



Just a note to start - I highly recommend purchasing The Netter Atlas of Human Anatomy. It has been HUGE for me to understand how all this stuff works. I still use it today as an OD, and it makes an AMAZING coffee table book that really freaks people out!


Anatomy of the Iris
- Sphincter Muscle: Contracts the pupil in a circular motion
- Dilator Muscle: Pulls the iris radially to enlarge the pupil, pulling it in folds.
- Back Surface: It is 2 cells thick and is covered by a heavily pigmented epithelial layer that is two cells thick (the iris pigment epithelium).
- Front Surface: has no epithelium, just fibrovascular pigmented tissue aka the stroma. Pigment granules here give color to the iris.
- Iris Root: The outer edge of the iris, is attached to the sclera and the anterior cilliary body.
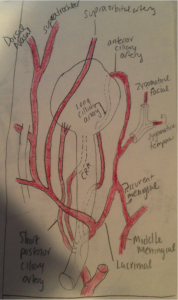
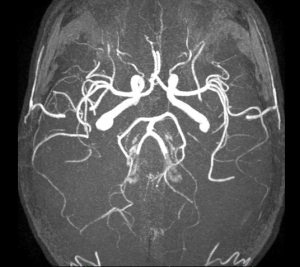
Vascular Supply to Iris
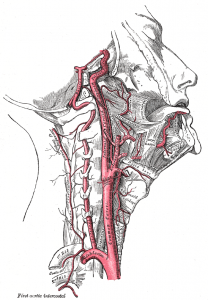
- Internal carotid artery comes up to the brain and the ophthalmic artery branches off of the internal carotid
- The long and short posterior cilliary artery’s branch off of the ophthalmic artery.
- LPCA’s and ACA’s divide in brach to form the major arterial circle of the iris which surrounds the outer iris. This then branches off to find the minor arterial circle which is closer to the pupil.
- On the way out the arteries transition to capillaries which transition to veins which run deep to the arteries.
- As the veins leave they also receive contribution from the cilliary body before heading to the large vortex veins and in inferior and superior ophthalmic vein.
The difference between the LPCA’s and SPCA’s is what they supply.
- LPCA’s –Iris, Cilliary Body, conjunctiva
- SPCA’s – Iris and Choroid

[adpress campaign=8]
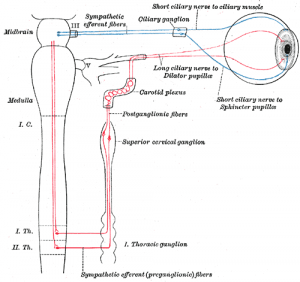
Sympathetic Innervation
- The first order (central) neuron descends from the hypothalamus to the first synapse in the cervical spinal cord
- The second order (preganglionic) neuron travels in the cervical sympathetic chain through the brachial plexus, over the pulmonary apex and synapses in the superior cervical ganglion. The superior cervical ganglion is located near the angle of the mandible and the bifurcation of the common carotid artery.
- The third order (postganglionic) neuron for the orbit enters the cranium within the adventitia of the internal carotid artery into the cavernous sinus. Here the oculosympathetic fibers exit the internal carotid.
- The fibers (long ciliary nerve) innervate the dilator muscles of the iris and the Müller’s muscle in the upper and lower lid.

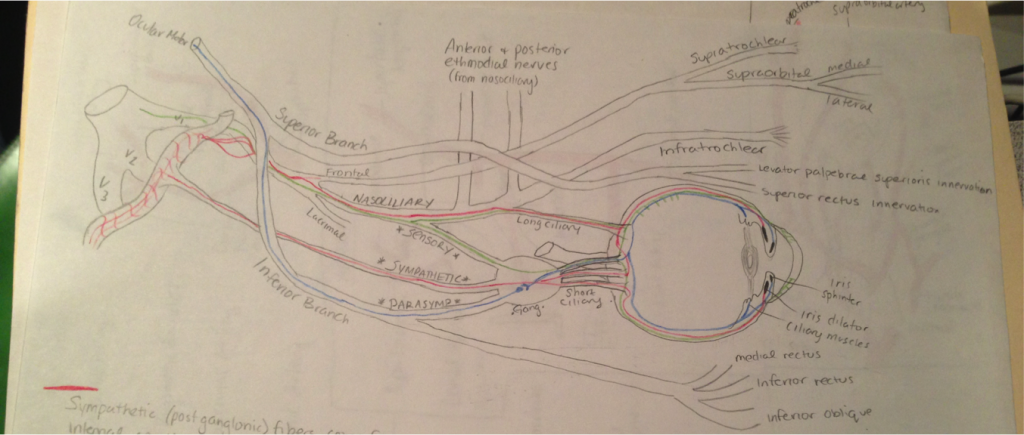
Sympathetic (post ganglionic) fibers come from the internal corotid artery. They can then take 2 roots to innervate the sphincter muscle. Root #1: TRIGEMINAL --> OPHTHALMIC --> NASOCILLIARY --> travel through the LONG CILLIARY nerve --> run into the iris sphincter. Root #2: Take a direct root directly through the SYMPATHEIC ROOT OF THE CILIARY GANGILON --> CILLIARY GANGLION --> SHORT CILLIARY NERVES --> IRIS SPHINCTER

