


Ultra-widefield retinal imaging has had a contentious path to acceptance in the eye care community. Initially, many practitioners were amazed by the images acquired with ultra-widefield systems, but did not know how this technology could improve their patient care or office flow. As ultra-widefield technology continues to innovate, more and more eye care practitioners are implementing this technology due to increasing ease of use, image quality, and evidence that ultra-widefield imaging can improve disease management. The CLARUS® 500 from ZEISS is the next generation in ultra-widefield imaging, combining true color ultra-widefield imaging with high-quality optics in an instrument that is designed around the patient and user experience.
One of the first noteworthy articles on the utility of ultra-widefield imaging was authored by a group at the Joslin Diabetes Center, a Harvard Medical School affiliate, comparing dilated retinal examination, dilated 7-field fundus photography, and non-mydriatic ultra-widefield imaging in the grading of diabetic retinopathy. The authors concluded that there was favorable agreement between all three forms of diabetic retinopathy grading. Ultra-widefield imaging and clinical examination agreed exactly in 70% (137) of eyes and agreed within 1 level of diabetic retinopathy in 93% (184) of eyes.1 These findings are even more impressive considering that ultra-widefield imaging was performed more quickly than standard photography and without the need for dilation. Recent investigations on the use of ultra-widefield imaging in diabetic retinopathy have shown that the presence of peripheral diabetic retinopathy is associated with a 4.7-fold increased risk of progression to PDR and a 3.2-fold increased risk of progression in diabetic severity by at least 2 levels.2 A surprising result to come out of this study is that 51% of all patients had diabetic retinopathy lesions that were predominantly peripheral.
Apart from its utility in pathology detection, ultra-widefield imaging is becoming an essential part of many practices as the healthcare landscape is quickly changing. As eye care providers are being asked to see more patients, while providing quality care in less time with shrinking reimbursement, technologies such as auto-refractors and optical coherence tomography (OCT) have become indispensable. OCT has revolutionized ophthalmic care by improving detection and assessment of ocular disease while auto-refractors have improved doctor efficiency. In a way, ultra-widefield retinal imaging is a combination of both aspects. When used in conjunction with a dilated fundus exam (DFE), ultra-widefield retinal imaging acts as the autorefractor to your ophthalmoscopy. A quick review of images prior to the DFE can help highlight any abnormalities that need extra attention during the DFE, effectively “guiding” the exam in a more deliberate fashion. Directing more time to pathology and less time to normal retina can help streamline the examination without compromising thoroughness. Patient education is streamlined with ultra-widefield imaging because patients can now see what doctors see, oftentimes providing a sobering “wake up call,” especially to the non-compliant or dissenting patient.
Want more content dedicated to ocular disease? Check out our medical optometry resource page for tons of clinical cases and images and information on using OCT and ultra-widefield imaging.
With trends moving towards multi-doctor practices, ultra- widefield imaging improves patient flow while maintaining quality of care and proper documentation across multiple visits. Extended ophthalmoscopy drawings often fall short of accurately documenting pathology for future comparison, compelling many doctors to seek an objective form of documentation. Being able to decrease inter-observer and intra-observer variability can prevent disagreement in clinical management, especially when a patient is seen by multiple doctors within a practice which improves patient outcomes and reduces patient anxiety and frustration.


