



As a glaucoma specialist, I struggle with the daily emotional task of diagnosing patients with an irreversible form of vision loss, inevitably at times feeling a heavy burden of explaining the grave nature of this sight-threatening disease. Having no curative treatment to reverse the optic neuropathy in glaucoma is the crux of managing patients with this condition.
The situation as it stands
Glaucoma is the second most common cause of blindness overall and the leading cause of irreversible blindness worldwide. As life expectancy grows, the incidence and prevalence of those diagnosed with glaucoma will continue to grow. Currently, in the United States, 1.9% of the population has been diagnosed with glaucoma, and in patients aged > 80, the prevalence is 7.7%.1 In addition to the varying glaucomatous etiologies and stages, there is a significant need for more individualized treatment modalities in the management of glaucoma.
The challenges
Management of glaucoma patients presents a spectrum of challenges ranging from poor medication regimen adherence (both due to multiple medication phenomenon and side effect profiles) to secondary or worsening ocular surface disease from chronic topical preserved medications to the need for novel treatments and more targeted mechanisms of action. Amazingly, the glaucoma world is currently racing forward with technological advances and significant therapeutic growth, with the following on the horizon to provide more tools to treat these patients.
Compliance—on the ocular surface front
While benzalkonium chloride (BAK) is necessary for preservation of sterility in topical ophthalmic solutions in a multidose vial (most glaucoma topical medications), it is one of the key perpetrators of ocular surface disease, particularly dry eye disease.2 It can cause several signs and symptoms, including conjunctival hyperemia and inflammation, tear film instability, burning, tearing, foreign body sensation, and pain.
Whereas a majority of glaucoma patients are on at least one topical glaucoma medication, ocular surface disease from chronic BAK preservative is inevitable and found in up to 40% of glaucoma patients.3-4 This in turn leads to intolerance of certain topical glaucoma medications and non-adherence to medications needed to curb disease progression.

Figure 1
On the horizon is a preservative-free multidose vial of Latanoprost, formulated by TearClear (Boston, MA). As of 24 August 2021, TearClear filed an investigational new drug (IND) application for TC-002 latanoprost ophthalmic solution 0.005%. The goal is to create a safe and effective formulation of latanoprost in a multidose vial that will capture the preservative before it leaves the bottle and reaches the ocular surface. This would allow BAK to remain in the bottle, preserving the eye drop's sterility but not allowing it to get the ocular surface.
Latanoprost is currently and has been the most common glaucoma medication prescribed as a first line of treatment, most likely due to its ease of access being both generic and affordable, and due to its efficacy being at least as effective—and in some studies superior—to the gold standard of beta-blocker timolol.5-7 Having a preservative-free version of this medication could be significant in the likelihood of compliance and tolerance of this medication. Additionally, if this formulation can then be applied to other glaucoma medications, common ocular side effects can be circumvented.
Compliance—polypharmacy and multiple medications
It is known that the more drugs a patient has to take, and the longer patients have to take them, the less likely they are to get every dose. One study defined non-adherence to glaucoma medications as missing ≥5% of the prescribed pressure-lowering eye drops and found that 30% of patients reported non-adherent over nine years.8 Some other studies show that up to 25% of patients on monotherapy alone miss >25% of their doses of medication.9 Adherence is crucial to the management of glaucoma and preventing progression, and therefore alternatives to daily medication administration are essential in glaucoma treatment.
The current debate in glaucoma management concerns first-line topical medication versus selective laser trabeculoplasty (SLT). Since the 2019 publication of the pivotal LIGHT trial in the Lancet, SLT has become the first-line therapeutic modality for many glaucoma patients. The LIGHT study demonstrated improvement in quality of life, cost efficiency, and maintenance of IOP over 36 months; it demonstrated superiority to topical medications as first-line treatment.10
In 2017, direct selective laser trabeculoplasty (DSLT) was proposed as an alternative to SLT via gonioscopy; DSLT demonstrated the same efficacy of SLT without eye discomfort secondary to gonioscopy and rotation of the lens during the procedure.11 Although being applied directly through a more dispersive scleral tissue, DSLT demonstrated targeted application of energy to the trabecular meshwork with less energy (efficacy achieved at 0.3mJ/spot).