Pharmacology
Pupil Dilator Muscle
- Sympathetic / Adrenergic = Alpha 1 = Dilation (mydrasis)
Iris Sphincter Muscle
- Parasympatheric / Muscarinic = M3 = Contraction (miosis)
Ciliary Muscle
- Sympathetic / Adrenergic = Beta 2 = Long-range focus
- Parasympatheric / Muscarinic = M3 = Close-up focus (accomodation)
The alpha-1 (α1) adrenergic receptor is a G protein-coupled receptor. Catecholamines like norepinephrine, epinephrine, and phenylephrine signal through the α1-adrenergic receptor in the central and peripheral nervous systems.
Anisocoria Information
- Pupils of 128 normal subjects in dim light, morning and afternoon, for five consecutive days
- 41% had an anisocoria of 0.4 mm or more at one time or another during these five days
- 3% had unequal pupils of 0.4 mm or more in all ten photography sessions
- At any given examination, a fairly constant 19% (24 of 128) of the subjects showed this amount of anisocoria
- The prevalence of anisocoria did not vary with the time of day, from day to day, or from week to week, nor was it influenced by the sex, age, or iris color of the subject
Causes of Anisocoria
- Physiological Anisocoria
- Mechanical Anisocoria
- Adie Pupil
- Horner's syndrome
- Inflammation
- CN III Palsy
- Angle-closure glaucoma
- Diabetes
- Syphilis
- Pharmacological Anisocoria
- Carotid Dissection
- Raeder Syndrome
- Wallenburg Syndrome
- Drugs - Pilocarpine, Cocaine, Tropicamide, MDMA (Ecstacy), Dextromethorphan (Cough suppressant), Scopolamine, Benzodiazapines (Xanax), Amphetamines (Adderal) NOT OPIODS LIKE MORPHENE
Horners Syndrome
Horner’s Syndrome indicates a problem with the sympathetic nervous system.


Horners Syndrome Symptoms
- Ipsilateral ptosis
- Ipsilateral miosis
- Sometimes ipsilateral anhidrosis
- Conjunctival injection
- Enophthalmos
- Loss of ciliospinal reflex (pupillary-skin reflex). This consists of dilation of the ipsilateral pupil in response to pain applied to the neck, face, and upper trunk. If the right side of the neck is subjected to a painful stimulus, the right pupil dilates (increases in size 1-2mm from baseline.
Types of Horner's Syndrome
- Wallenburg Syndrome
- Pancoast Tumor
- Carotid Dissection
- Raeder Syndrome
Horner's Syndrome: A Note On Pediatrics
Heterochromia is a difference in eye color between the two eyes. This happens because a lack of sympathetic stimulation in childhood interferes with melanin pigmentation of the melanocytes in the superficial stroma of the iris.


