Cardiovascular disease is the leading cause of death in America; approximately 697,000 people died from cardiovascular diseases in 2020.
1 Changes in the cardiovascular system often manifest as
ocular pathology.
Disrupting the ocular vasculature can lead to a multitude of issues, meaning that ophthalmologists may use the eye as a gateway to known or underlying cardiovascular diseases a patient may present with.2
Ocular manifestations of heart disease
Changes in the retinal vasculature, such as vascular dilation and tortuosity, may be caused by many conditions, including
hypertension, diabetes, coagulopathies, and even congenital heart defects.
2 Additionally, dissection of the internal carotid artery can cause amaurosis fugax, a transient monocular loss of vision.
2- Infective endocarditis: This may lead to septic emboli that travel to the eye. On exam, this is associated with Roth spots, retinitis, embolic retinopathy, or even subretinal abscess.2
- Chronic hypertension: This can lead to various degrees of hypertensive retinopathy, macular edema, and ischemia of the retina and optic nerve.1
- Coronary artery disease: the most common type of heart disease, is usually a result of atherosclerotic changes in the coronary vessel walls, which can result in a plethora of ocular disturbances, such as stroke, retinal vein occlusion, and retinal artery occlusion, to name a few.1
- Cardio-oncological pathologies: Can manifest as vision loss due to central retinal artery occlusion. An example of this is a cardiac myxoma, a benign connective tissue tumor.2
Retinal vascularity
Retinal vascular tortuosity and dilation may be seen in conditions with compromised or disrupted oxygen levels in the eye. This can be seen in acquired and
congenital conditions.
3 Velocardiofacial syndrome, also known as DiGeorge Syndrome, is caused by an autosomal dominant microdeletion at chromosome 22 (22q11.2).
4The hallmark of this syndrome is defective development of the third and fourth pharyngeal pouches, leading to a hypoplastic thymus and parathyroid glands.4 This congenital disease can cause cardiac anomalies, such as Tetralogy of Fallot or persistent truncus arteriosus, both of which are cyanotic congenital heart defects.4
In addition, acyanotic congenital heart defects, such as coarctation of the aorta, are associated with Turner syndrome.5,6 Studies have shown that retinal artery tortuosity is reported in patients with coarctation of the aorta, and retinal vascular dilation is prominent in patients with cyanotic heart disease, causing polycythemia and hypoxia.3
One of the hallmarks of Tetralogy of Fallot is a ventricular septal defect, in which there is abnormal communication between the left and right ventricles.4 This causes blood to be shunted from the left to right side of the heart, essentially leading to a decreased cardiac output and eventually pulmonary hypertension.
Additionally, coarctation of the aorta is characterized by a narrowing of the aorta at the aortic isthmus, decreasing the amount of oxygenated blood reaching the organs and extremities.5,6 Treatment of congenital heart defects involves repairing the ventricular septal defect in the case of Tetralogy of Fallot and persistent truncus arteriosus, and balloon angioplasty for coarctation of the aorta.7,8,9
Figure 1 shows fluorescein angiography illustrating familial retinal artery tortuosity.10
Figure 1: Courtesy of Retina Image Bank by Luiz Zago.
Amaurosis fugax
The internal carotid artery supplies oxygenated blood to vital structures, such as the brain and eyes. Dissection of the internal carotid artery or occlusion of the central retinal artery by microemboli can lead to amaurosis fugax, a sudden and painless
monocular vision loss followed by spontaneous recovery.
2“Carotid dissection is often due to penetrating or blunt trauma, though spontaneous dissection can occur, and is often related to hypertension.”
Retinal ischemia caused by microemboli may be due to atherosclerosis, defined as the formation of plaques within the intima of a blood vessel wall.11 Arterial hypertension and dyslipidemia are both modifiable risk factors for atherosclerosis.12 In this light, a vasculopathic patient presenting with or complaining of monocular vision loss should trigger a cardiology consult, as it may be a sign of a more serious underlying condition.
Roth spots, retinitis, embolic retinopathy, and subretinal abscesses
Infective endocarditis is inflammation of the endocardium, the innermost layer of the heart. It is typically caused by a bacterial infection, and affects patients with pre-existing damage to heart valves.13
Bacterial vegetation can lead to bacterial thromboemboli, furthering vessel occlusion and infarction due to emboli.
13 One ocular manifestation of these septic emboli is Roth spots, which are
retinal hemorrhages caused by vascular occlusion of a retinal capillary.
14 Fundus examination presents with exudative, hemorrhagic lesions with pale centers, as seen below.
Treatment of infective endocarditis involves an infectious disease consult and beginning empiric antibiotic therapy.
Figure 2 depicts a fundoscopy of the left eye, showing multiple Roth spots.15
Figure 2: Courtesy of Cheima Wathek et al.