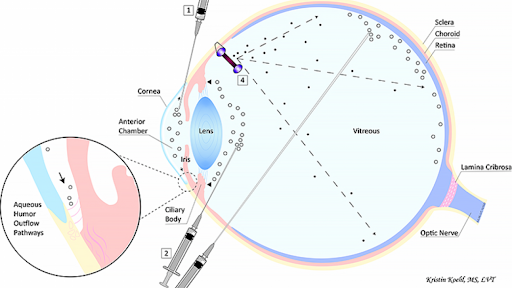
Figure 2 demonstrates gonioscopic selective laser trabeculoplasty and path of the laser beam versus direct selective laser trabeculoplasty without a gonioscopic lens with a laser beam.

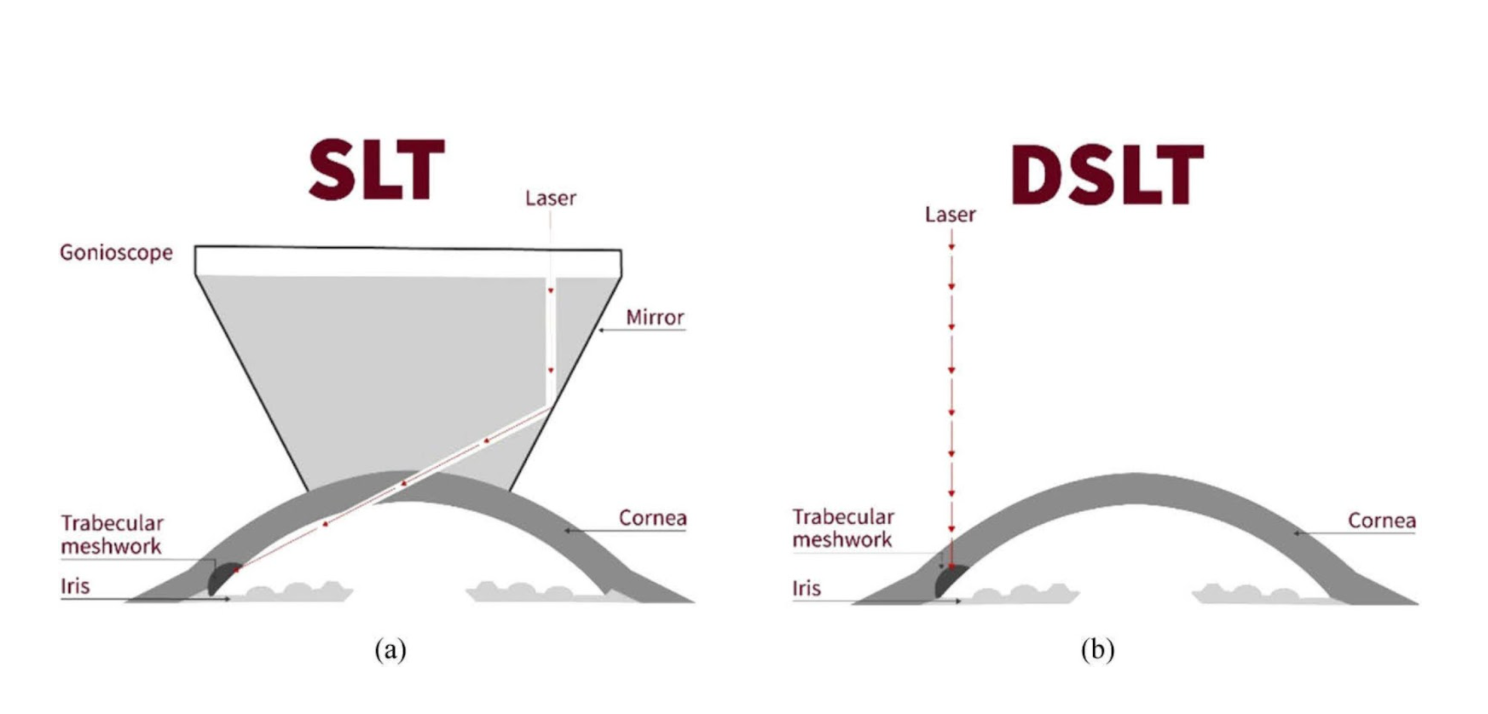
Figure 2: Diagram from Belkin M, et al. Non-contact direct selective laser trabeculoplasty: light propagation analysis. Biomed Opt Express.2020;11(6):2889–2904.
Compliance—sustained released devices
Another category of new technologies that offer a better potential for compliance is sustained-release devices that can be added to our repertoire of adjunctive glaucoma treatments for patients with poor adherence to medications.