A 200° ultra-widefield image of a healthy eye.
Many would argue that the above mentioned advantages are not truly evident with current and past iterations of ultra- widefield retinal imaging due to color inaccuracy, retinal distortion, inadequate image resolution, or difficulty in image acquisition. The latest instrument from ZEISS, the CLARUS 500, aims to solve all of these issues and provide quality images that are easily acquired. It is a true color ultra-widefield retinal imaging device that provides high-quality images of the optic nerve head, macula, and periphery with 7 micron resolution. To help in the disease management of both macular and peripheral disease, the ZEISS CLARUS 500 is able to take 133° true color images with one capture or 200° images with an auto-merge feature. Stereoscopic photography and fundus autofluorescence (FAF) provide additional pathology visualization and detection capabilities. The ZEISS CLARUS 500 uses three wide-spectrum LEDs to enable image capturing in true color and reduce optic nerve head bleaching.
For more great clinical photos and cases, check out this article.
The partially confocal optics reduce lid, lash, and other artifacts from the anterior segment. External ocular images can also be acquired to aid in anterior segment disease management and education. The ZEISS CLARUS 500 combines numerous technical features into a sleekly designed platform with both patient and operator comfort in mind. It utilizes a standard slit lamp/joystick approach and a chin rest to improve patient comfort and remove any burden from the patient during image acquisition. A live infrared preview of the retina assists the operator in obtaining focused images without the need for multiple acquisitions. The live infrared preview allows the operator to optimize alignment while ensuring that lids and lashes do not interfere with the image capture, which decreases image capture time, eliminates patient exposure to excessive image capture flashes, and improves patient experience.


Real and schematic images of the ZEISS CLARUS 500 showcasing the patient-centric design.
The ZEISS CLARUS 500 combines an easy image acquisition platform with an intuitive user interface to allow for the effortless review of images. Sequential imaging of lesions is simplified by pulling forward previous image annotations. Evaluation of several images at once, including different color channels and FAF, is streamlined by coordinating images to the same retinal locus and zoom. The image review software can be installed on multiple computers to improve office flow.
Currently, many practitioners have a standard fundus camera to help in the management of posterior pole disease and an ultra- widefield system for the management of peripheral disease. Due to its increased resolution and true color, the ZEISS CLARUS 500 may aid in detection of both posterior pole disease such as glaucoma and peripheral disease such as lattice degeneration or retinal tears. These images are similar to what we traditionally see during our clinical exam, decreasing the learning curve in image interpretation and disease detection. Unlike previous systems, the ZEISS CLARUS 500 also has stereoscopic images to help distinguish pathology in cases where binocularity is an important cue. Due to its vast array of technical features and its ease of use, the ZEISS CLARUS 500 can effectively be the only fundus camera in any office, regardless of whether that office is a high volume multi-specialty practice or a one-doctor practice.

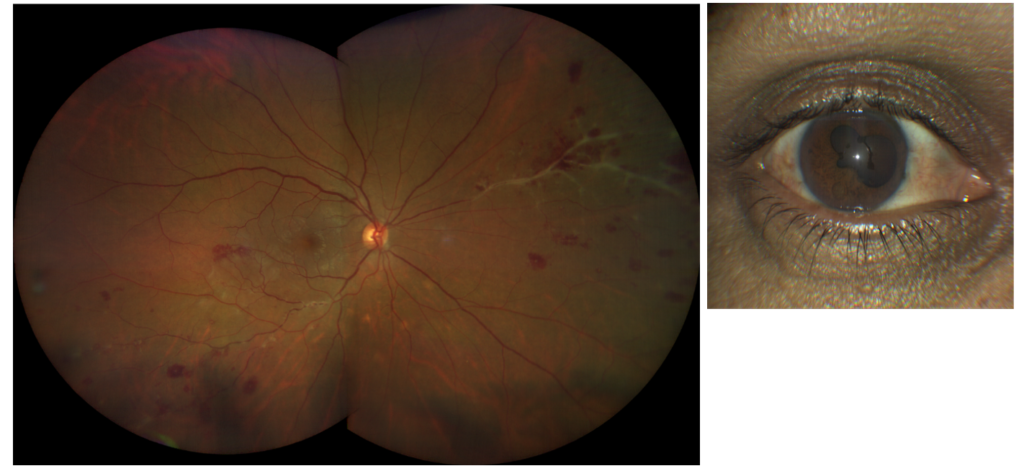
A 200° ultra-widefield image of a patient with retinal vasculitis and an external image taken with the CLARUS 500 revealing posterior synechiae.
ZEISS offers a full suite of diagnostic equipment. The ZEISS CIRRUS HD-OCT provides an invaluable tool for the management of retinal and optic nerve pathology.
Similar to the assessment of glaucoma, where multiple diagnostic technologies aid in management, the evaluation of choroidal nevi also necessitates a multimodal approach. Fundus photography is essential for the detection and documentation of choroidal nevus size and pigmentation whereas OCT helps in the evaluation of lesion structure. True color images captured with CLARUS 500 can be separated into red, green and blue channel images to help enhance the visual contrast of details in certain layers of the retina. True color imaging is also ideal for discerning abnormalities overlying choroidal nevi such as yellow drusen and orange lipofuscin. Yellow drusen are most often signs of a benign lesion while the presence of orange lipofuscin usually denotes a suspicious lesion that needs further evaluation. Using the different color channels can help differentiate choroidal lesions, which are better visualized with red separation, from more superficial lesions such as CHRPE, which are better imaged with green separation. Using serial fundus photography, any significant changes in size and pigmentation can be easily assessed.
These changes can be indicative of a choroidal melanoma and would require further evaluation. Infrared imaging and FAF can help visualize lipofuscin or retinal pigment epithelium (RPE) dysfunction, which may be suggestive of a metabolically active lesion such as a small choroidal melanoma. When reviewing multiple images, the ZEISS CLARUS 500 image review software can coordinate the images to the nevus using a common zoom factor. One can easily review color and FAF images from multiple dates to evaluate small changes in lesion size, color, or FAF. Annotations such as size are propagated onto future images so that repeat measurements do not need to be made. Other risk factors for choroidal melanoma, such as lesion thickness and presence of subretinal fluid, are more readily evaluated with OCT. This multimodal approach to nevus evaluation can help prevent superfluous referrals and preventable melanoma growth.