Hypertensive retinopathy
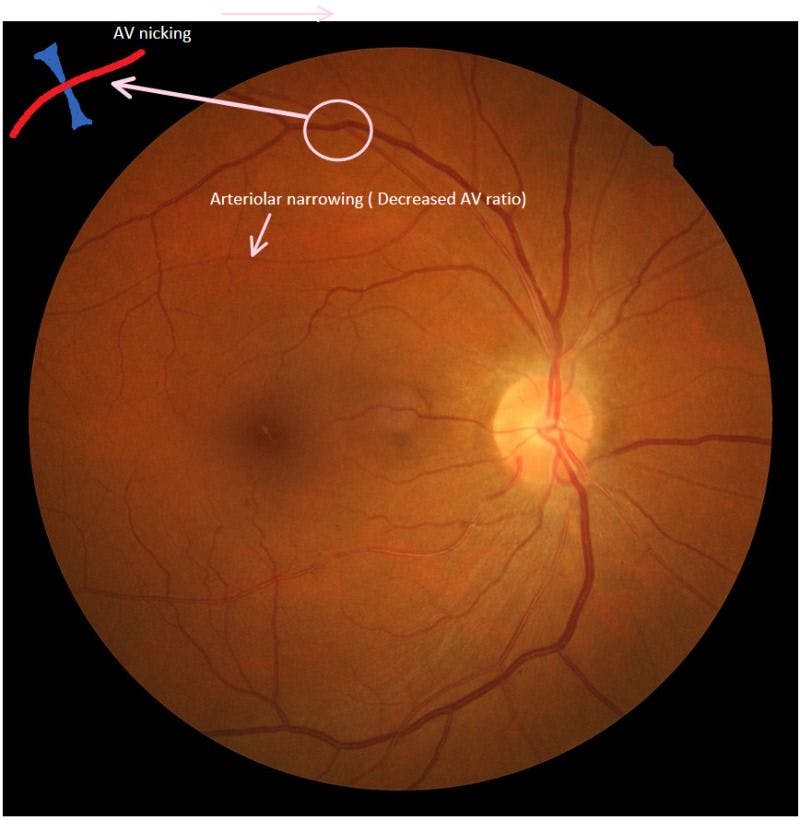
Hypertensive retinopathy is a common ocular manifestation in patients with chronic hypertension. Retinal vascular vasoconstriction precedes the hardening and breakdown of the blood-retinal barrier. The disease presents on a fundoscopic exam with cotton wool spots, flame-shaped hemorrhages, microaneurysms, and hard exudates.16 One very important sign to note is arteriovenous nicking, which is the tapering of a retinal venule at the point where a retinal arteriole crosses the retinal venule.17
In addition, a hypertensive crisis (blood pressure of >180/120mmHg) may present with papilledema, and Elschnig spots, which are round, brown-black spots with a bright ring scattered throughout the retina–these are secondary to ocular tissue infarction.17
Managing hypertensive retinopathy includes managing the underlying systemic disease. Nonpharmacological measures include weight loss, dietary approaches to stop hypertension (DASH) diet, and increasing exercise.
18 Pharmacological treatment includes the use of ACE inhibitors, angiotensin receptor blockers, and other medications to reduce blood pressure.
18 Local ophthalmic treatments include retinal laser for leaky blood vessels and intravitreal injections (steroid or
anti-VEGF) for cases with macular edema.
Figure 3 highlights a prime example of grade IV hypertensive retinopathy featuring arteriovenous nicking.19
Figure 3: Courtesy of Pranav Modi et al.
Vision loss associated with giant cell arteritis
Giant cell arteritis (GCA) is classified as an autoimmune vasculitis, resulting in chronic inflammation of both medium and large-sized arteries.
20 “The disease commonly affects the carotid artery and its branches, along with the aorta.”
Vision loss is a common manifestation of GCA due to inflammation of the ophthalmic artery, which is the first major branch of the internal carotid artery.20 Patients may also present with a scintillating scotoma, which is an arch-shaped scotoma that begins centrally and moves peripherally.21
GCA may also cause patients to experience
diplopia (double vision).
21 Recognizing and managing GCA is essential in order to prevent and minimize the risk of vision loss (both in the presenting eye and fellow eye). Patients suspected of the disease should undergo immediate diagnostic testing, including labs for erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and a complete blood count (CBC), and begin high-dose glucocorticoids.
22GCA is often co-managed with the patient’s primary care doctor and/or rheumatologist. Temporal artery biopsy is the gold standard for diagnosis and should be performed shortly after starting steroids.