(i) Mediprint Ophthalmics
LLT-BMT1, a contact lens printed with bimatoprost using MediPrint’s proprietary contact lens printing process, is currently undergoing clinical trials. Their SIGHT-1, safety profile and initial efficacy in phase I and IIa, showed 100% tolerability in five patients and lower hyperemia than bimatoprost topically, as well as good efficacy in a single dose. SIGHT-2 phase IIb clinical trial to assess efficacy dosing, and SIGHT-3 phase III are in the planning phases.
Figure 3, below, illustrates MediPrint’s technology of layered medication printing on contact lenses.

Figure 3
Mati Therapeutics
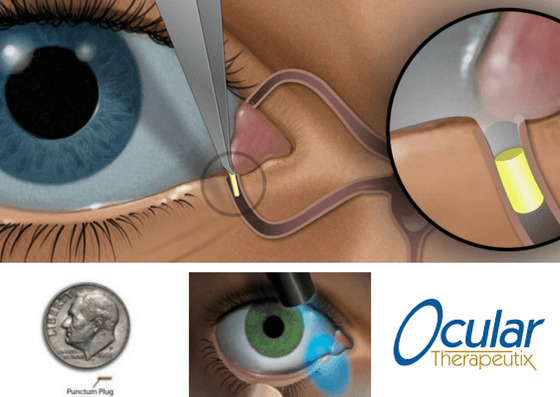
The platform Evolute consists of a translucent L-shaped latanoprost polymer matrix surrounded by silicone that is inserted into the nasolacrimal duct. This polymer can be seen by the naked eye only by everting the lower eyelid. This device will slowly elute medication at a consistent rate. They are currently in a phase II clinical trial.
In phase I the translucent L-shaped latanoprost punctal plug was found to be comfortable. It was also associated with a 20% lowering from baseline IOP over a 3-month period, and in two separate clinical trials, it had a retention rate of 92% and 96%, respectively.

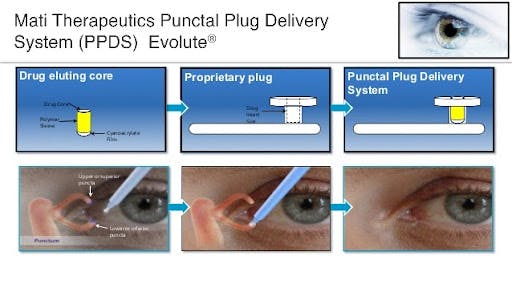
Figure 4: http://ourgsc.blogspot.com/2018/01/
Ocular Therapeutix
Their platform includes a dissolving intracanalicular depot of travaprost. The plug is invisible to the patient, but is fluorescent at the slit lamp. The prostaglandin analogue is encapsulated in polylactide microparticles in a resorbable hydrogel rod. When it comes into contact to the tear film, the rod will swell in the canaliculus and hydrolysis of the microparticles will release the drug into the tear film. Phase I safety showed no hyperemia and retention up to 90 days was 48%.
They are currently in phase II study, 73 patients randomly assigned to two groups to receive either the travoprost plug with twice daily artificial tears or timolol 0.5% twice daily with placement of a drug-free punctal plug. At 90 days, there was a 4.5 to 5.7 mm Hg reduction from baseline IOP in patients who had the travoprost punctal plug, which was clinically meaningful.
However, the control group had a placebo plug in the punctum and therefore the timolol had longer contact with the surface of the eye, possibly allowing for the more significant IOP reduction of 6.4-7.6 mmHg.

Novel and more targeted approaches
With a larger bank of knowledge on a microscopic and molecular level, technologies can now target specific tissues and areas in which the pathology of glaucoma stems from an effect.
Transforming Growth Factor β (TGFβ)
Transforming Growth Factor β (TGFβ), a signaling molecule in the inflammatory pathway, that communicates between cells resulting in inflammation and fibrosis in several disease states has been demonstrated to be in higher levels in the aqueous humor of those patient’s eyes with open angle glaucoma. The increase in this factor has been seen to lead to scarring of the trabecular meshwork drainage system.
A team at the University of Birmingham in the UK have focused on stopping this pathway, and have found in a preclinical model that a novel low molecular weight dextran-sulphate, ILB® can normalize the matrix in the eye and therefore potentially lower the IOP.