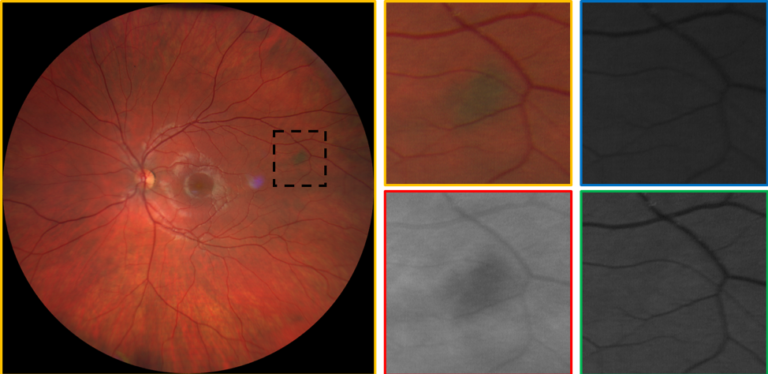
A choroidal nevus imaged in color and with blue, red, and green color channels. Note how the nevus is best visualized with red separation, which best images posterior retinal and choroidal lesions.
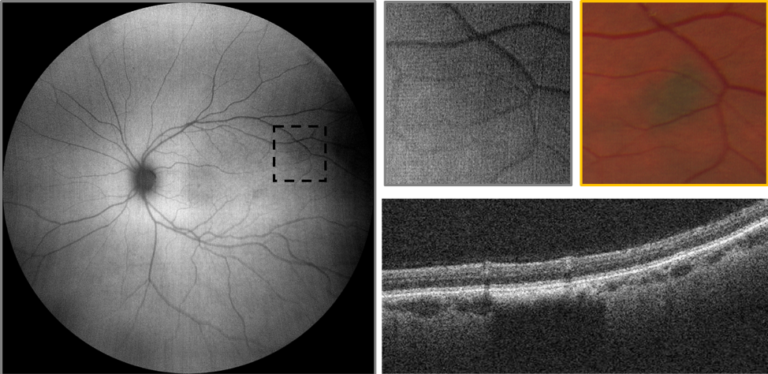
A choroidal nevus imaged with widefield FAF and OCT. FAF is an RPE phenomenon; therefore, the nevus is not visualized with FAF because it is posterior to the RPE.
Central serous chorioretinopathy (CSC) lends itself well to multimodal imaging due to the significant variability in clinical presentation, especially between the acute, chronic, and resolved forms of the disease. RPE atrophy can occur even after a relatively quick self-limiting case of CSC. These changes can be visualized with B-Scan OCT as mild degenerations of the RPE, but are more readily visualized with FAF. Areas of hypoautofluorescence represent areas of RPE atrophy while hyperautofluorescence denotes areas of metabolically stressed RPE that often times convert to atrophic regions. As opposed to the classic symptomatic central serous retinal detachment, CSC may also present extra-foveally without any reported symptoms. These cases are often incidental findings and may present as scattered RPE changes resulting from resolved serous detachments. The CLARUS 500 may be particularly useful in these cases because it combines ultra-widefield imaging with FAF to provide sweeping views of RPE dysfunction that is often understated with standard fundus photography or DFE.

