



A full schedule is only as full as the patients that show up for the appointments. There are ways in which managing a schedule can result in greater efficiencies and truly be a gauge on how the business is doing. A well-managed schedule can also help predict monthly revenue and overall office performance. Having this information in hand can give you a competitive advantage and help take some of the risks out of the unknown.
So how do you create a schedule that is traceable and alerts you to the unforeseen patterns of no-shows and rescheduling? It begins with a system and process of scheduling. Once you have your process down, you can start measuring your key performance indicators.
Let me outline the steps in creating a system that has successfully gauged our multi-location practice allowing us to know when to add more doctors, when to or when not to charge no-show fees, and when to change our patient engagement protocols.
Step one: The next appointment
This first step is about scheduling and how to schedule appointments. There are two different approaches to scheduling. The first is a recall system and the second is a pre-appointment system. The pre-appointment system is a home run compared to the single-base hit recall system.
For small, one-location offices in a small town, the recall system may be something that still works. In order to grow a larger practice with multiple doctors, it is imperative to keep the schedule moving forward and full. So the first step is ensuring all patients have a “next appointment.”
Step two: No specialized appointment slots
The second step is understanding how those patients will be scheduled in the EMR scheduler. The best way, in my opinion, is to make each time slot the same type of appointment. When you have multiple doctors and all types of different appointments, the “old” system of scheduling a glaucoma exam only in a “glaucoma time slot” is a way to get your schedulers confused and make it difficult to transition patients to an online scheduling system.
In step two I would highly recommend the time slots in the schedule are “any” slots that allow staff and patients to schedule any type of appointment into that slot.
Step 3: Patient reminders
Once the patient is pre-appointed, patient engagement software that reminds the patients in advance of their upcoming appointment is paramount. Whatever software you use, you’ll find it important to tailor the reminder intervals to your practice and appointment types.
We have found that one-week, one-day, and same-day appointment reminders are best for our practice. Then if a patient has not confirmed, we may get on the phone before the day of the appointment and track them down.
Step 4: Build the wait list
This step will help you prepare for the no-show or rescheduled appointment. If you are fortunate as a practice to have a wait list, then have your staff work the wait list when appropriate.
For no-shows, we have chosen not to charge the patient but instead make a note in their chart. When they no-show three times, we consider sending a letter and dismissing them from the practice. This is harsh, but actions by the patient speak volumes. If they are non-compliant in showing up for appointments, they are likely non-compliant in managing their eyes.
When it comes to charging no-show patients a fee, we believe you win the battle but lose the war.
Step 5: Track supply and demand
Track how full the practice is and how much demand is on the schedule. When the demand is high and no-shows/reschedules are low, consider hiring another OD.
Alternatively, consider discontinuing that managed vision care plan that is a loss leader. I love this metric because it gives me a great gauge of how we are doing currently and year-over-year trends.

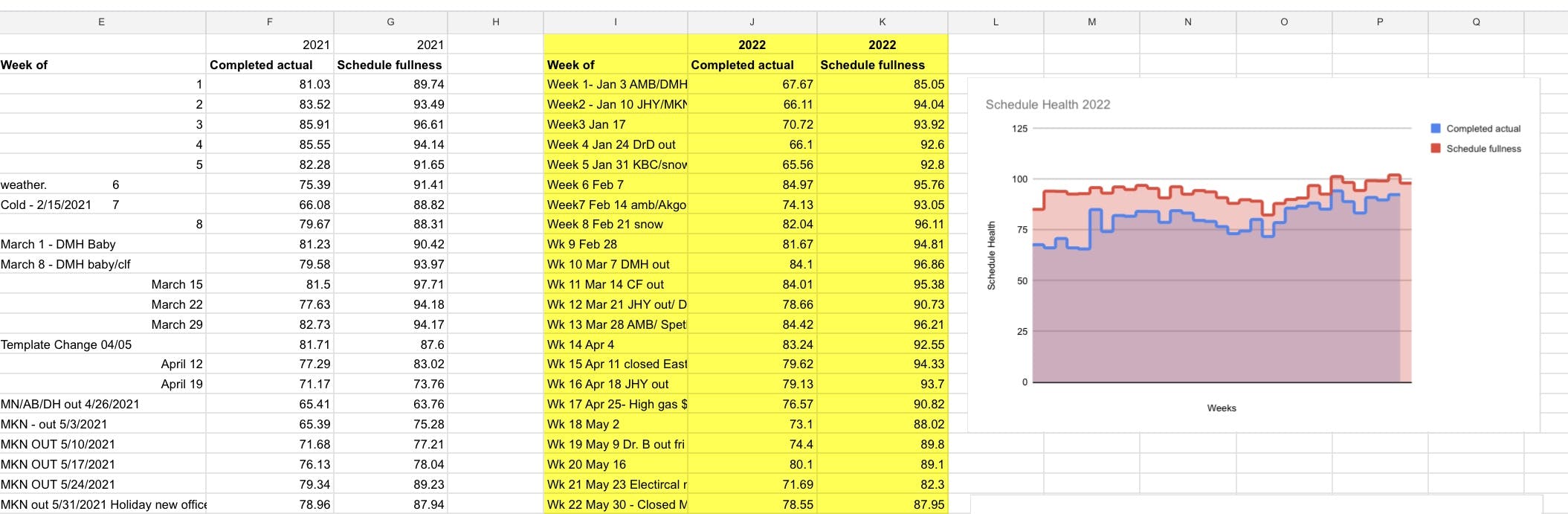
Figure 1: Example of tracking spreadsheet for schedule fullness and completed actual.
Schedule fullness: The schedule fullness is calculated on a Friday at 2pm. It is the number of appointments scheduled for the next week divided by the total number available across all locations and all doctors. The above for “Wk 22 May 30” would be 87.95% full. So out of 100 appointments available 88 were full.
Completed actual: The actual is the total patients that showed, divided by the number of spots available. This is calculated the following week on Friday at 2pm. The number of appointments completed is divided by the total number of appointments available.
The schedule fullness and completed actual above can then be compared to previous years to also look at trends that are occurring. Some readers may ask why we don’t utilize an EMR system or analytic software for this; frankly, we have not yet found one that is accurate enough to make key decisions. Analytic software can work but tends to be an indicator that is too delayed in processing the actual numbers. We want a week at a time, not months.
Measuring your scheduling team’s success
The above steps are a system that allows you to identify and manage the practice schedule. It also creates a way to measure the success of your scheduling team.
We can identify trends within the local economy or immediately measure if our schedule is impacted by an uptick in COVID or inflation concerns. If there are a significant number of no-shows, we will be able to identify this with our system and pivot on how we manage them. This is a metric that I personally monitor on a weekly basis and address our leadership if patterns start to emerge.