In the preclinical experimental model, they found that daily subcutaneous injections of ILB significantly reduced extracellular matrix levels of TGFB within the eye’s trabecular meshwork, normalized the IOP and prevented degeneration of retinal neurons.12 Being able to target specific molecules along the pathological process of glaucoma may allow us in the future to reverse damage caused by this disease. Currently being studied as a subcutaneous injection, a project is also in the works to formulate it into a topical gel.
The role of TGFB in glaucoma pathology is represented by Figure 6.


Figure 6: Diagram from Hasenbach K, Bergen T, et al. Potent and selective antisense oligonucleotides targeting the transforming growth factor beta (TGF-β) isoforms in advanced glaucoma: a preclinical evaluation. Medicine.2016.
Gene therapy
Gene therapy is at the forefront of many degenerative familial chronic diseases. Glaucoma is no exception. Targeting specific molecular level enzymes, receptors, as well as tissues known to be part of the glaucoma pathway has been paving the path for gene therapy to become a reality.
Adeno-associated virus vectors
Using viral vectors as a means of communication in gene therapy has been key to studying gene treatments. In 2019 a group looking specifically at human trabecular meshwork cells in postmortem eyes found that a specific double-stranded adeno associated vector (Tyrosine scAAV2) increased transduction in human trabecular meshwork (TM) cultured cells and all TM-outflow layers suggesting a proof of concept for future gene therapy work showing entry into the TM can be achieved.13 Potentiating the possibility of drug delivery or gene therapy delivery into this pathological space.
CRISPR
As of 2020, the Staphylococcus aureus-derived CRISPR-Cas9 platform has been studied in mouse models via intravitreal injection of a single recombinant adeno-associated virus vector (AAV) - a licensed FDA approved ocular gene therapy. It has been reviewed and shown to reduce IOP by selectively disrupting aqueous humor production at the ciliary body epithelium level. This platform target the aquaporin-1 receptor explicitly or the ciliary body epithelium and has not been found to target the same receptors in the cornea or retina, showing promise of specificity and efficacy.14
Non-viral vector
Although most gene therapy studies in the area of glaucoma gene therapy have been conducted using viral vectors, these viral vectors have the potential for mutagenesis. Therefore non-viral vectors, if created, may provide another tool for treatment. A proof of concept study to assess the efficacy of a non viral vector (cationic TPGS-chiotsan nanocapsules (TCNs)) were seen to be capable of targeting the MYOC gene for myocilin associated glaucoma therapy via a positively charged a non viral vector (D-α- tocopheryl glycol succinate 1000 (TPGS)-chitosan nanocapsules as).15 Myocilin found in the smooth muscle of the trabecular meshwork has been seen to be part of the pathological process in contractility in glaucoma.
Enzyme/protein-based gene therapy
One group at the Icahn School of Medicine at Mount Sinai in NYC directed their gene therapy research in mouse models at the CaMKII (calcium/calmodulin-dependent protein kinase II) pathway. They found by activating this pathway in mouse models that had gone through optic nerve crush injuries; they could protect against retinal ganglion cell damage; these cells are known to undergo the earliest signs of degeneration in glaucomatous eyes. Performing visual tests on these mice further enhanced these findings.16
Another group at the University of Cambridge studied injured retinal/optic nerve cells in mice models and found that upregulating Protrudin, in turn upregulating the endoplasmic reticulum of axon regeneration.17 Although some of these studies show promising results in both in vivo and in vitro models, there is still a significant way to go before gene-based therapy for glaucoma pathology can progress to clinical trials.
To add to our surgical repertoire
Surgically, we have some more options coming down the pipeline as early as the first quarter of 2022. Surgical techniques from MIGS to tubes and translate all, except photocoagulation laser treatments, involve improving the aqueous humor outflow pathway either via the conventional or non-conventional pathway.
Hyaluronic acid
As we know, the suprachoroidal space (SCS) is part of the non-conventional outflow pathway of aqueous humor, making up ~8-10mmHg of intraocular pressure (IOP). A study shows that injecting hyaluronic acid into the SCS will lower IOP. This procedure proposed as a non-surgical procedure involving a microneedle would potentially be a drug-free, non-surgical method shown to lower IOP over 4 months without requiring daily patient adherence.