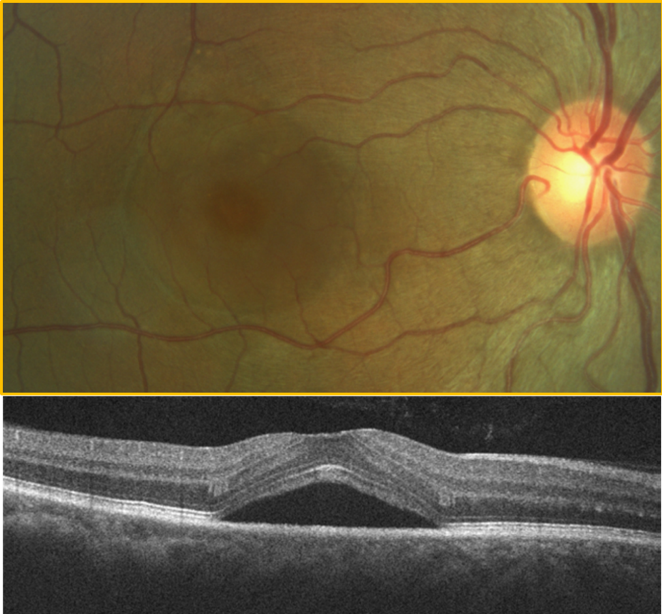
A serous retinal detachment secondary to CSC is noted with fundus photography and OCT.

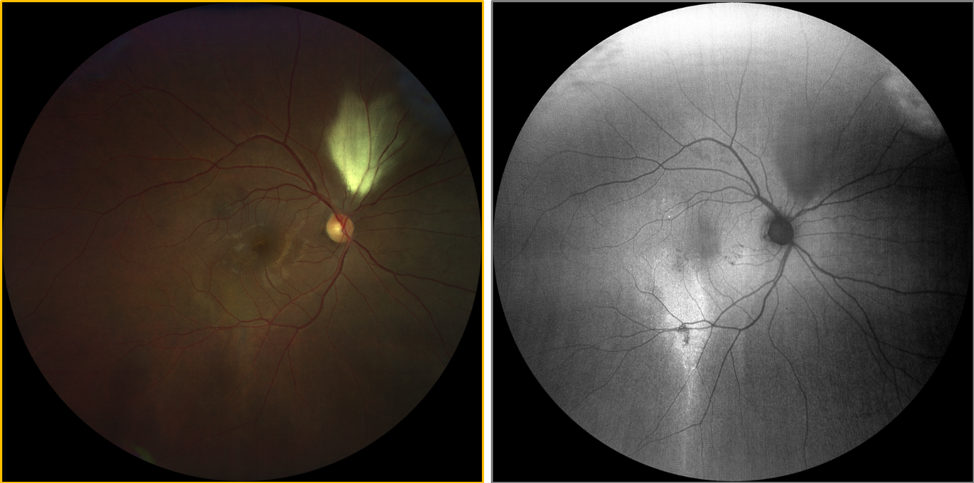
Multifocal retinal atrophy secondary to resolved CSC changes noted with color photography and widefield FAF. FAF reveals hyper-FAF, which is thought to indicate a metabolically active or “sick RPE.” The hypo-FAF areas represent signs of retinal atrophy. Note the area of RNFL myelination superior to the optic nerve head which masks the FAF signal causing relative hypo-FAF.

