


On this episode of Interventional Mindset, Preeya K. Gupta, MD, speaks to Julio Cesar Albarracin, MD, about new treatment options for patients with Demodex blepharitis (DB) and how to present them to patients.
Dr. Albarracin is a cataract and refractive surgeon at the Key-Whitman Eye Center in Dallas, Texas.
Diagnosing DB at the slit lamp
During his residency at Georgetown University, when Dr. Albarracin identified DB in a patient, his attending physician advised him not to say anything because of a lack of treatment options and a desire to avoid scaring the patient. Now, 2 years later, things have changed.
Over the past 2 years, Drs. Gupta and Albarracin have both noted that DB has been the cause of a significant amount of the pathology they’ve come across in-clinic, leading them to actively be on the lookout for it.
But how should you conduct an ocular surface examination to identify DB—and what signs should you be on the lookout for? Every patient that comes into Dr. Albarracin’s practice goes through the “look, lift, pull, push, pull—and stain” examination algorithm, which was recently outlined by Marjan Farid, MD.1
As part of this, he gets the patient to look down and then observes for three signs and symptoms of DB on the eyelid margin:
- Redness
- Itchiness
- Discharge from the eye
Figures 1 and 2: Slit lamp images of lash collarettes on patients with Demodex blepharitis.

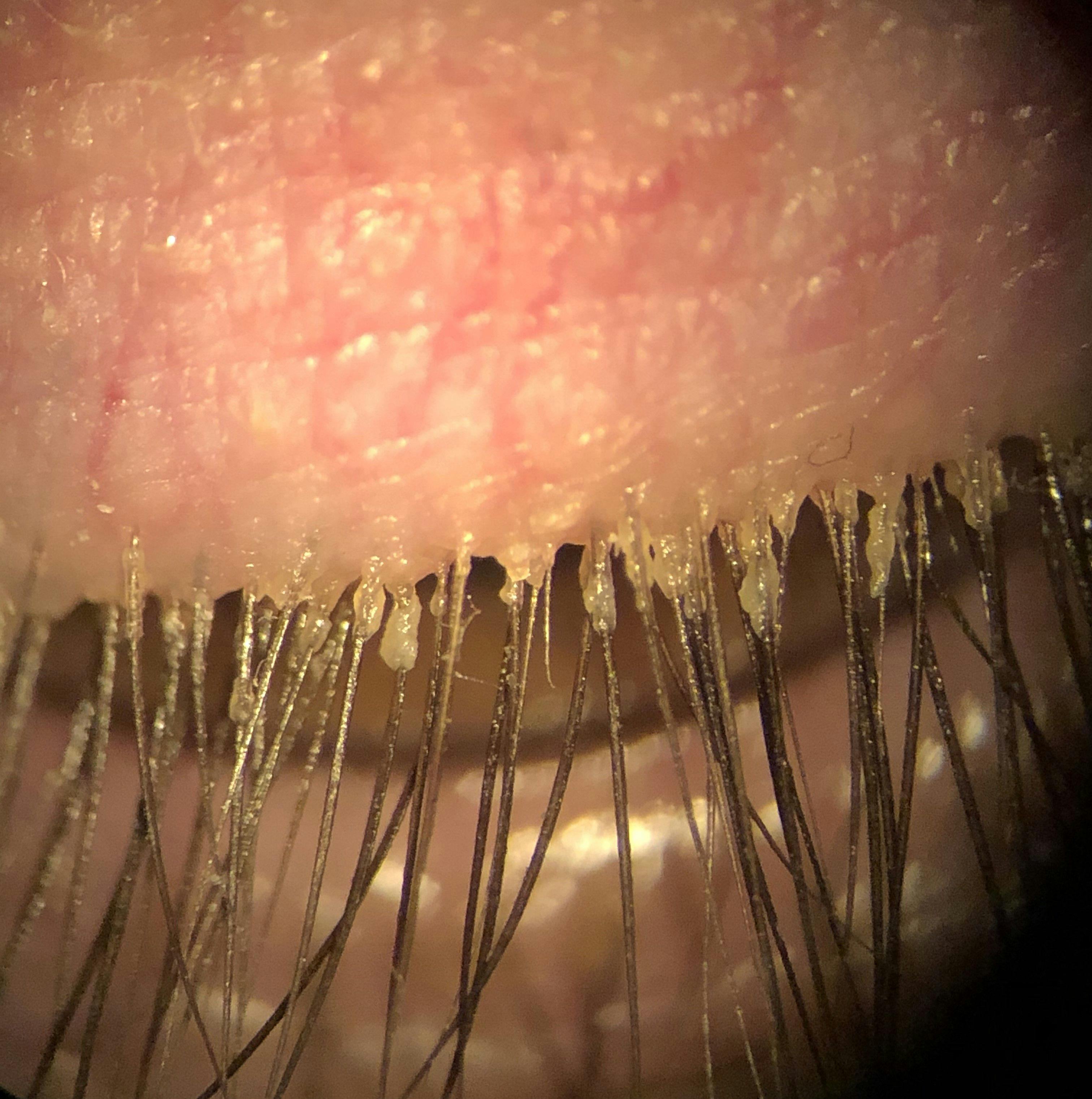

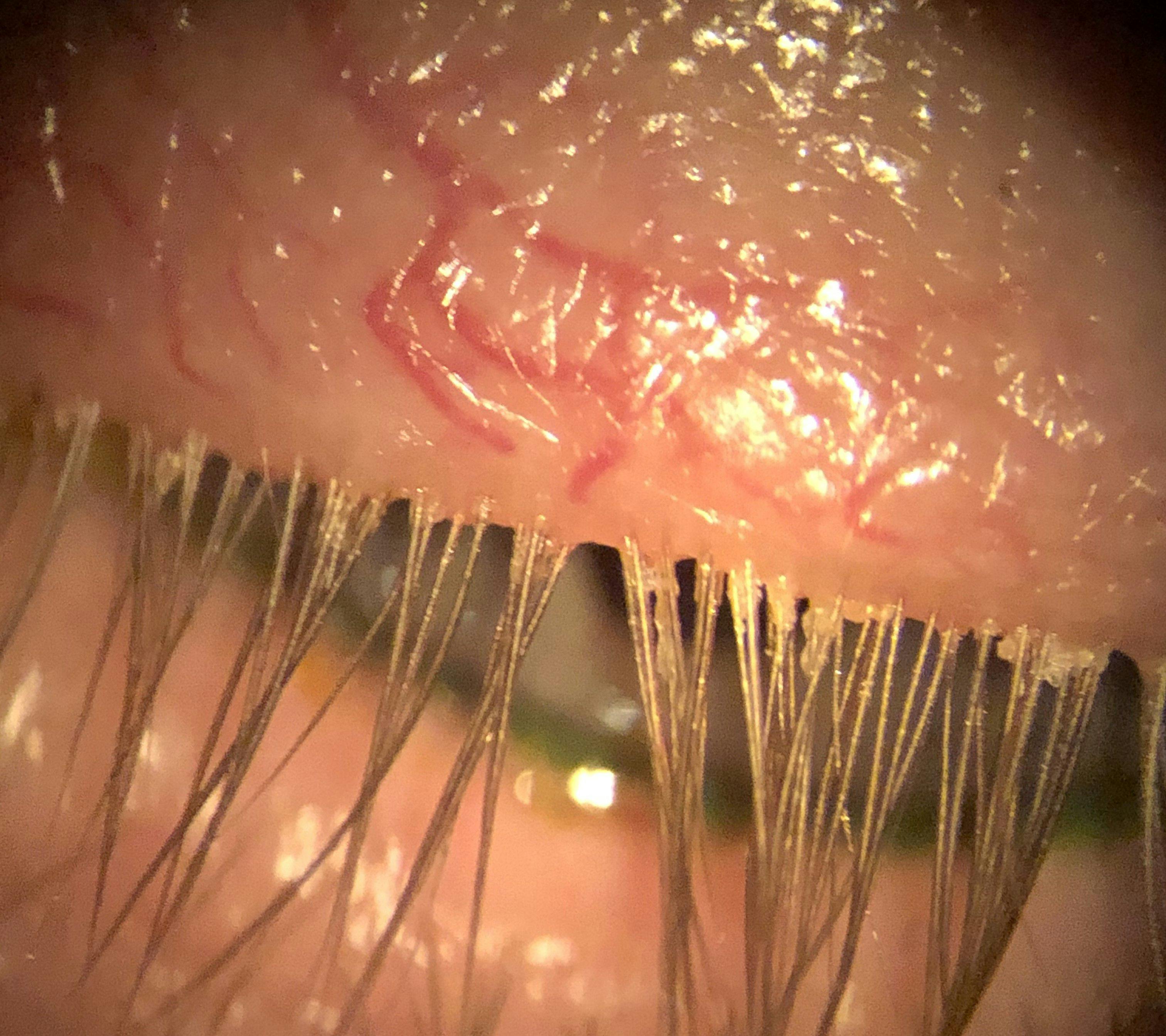
Figures 1 and 2: Courtesy of Cory Lappin, OD, MS, FAAO.
