


It is the leading cause of irreversible blindness in the world and researchers have estimated that this year, nearly 80 million people will be affected by it.1
We are talking about glaucoma.
Optometrists play an increasingly critical role in the treatment and management of glaucoma. As our understanding of the disease continues to grow, ODs are on the forefront of not just preventing patients from going blind, but detecting and treating glaucoma even before any functional vision loss occurs.
In celebration of World Glaucoma Week, we are sharing some top tips when it comes to the treatment, management, and detection of glaucoma.
What is glaucoma?
Glaucoma is a group of optic neuropathies characterized by retinal ganglion cell (RGC) atrophy that is progressive in nature that results in structural and functional damage to the optic nerve. There are many types of glaucomas and etiologies, but primary open angle glaucoma (POAG) is still responsible for the majority of glaucoma worldwide.2 As our understanding of glaucoma has improved and evolved, we know now that macular evaluation is critical in all stages of glaucoma and should be part of any glaucoma evaluation.3
Tip #1: Keep these key factors in mind when diagnosing glaucoma
When it comes to diagnosing glaucoma or making a decision to start treatment for those who you consider high risk, there are a number of factors to take into consideration.
- Intraocular Pressure: It’s been well established that IOP is a risk factor for glaucoma.
- Nerve appearance: It is important to look specifically for vertical elongation of the optic nerve along with notches, thinning, and presence of drance hemes. Asymmetry between the optic nerves, typically a difference in vertical C:D ratio greater than .20 should be thought of as suspicious. It is also important to keep in mind the ISNT rule which states that the neuroretinal rim should appear thickest to thinnest, inferiorly, superiorly, nasally, and temporally.
- Visual field defects and repeatability of defects: When analyzing visual fields, it is important to remember that early glaucomatous field defects typically present as nasal steps, paracentral scotomas, arcuate bundle scotomas, or temporal wedges.
- OCT RNFL findings: OCT can be an effective tool in detecting change from glaucoma earlier on in the disease process. Special attention should be paid to the global RNFL thickness as it has a very high accuracy and reproducibility for detecting glaucomatous changes. Look for a change of more than 5 µm on global RNFL thickness as this indicates suspicion for glaucoma.4
- Central corneal thickness: OHTS investigators found that those with CCT ≤ 555 μm had three times the risk of progressing POAG than those with CCTs > 558 μm. Researchers believe CCT is a “predictive factor” as it is still unknown if CCT is an independent risk factor regardless of IOP or if the proposed risk is linked to its association with IOP.5,6
Tip #2: Stay up to date with new visual field testing technologies
ZEISS introduced a 24-2C test pattern in response to a paradigm shift in glaucoma care toward the testing and detection of macular damage in all stages of glaucoma. Previously, macular visual fields such as the 10-2 were typically reserved for advanced glaucomatous disease when patients were left with only a central island of vision but seminal work by Dr. Donald Hood has placed emphasis on the significant extent with which glaucoma damages the macula even in early stages of the disease. This has resulted in many clinicians incorporating 10-2 visual fields into their testing protocol for all glaucoma patients and suspects.3 The 24-2C combines the 24-2 protocol with 10 additional macular points. Effectively, this updates the current gold standard in glaucoma perimetry to align with current trends in glaucoma thinking. These added test points sample from the most vulnerable areas of the macula to help detect damage in all stages of glaucoma.
In honor of #GlaucomaWeek, we are giving away FREE copies of Effective Perimetry by ZEISS (the global leader in glaucoma management solutions) to ensure that future ODs are equipped to understand visual fields and make excellent clinical decisions. Head over to Instagram @covalentcareers.optometry to learn more about the giveaway!
Tip #3: Don’t forget about the angle
Evaluation of the angle is critical in the management of glaucoma and it is impossible to accurately treat glaucoma without knowing the status of it. It is easy to avoid gonioscopy due to patient discomfort or difficulty in performing the test. However, many studies have shown that angle closure glaucoma is far more common than once thought. There are significant racial predilections in the types of glaucoma, with Asian patients tending to have angle closure glaucoma and non-Asians manifesting the open angle form. Though less common, angle closure glaucoma is more likely to cause blindness with 47% of all cases of blindness due to glaucoma arising from angle closure.7 The gonioscopic evaluation of the angle allows us to draw the distinction between open and closed angle glaucoma. Though not a replacement, when using OCT for glaucoma diagnosis and management, it can aid in the detection of angle closure and does provide several novel parameters which cannot be evaluated with gonioscopy.