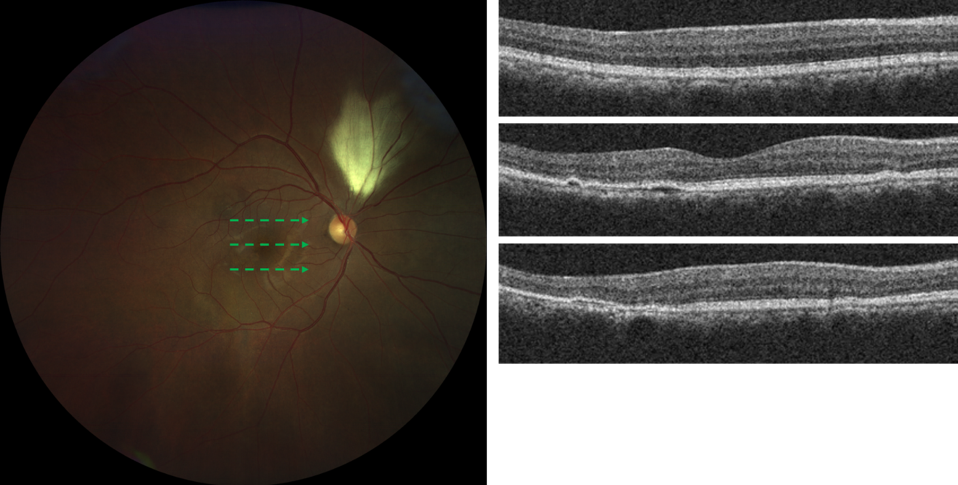
OCT B-scan images through three retinal loci showing varying amounts of outer retinal disease.

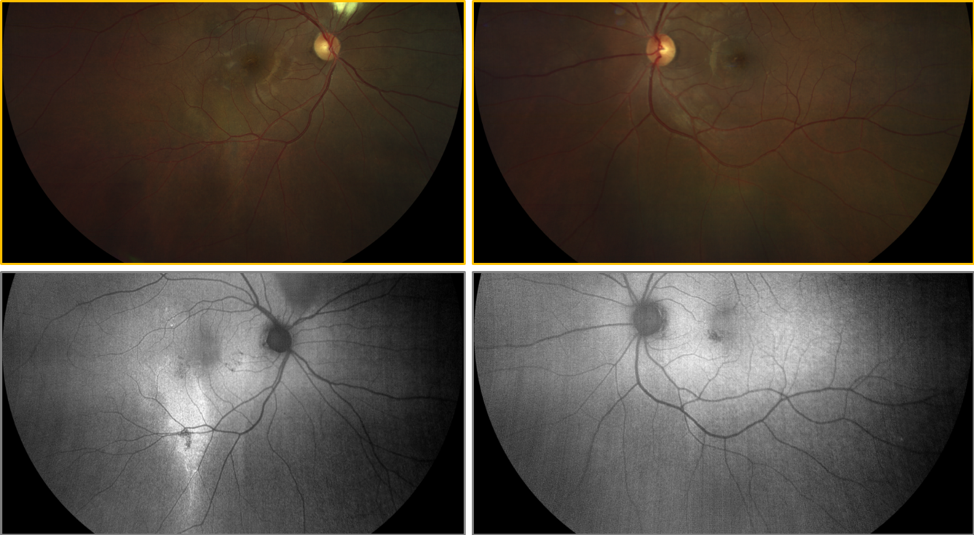
Widefield FAF of the fellow eye reveals mild hypo-FAF changes inferior-nasal to the foveal that are suggestive of retinal atrophy. Widefield FAF is preferred in these type of cases because these mild changes are often invisible to ophthalmoscopy and fundus photography.
Though diabetic retinopathy is classically thought to be a posterior pole disease, as mentioned above, recent studies have shown that hemorrhaging is frequently found peripherally as well. The ZEISS CLARUS 500 can image peripheral hemorrhaging but also provide high-quality images of the macula. These images can be zoomed in to evaluate the fovea for small microaneurysms. Serial high-quality images of the macula should be assessed for high microaneurysm turnover, as this has been shown to have a high-risk association with the development of diabetic macular edema.3 The presence of hemorrhages and cotton wool spots is important to document but the most common cause of vision loss in these patients is diabetic macular edema, which is significantly harder to document with fundus photography. In cases of suspected diabetic macular edema, OCT imaging can definitively rule out the presence of retinal thickening and prevent unnecessary referrals.