Studied in normotensive rabbits for more than 1 month using a HA hydrogel formulation enabled IOP reduction for four months. Safety showed it was well tolerated. This adds to our more sustained treatment devices that will allow for lower IOP, improved quality of life, and therefore longer compliance by patients.18
Figure 8 illustrates histopathological analysis of hydrogel-injected eyes. Enlarged SCS space after HA injection and HA-XL injection. Rabbit eyes were injected with A) Sham, B) commercial hyaluronic acid hydrogel (HA), or C) in situ-forming hyaluronic acid hydrogel (HA-XL). Red and blue arrows indicate local hemorrhage and fibrotic tissue formation, respectively. * is the approximate site of injection.18

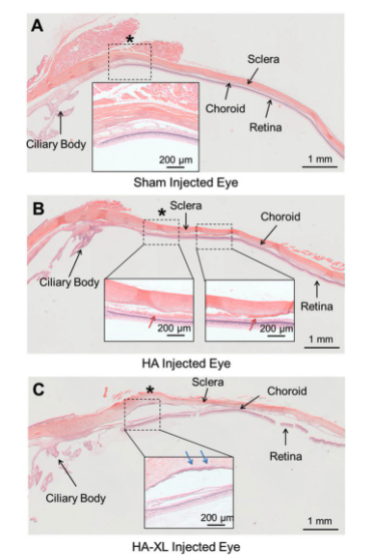
Figure 8
Preserflo
Using SIBS technology/material (biocompatible material), Preserflo is 8.5mm by length and 350 um in diameter (½ the length of standard tube) with a 70 um lumen diameter (¼ the diameter of a standard tube). Surgically inserted from an ab externo approach and using mitomycin C application to the sclera before insertion, the Preserflo provides a less invasive option of glaucoma surgical management than standard tube surgery. A multicenter study showed that Preserflo reduced mean diurnal IOP from 21.1 mm Hg to 14.2 mm Hg at month 12 compared with a reduction from 21.1 mm Hg to 11.2 mm Hg in a standard of care trabeculectomy group.
However, they found that early postoperative complications like choroidal detachment, bleb leakage, and flat or shallow anterior chamber are significantly lower than in trabeculectomy. The device is readily available in Europe, and in July 2020 the US FDA accepted its premarket approval application for the MIGS device. Santen, partnered with Glaukos, hopes to bring it to the US by 2021.
Figure 9 shows a diagram of Preserflo.

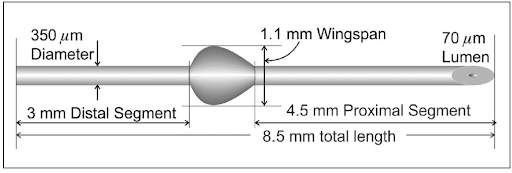
Figure 9: Courtesy of Santen.
iDose
iDose is a sustained release device that slowly releases ocular hypertensive travaprost into the anterior chamber after being surgically injected into the trabecular meshwork. It is a titanium implant (1.8 x 0.5 mm). It is currently in phase III clinical trials. Phase II was conducted comparing fast and slow eluting travaprost implant to a control treatment of sham surgery followed by topical timolol maleate 0.5%.
These trials resulted in the fast-eluting implant lowering IOP by 8.5 mm Hg (a 33% decrease from baseline), the slow-eluting implant lowering IOP by 8 mm Hg (a 32% decrease), and timolol lowering IOP by 7.6 mm Hg (a 30% decrease). This IOP reduction was stable and sustained to 12 months postimplantation. The need for additional glaucoma drops at 12 weeks was avoided by 82% of patients in both study groups and 74% in the control group.19
Figure 10 of an inserted iDose in the trabecular meshwork.

Figure 10: Courtesy of Glaukos
Takeaways
The above modalities of glaucoma treatment options offer providers new options in treatment for our patients who potentially have polypharmacy compliance issues, ocular surface intolerance of medications, or poor control of their pressure requiring further treatment. Being able to better tailor our care to each individual patient’s needs. Despite the difficult task of educating someone on their diagnosis with glaucoma, and partnering with them throughout this chronic condition, there has never been a more exciting time to be in the field of medicine (any field in my opinion!).
With consistently new advances in glaucoma, both with diagnosis and treatment, we are truly able to tailor our care to our individual patients and give them hope that with the tools available to us we can not only stave off vision loss but perhaps improve some quality of life along the way. And, one day hopefully, in our career lifetimes, we will be able to offer them a way to reverse glaucomatous optic neuropathy.
References
- Friedman DS, Wolf RCW, O’Colmain BJ, et al, Eye Diseases Prevalence Research Group. Prevalence of primary open-angle glaucoma among adults in the United States. Arch Ophthalmol.2004;122(4)532-538.
