. Klin Monbl Augenheilkd. 2014;231(5):496-504.
- Finn DF, Walsh JJ. Twenty-first century mast cell stabilizers. Br J Pharmacol. 2013;170(1):23-37.
- Simons FE, Simons KJ. H1 antihistamines: current status and future directions. World Allergy Organ J. 2008;1(9):145-55.
- Baab S, Le PH, Kinzer EE. Allergic conjunctivitis. In: StatPearls. StatPearls Publishing; 2021.
- Bonini S, Bonini S, Lambiase A, et al. Vernal keratoconjunctivitis revisited: a case series of 195 patients with long-term followup. Ophthalmology. 2000;107(6):1157-1163.
- Kumar S. Vernal keratoconjunctivitis: a major review. Acta Ophthalmol. 2009;87(2):133-147.
- Buckley RJ. Vernal keratoconjunctivitis. Int Ophthalmol Clin. 1988;28(4):303-308.
- La Rosa M, Lionetti E, Reibaldi M, et al. Allergic conjunctivitis: a comprehensive review of the literature. Ital J Pediatr. 2013;39:18.
- Batta P, Tu EY. Atopic Keratoconjunctivitis In: Holland EJ, Mannis MF, Lee WB. Ocular Surface Disease: Cornea, Conjunctiva and Tear Film, Elsevier; 2013.
- Safarini OA, Patel J. Calcineurin inhibitors. In: StatPearls. StatPearls Publishing; 2021.
- Guglielmetti S, Dart JK, Calder V. Atopic keratoconjunctivitis and atopic dermatitis. Curr Opin Allergy Clin Immunol. 2010;10(5):478-485.
- Hogan MJ. Atopic keratoconjunctivitis. Am J Ophthalmol. 1953;36(7 1):937-947.
- Enríquez-de-Salamanca A, Calder V, Gao J, et al. Cytokine responses by conjunctival epithelial cells: an in vitro model of ocular inflammation. Cytokine. 2008;44(1):160-167.
- Metz DP, Hingorani M, Calder VL, Buckley RJ, Lightman SL. T-cell cytokines in chronic allergic eye disease. J Allergy Clin Immunol. 1997;100(6 Pt 1):817-824.
- Bielory L, Meltzer EO, Nichols KK, Melton R, Thomas RK, Bartlett JD. An algorithm for the management of allergic conjunctivitis. Allergy Asthma Proc. 2013;34(5):408-420.
- Gurwood AS. A Red Eye Fight. Review of Optometry. October 2018.
- Bielory B, Bielory L. Atopic dermatitis and keratoconjunctivitis. Immunol Allergy Clin North Am. 2010;30(3):323-336.