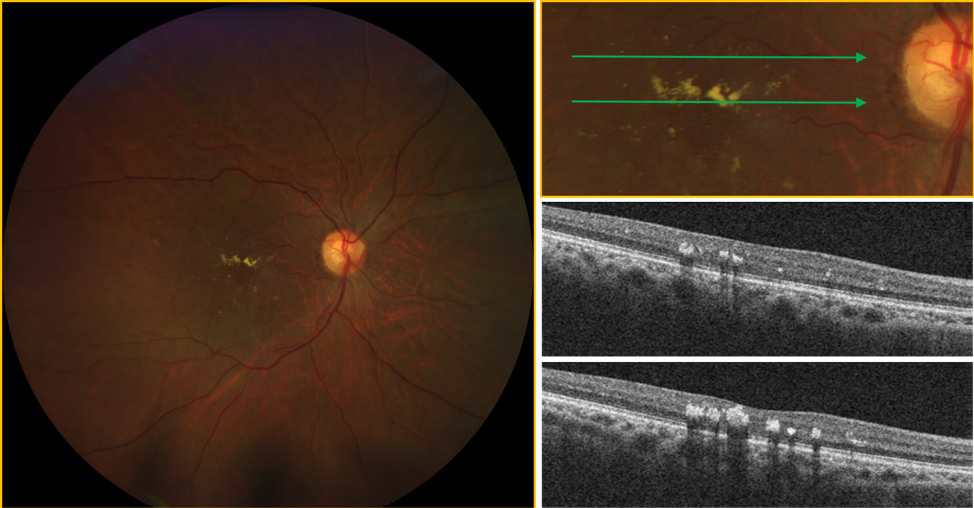
Widefield color image of diabetic retinopathy with exudation. OCT imaging confirms the exudation though there is no significant associated retinal thickening.

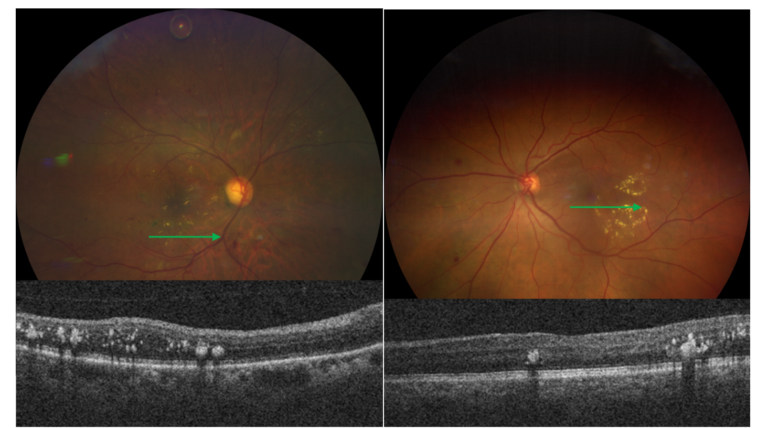
Widefield color images reveal diabetic retinopathy with exudation. On the left, anti-VEGF can be seen floating superiorly within the vitreous. OCT imaging confirms exudation and mild retinal thickening.
Chorioretinal scarring can create a diagnostic predicament for the eye care practitioner. Often times, the etiology of a chorioretinal scar is unknown and if the lesion looks inactive, not much concern is warranted. Without associated findings such as active uveitis, active vitritis, or hemorrhaging, chorioretinal scars are often monitored yearly. Using FAF capabilities, seemingly inactive lesions may appear to be metabolically active and perhaps require closer follow up. Because of its wide scan size, The ZEISS CLARUS 500 may visualize other lesions within the same eye or within the fellow eye that are difficult to visualize with DFE or color photography. Disseminated or bilateral retinal findings may change not only the prognosis but follow up and management of these patients.