- Baudouin C. Side effects of antiglaucomatous drugs on the ocular surface. Curr Opin Ophthalmol.1996;7(2)80-86.
- Leung EW, Madieros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma.2008;17(5)350-355.
- Ghosh S, O’Hare F, Lamoureux E, Vajpayee RB, Crowston JG. Prevalence of signs and symptoms of ocular surface disease in individuals treated and not treated with glaucoma medication. Clin Exp Ophthalmol. 2012;40(7):675-681.
- Hedman K, Larsson LI. The effect of latanoprost compared with timolol in African-American, Asian, Caucasian, and Mexican open-angle glaucoma or ocular hypertensive patients. Surv Ophthalmol. 2002;47(Suppl 1):S77–89. doi: 10.1016/S0039-6257(02)00310-7. [PubMed] [CrossRef] [Google Scholar]
- Collaborative Normal-Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressures. Am J Ophthalmol. 1998;126:487–497. doi: 10.1016/S0002-9394(98)00223-2. [PubMed] [CrossRef] [Google Scholar]
- Parrish RK, Palmberg P, Sheu WP. XLT Study Group. A comparison of latanoprost, bimatoprost, and travoprost in patients with elevated intraocular pressure: a 12-week, randomized, masked-evaluator multicenter study. Am J Ophthalmol. 2003;135:688–703. doi: 10.1016/S0002-9394(03)00098-9. [PubMed] [CrossRef] [Google Scholar]
- Wolfram C, Stahlberg E, Pfeiffer N. Patient-reported non adherence with Glaucoma Therapy. J Ocul Pharmacol Ther.2019;35(4):223-228.
- Broadway DC, Cate H. Pharmacotherapy and adherence issues in treating elderly patients with glaucoma. Drugs Aging. 2015;32(7):569–581.
- G. Gazzard, E. Konstantakopoulou, D. Garway-Heath, et al. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial. Lancet.2019;393(10180)1505–1516.
- Geffen N, Ofir S, Belkin M, et al. Transscleral Selective Laser Trabeculoplasty Without a Gonioscopy Lens. J Glaucoma.2017;26(3):201–207.
- Hill LJ, Botfield HF, Begum G, et al. ILB® resolves inflammatory scarring and promotes functional tissue repair. npj Regenerative Medicine 2021; 3 volume.
- Estevez LR, Asokan P, Borras T, et al. Transduction optimization of AAV vectors for human gene therapy of glaucoma and their reversed cell entry characteristics.Gene Therapy 2020. 27;127-142.
- Wu J, Bell O, Copland D, et al. Gene Therapy for Glaucoma by Ciliary Body Aquaporin 1 Disruption Using CRISPR-Cas9. Molecular Therapy. 2020;28(3):4; 820-29.
- Karthikeyan K, Jain A, Cring M, et al. Positively Charged TPGS-Chiotsan Nanocapsules as a Non-Viral Vector for Glaucoma Gene Therapy. Investigative Ophthalmology & Visual Science. 2020, Vol.61, 2896.
- Guo X, Zhou J, Starr C, Mohns EJ, Li Y, Chen E, Yoon Y, Kellner CP, Tanaka K, Wang H, Liu W, LR, Demb JB, Crair MC, and Chen B. “Preservation of vision after CaMKII-mediated protection of retinal ganglion cells.” Published online July 22, 2021 in Cell. DOI:10.1016/j.cell.2021.06.031
- Petrova, V., Pearson, C.S., Ching, J. et al. Protrudin functions from the endoplasmic reticulum to support axon regeneration in the adult CNS. Nat Commun 11, 5614 (2020). https://doi.org/10.1038/s41467-020-19436-y
- Chae JJ, Jung JH, Zhu JW, et al. Drug-Free, Nonsurgical Reduction of Intraocular Pressure for Four Months after Suprachoroidal Injection of Hyaluronic Acid Hydrogel. Advanced Science.2020 https://doi.org/10.1002/advs.202001908
- Ibach M. Interim results of a prospective phase II study of travoprost intraocular implants. Paper presented at: the American Academy of Optometry Annual Meeting; November 9, 2018; San Antonio, Texas.
- Randomized study comparing two models of a travoprost intraocular implant to timolol maleate ophthalmic solution, 0.5%. ClinicalTrials.gov Identifier: NCT03519386. https://clinicaltrials.gov/ct2/show/NCT03519386. Accessed June 12, 2020.