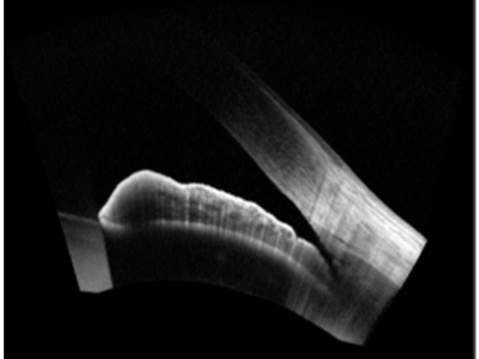
Figure 1: A narrow but open angle
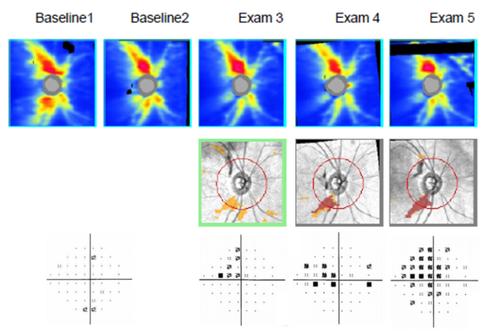
Tip #4: Understand change on OCT
Due to the progressive nature of glaucoma, change from baseline is an important indicator in the detection of disease, and therefore one must be diligent in performing serial examinations and comparing against baseline. Progression analysis software, like Guided Progression Analysis of the ZEISS CIRRUS OCT can allow for effective comparison of all subsequent scans to a patient’s baseline. When using GPA, keep in mind the floor effect, which is the measurement minimum at which RNFL thickness will no longer decrease although the disease will continue to worsen. An eye with a visual field mean deviation of approximately -22dB will reach the measurement minimum of approximately 57 μm (these numbers apply specifically to the CIRRUS OCT) at which point the RNFL thickness may no longer decrease but the eye will continue to lose vision, eventually reaching complete blindness.8 For this reason, perimetry is the preferred method for monitoring more advanced stages of glaucoma.

Tip #5: Know some of those other risk factors for glaucoma
When it comes to understanding risk, you must keep in mind all risk factors. Here are some risk factors to keep in mind:
- Age: Patient age of 60+ is a risk factor.9
- Race: African Americans have a six times higher risk of developing glaucoma than Caucasians, and the onset of glaucoma is ten years earlier in African Americans than in Caucasians with Hispanics and Asians also at higher risk.9
- Family History: Having a first degree relative with open angle glaucoma increases a person’s risk from 2.3% to 22%, and having a sibling with glaucoma increases one’s risk from 0.7% to 10.4%.9
- Systemic Conditions: There are studies that support diabetes and hypertension as contributing risk factors for glaucoma.
- Myopia: An increased axial length has been found to be a risk factor for glaucoma.9
Sources:
- Fingeret M. Optometric Clinical Practice Guideline: Care of the Patient with Open Angle Glaucoma. In: AOA, ed2010.
- “Primary Open-Angle Glaucoma Suspect PPP - 2015.” American Academy of Ophthalmology, 30 May 2018, www.aao.org/preferred-practice-pattern/primary open-angle-glaucoma-suspect-ppp-2015
- Blumberg, D M, et al. “Association Between Undetected 10-2 Visual Field Damage and Vision-Related Quality of Life in Patients With Glaucoma.” JAMA Ophthalmology., U.S. National Library of Medicine, 1 July 2017, www.ncbi.nlm nih.gov/pubmed/28542692
- Mwanza JC, Oakley JD, Budenz DL, Anderson DR. Ability of cirrus HD-OCT optic nerve head parameters to discriminate normal from glaucomatous eyes. Ophthalmology. 2011;118(2):241-248.e241.
- Gordon MO, Beiser JA, Brandt JD, et al. The Ocular Hypertension Treatment Study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):714-720; discussion 829-730.
- Brandt JD, Gordon MO, Gao F, Beiser JA, Miller JP, Kass MA. Adjusting Intraocular Pressure for Central Corneal Thickness Does Not Improve Prediction Models for Primary Open-Angle Glaucoma. Ophthalmology. 2012;119(3):437-442.
- Quigley, Harry A., and Aimee T. Broman. “The number of people with glaucoma worldwide in 2010 and 2020.” British journal of ophthalmology 90.3 (2006): 262-267.
- Schiefer, Ulrich, et al. “Spatial pattern of glaucomatous visual field loss obtained with regionally condensed stimulus arrangements.” Investigative ophthalmology & visual science 51.11 (2010): 5685-5689.
- McMonnies CW. Glaucoma history and risk factors. J Optom. 2016.