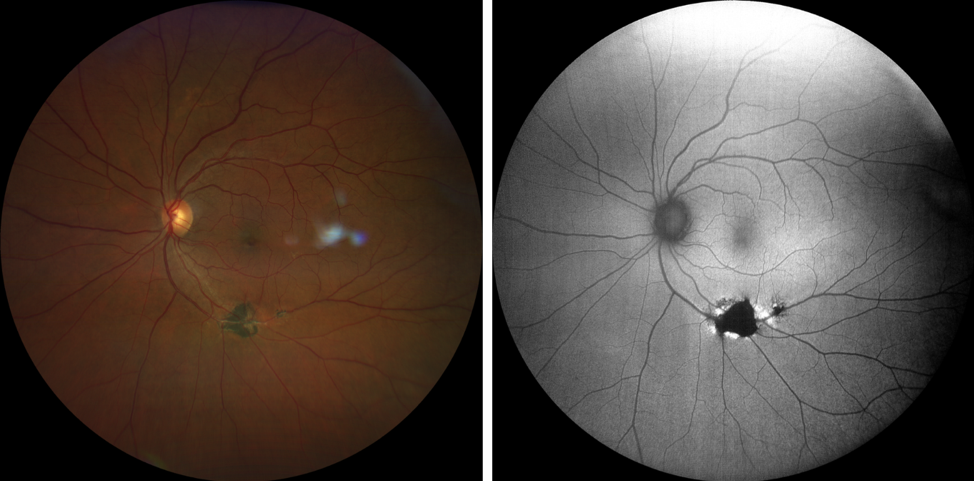
Widefield color imaging documents chorioretinal atrophy and widefield FAF imaging reveals hyper-FAF changes surrounding hypo-FAF changes, suggestive of an ongoing pathological process. Grayish lesions temporal the macular are vitreal opacities, likely secondary to a prior episode of vitritis.

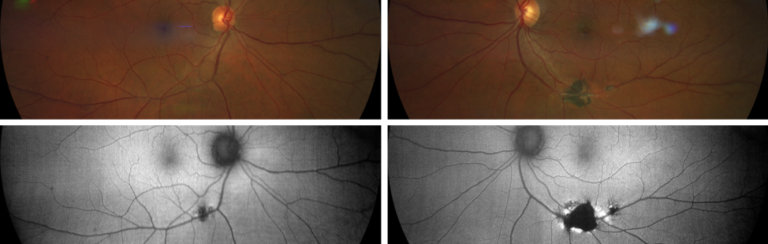
Widefield FAF imaging of the fellow eye reveals mild changes that were invisible to ophthalmoscopy and color imaging.
The differentiation of optic nerve head drusen from optic nerve head edema can often be a difficult clinical decision. Superficial optic nerve head drusen may be easy to distinguish with DFE or fundus photography but buried optic nerve head drusen are often difficult to appreciate. Unlike standard fundus photography, which has minimal utility in the differentiation of buried disc drusen from papilledema, FAF imaging can greatly aid in the visualization of buried disc drusen. Though devoid of lipofuscin, optic nerve head drusen are significantly hyperautofluorescent and easily imaged with FAF. Once identified, optic nerve head drusen must be monitored regularly due to possible compression of the RNFL and resultant atrophy that is very similar to glaucoma. Arcuate defects on visual field and RNFL thinning on OCT may occur even though there may be minimal cupping.4 As the atrophy progresses, optic nerve head pallor and non- glaucomatous cupping may appear. This progression can be monitored with OCT RNFL imaging, OCT ganglion cell analysis, and visual field testing. Though no accepted treatment for optic nerve head drusen exists at this time, some practitioners initiate ocular hypotensive treatment to prevent further damage.