Central retinal artery occlusion
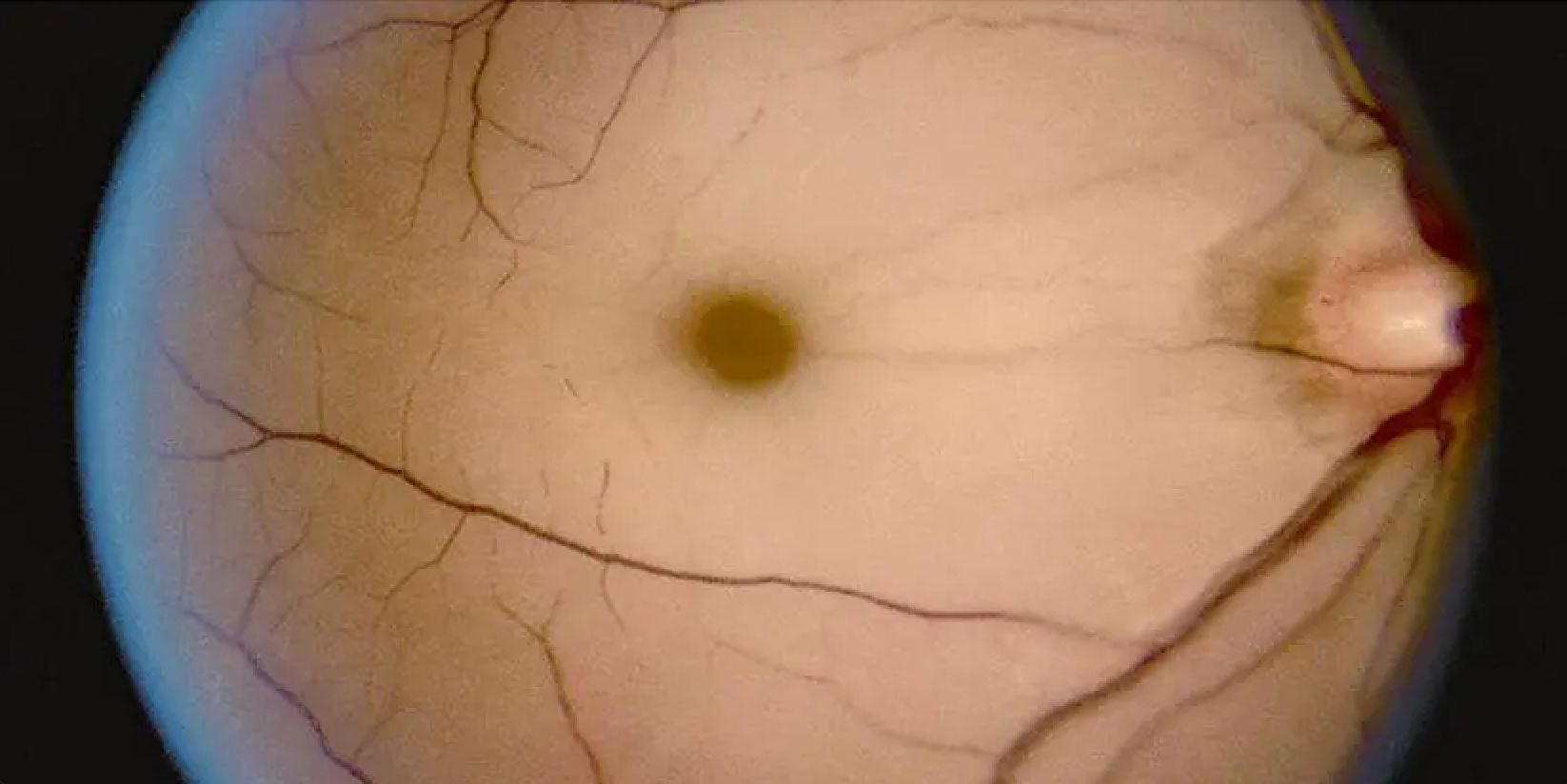
Central retinal artery occlusion is usually due to thromboemboli and may result in amaurosis fugax. Early fundoscopic exam often presents with a pale and swollen retina and a cherry-red spot near the fovea.
23 Occlusion of the central retinal artery results in severe loss of vision, ranging from finger counting to light perception, and even no-light-perception disturbances.
23 “Patients often present with a relative afferent pupillary defect.”
Occlusion to the central retinal artery is an ophthalmologic emergency; permanent retinal damage can occur quickly, with some literature citing at least 90 minutes following the occlusion.24 Various treatments have been suggested, including ocular massage, which may allow emboli to travel distally to reduce ischemia.24
Figure 4 shows fundus photography of a left eye with an acute central retinal artery occlusion, signified by its grayish-white fundus and the narrowing of retinal vessels.25
Figure 4: Courtesy of Lisa Schocket et al.
Conclusion
The ocular manifestations of cardiovascular diseases are important for
eyecare providers to look out for. Various clinical signs can signal diseases, such as hypertension, coronary artery disease, endocarditis, and more.
Binocular indirect ophthalmoscopy, optical coherence tomography (OCT), and fundus angiography/photography are essential tools in helping to diagnose ocular pathology. Awareness of these ocular manifestations is vital in managing patients’ eyesight and cardiovascular health.