He also pushes on the meibomian glands to assess the quality of the meibum and checks for co-existing problems such as rosacea or meibomian gland dysfunction (MGD). As Dr. Gupta highlights, MGD increases the likelihood that a patient will experience DB—as does age, which increases Demodex prevalence exponentially.
A new option for treating Demodex blepharitis
The past 2 years have also come with a new treatment modality for DB in the form of XDEMVY (0.25% lotilaner ophthalmic solution, Tarsus Pharmaceuticals), an eye drop that is typically taken twice daily for a 6-week period.
Both doctors have seen good results with XDEMVY—sometimes in cases where other modalities have fallen short. In one specific case, Dr. Albarracin saw a patient with ocular surface disease (OSD) who had been given several other topical eye drops and treatment modalities, alongside intense pulsed light therapy (IPL), with no improvement.
Because, when he looked at her signs and symptoms, Dr. Albarracin noticed that they seemed consistent with DB, so he pitched XDEMVY to her as a low-risk, short-term option—that wouldn’t burn or sting like other medications—and that may offer a small amount of improvement.
Despite not promising a cure, after completing the treatment course, the patient came back to Dr. Albarracin’s office feeling completely better and having stopped other treatments. “There are just those patients that are particularly sensitive to the Demodex mites that have colonized their eyelids and lashes,” he says. “Ultimately, we don’t know until we try.”
Alongside other patients, Dr. Albarracin also has his own testimony regarding XDEMVY’s efficacy, having gone through the 6-week course himself and experienced resolution of his own DB.
And, regarding DB patients with MGD, both doctors highlighted new data showing that a 6-week course of XDEMVY improved meibomian gland secretion and flow,2 potentially acting as a jump-start for other traditional MGD therapies.
Talking DB treatment: 3 tips for having effective conversations with patients
Although there is now an effective treatment, pitching it to patients is something that some practitioners find difficult.
Here is Dr. Gupta's and Dr. Albarracin’s advice for having the conversation with your patients regarding DB:
1. Offer judgment-free descriptions
Hearing that it’s caused by mites, it may be easy for patients to feel embarrassed or to assume that they have a hygiene problem. To prevent this, it’s important to humanize the condition—for example, by explaining that everybody has mites and DB is the result of increased sensitivity to these mites, not some sort of failing on their part.
Dr. Albarracin also uses his personal experience, sharing that he himself experienced the same symptoms that the patient he is talking to currently has.
2. Meet their treatment regimen where it’s at
As mentioned earlier, many patients with DB also have existing MGD or other conditions like dry eye—meaning that they are likely already taking a number of medications and may be reluctant to add another.
Here, Dr. Gupta will explain to patients that XDEMVY isn’t a forever medication and will only require 6 weeks of compliance. But she does also highlight the need for patients to stick with it for the full course to effectively catch all the Demodex mites at all different cycles of life.
3. Use visual aids
As a visual learner, Dr. Albarracin likes to show patients what their eyes currently look like—and the difference that XDEMVY can make. There are two ways through which he does this.
Firstly, by using the “before and after” media created by TarsusRX to demonstrate his hopes for the medication’s potential benefits.3 Alongside this, he combines this with Ullman Indirect, an app created by one of his friends that allows him to capture slit lamp photos using his phone.
“I’ve found that when patients see what their eyes actually look like under the microscope—especially considering the fact that things look different macroscopically—they really appreciate it,” he explains. “It’s something that’s really changed my practice.”
Conclusion
If you’re new to XDEMVY and you’re trying to decide whether to put a patient on XDEMVY, Dr. Albarracin’s advice is that even if there’s only one collarette, if the patient is diligent with their lid hygiene, it’s worth giving XDEMVY a shot when you notice the first signs and symptoms of DB—something Dr. Gupta agrees with.
“With it being such a low-risk treatment, the potential upside is far greater than the potential downsides—especially in this population that can be very difficult to treat and keep happy over time; as things progress,” she says. “If you’re not treating Demodex blepharitis, you’re really missing the low-hanging fruit of OSD.”
This article was written by Oscelle Boye, MBiomed, based on the recorded video conversation between Drs. Gupta and Albarracin.