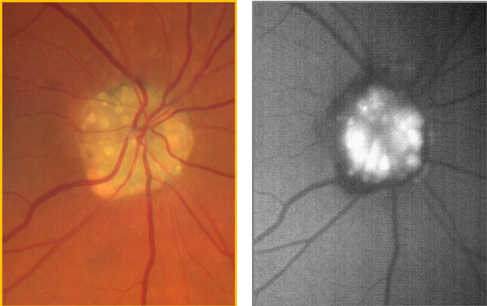
Numerous optic nerve head drusen are easily visualized with color photography. The optic nerve head drusen are noted as discrete areas of hyper-FAF.

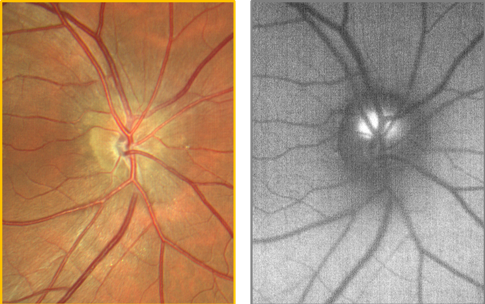
The optic nerve head drusen are not easily visualized with color imaging though a corresponding retinal nerve fiber layer is noted superior-temporally. FAF imaging easily visualizes the optic nerve head drusen, noted as discrete hyper-FAF round lesions.
Eye care practitioners are no longer managing retinal and optic nerve head disease based merely on appearance, but are using cutting-edge approaches to assess structure and function in a myriad of ways. The ZEISS CLARUS acquires high-quality, true color and FAF images of the posterior pole and retinal periphery. Together with OCT, OCTA and visual field testing, ZEISS offers a comprehensive suite of diagnostic devices to aid in detection and diagnosis of the full spectrum of ophthalmic diseases. In a world of decreasing reimbursement and busier patient schedules, the ZEISS CLARUS 500 aims to fulfill what ultra-widefield technology initially promised: high-quality imaging that improves patient care and office flow.
Sources:
- Silva, Paolo S., et al. “Nonmydriatic ultrawide field retinal imaging compared with dilated standard 7-field 35-mm photography and retinal specialist examination for evaluation of diabetic retinopathy.” American journal of ophthalmology 154.3 (2012): 549-559.
- Silva, Paolo S., et al. “Peripheral lesions identified on ultrawide field imaging predict increased risk of diabetic retinopathy progression over 4 years.” Ophthalmology 122.5 (2015): 949-956.
- Nunes, Sandrina, et al. “Microaneurysm turnover is a biomarker for diabetic retinopathy progression to clinically significant macular edema: findings for type 2 diabetics with nonproliferative retinopathy.” Ophthalmologica 223.5 (2009): 292-297.
- Auw-Haedrich, Claudia, Flemming Staubach, and Heinrich Witschel. “Optic disk drusen.” Survey of ophthalmology 47.6 (2002): 515-532.
CAM.10092 www.zeiss.com/us/med
The statements of the doctor who has written this white paper reflect only their personal opinions and experiences and do not necessarily reflect the opinions of any institution with whom they are affiliated. The doctor who has written this white paper has a contractual relationship with Carl Zeiss Meditec, Inc., and has received financial compensation.
© 2018 Carl Zeiss Meditec, Inc. All rights reserved. Only for sale in selected countries.