Horner's Syndrome Order
- First-order neuron disorder: Central lesions that involve the cervical spinal cord.
- Second-order neuron disorder: Pre-ganglionic like a lung tumor
- Third-order neuron disorder: Postganglionic lesions at the level of the internal carotid artery (e.g. a tumor in the cavernous sinus or a carotid artery dissection).
Horner's Syndrome Causes
- Lesion or compression of one side of the cervical or thoracic sympathetic chain
- Post surgical trauma (very common)
- Trauma to the base of neck
- Middle ear infection
- Tumors; Pancoast tumor on apex of lung
- Aortic aneurysm
- Thyroid carcinoma
- Multiple sclerosis
- Carotid artery dissection
- Cavernous sinus thrombosis
- During a migraine attack
How To Diagnose Horner's Syndrome
(Is there Horners or not?)
- 10% Cocaine eyedrops block the reuptake of norepinephrine resulting in the dilation of a normal pupil. However, in Horner's syndrome the lack of norepinephrine in the synaptic cleft causes mydriatic failure.
Or use
- alpha-agonist 0.5% apraclonidine (alpha 2 agonist) to both eyes and observe the increased mydriatic effect (due to hypersensitivity) on the affected side of Horner syndrome (the opposite effect to what the cocaine test would produce in the presence of Horner's).
How To Diagnose Horner's Syndrome
(Is it a pre or post ganglionic lesion?)
- Topical 1% Hydroxyamphetamine causes a release of norepinephrine from intact adrenergic nerve endings causing pupillary dilation.
- One hour after instillation of 1% hydroxyamphetamine, dilation of both pupils indicate a lesion of the 1st or 2nd order neuron.
- If the smaller pupil fails to dilate it indicates a lesion of the 3rd order or postganglionic neuron.
Horners Syndrome Etiology
- Of 450 cases of Horner's syndrome examined by pupillography. 13% were caused by tumor but less than 3% were undetected malignant tumors.
- The largest group of lesions (40%) had an undetermined cause, presumably related to vascular disease.
- Hydroxyamphetamine test usually can differentiate postganglionic from preganglionic lesions, its clinical value and accuracy for this purpose has been overemphasized in previous reports.
- Of the 13 undetected malignant neoplasms, nine (69%) manifested as Pancoast's syndrome with arm pain, a reliable sign to identify patients with Horner's syndrome caused by undetected malignancy.
Wallenburg’s Syndrome
THIS IS A 1st ORDER HORNER’S
Also known as...
- Lateral medullary syndrome
- Wallenberg syndrome
- Posterior inferior cerebellar artery syndrome
- A disease in which the patient has a constellation of neurologic symptoms due to injury to the lateral part of the medulla in the brain, resulting in tissue ischemia and necrosis.

Wallenburg’s Syndrome Symptoms
- Sensory deficits affecting the trunk and extremities on the opposite side of the infarction
- Sensory deficits affecting the face and cranial nerves on the same side with the infarct.
- Specifically, there is a loss of pain and temperature sensation on the contralateral side of the body and ipsilateral side of the face.
- This crossed finding is diagnostic for the syndrome.
- Symptoms Include - Dysphagia, slurred speech, ataxia, facial pain, vertigo, nystagmus, Horner syndrome, diplopia.
Wallenburg’s Syndrome Causes
- Occlusion of the posterior inferior cerebellar artery (PICA) or one of its branches
- Occlusion of the vertebral artery
- The most commonly affected artery is the vertebral artery, followed by the PICA, superior middle and inferior medullary arteries.

Wallenburg’s Syndrome Treatment
- Treatment for lateral medullary syndrome involves focusing on relief of symptoms and active rehabilitation to help those suffering from the stroke syndrome recover their activities of daily living and cope with neurologic loss that can be psychologically devastating.
- One of the most unique and difficult to treat symptoms that occur due to Wallenberg syndrome are interminable, violent hiccups. Depending on the severity of the blockage caused by the stroke, the hiccups can last for weeks.
- Long term treatment generally involves the use of antiplatelets like aspirin or clopidogrel and statin regimen for the rest of their lives in order to minimize the risk of another stroke.
- Treatment for this disease can be disconcerting because some individuals will always have residual symptoms due to the severity of the blockage.
- Two patients may present with the same initial symptoms right after the stroke has occurred, but after several months one patient may fully recover while the other is still severely handicapped.
Pancoast Tumor
THIS IS PRE-GANGLIONIC 2nd ORDER HORNER’S
It is a type of lung cancer defined primarily by its location situated at the top end of either the right or left lung. The growing tumor can cause compression of…
- brachiocephalic vein
- subclavian artery
- phrenic nerve
- recurrent laryngeal nerve
- vagus nerve
- sympathetic ganglion resulting in Horner's syndrome.
Pancoast Tumor Symptoms
Other than horner’s syndrome..
- Arm and shoulder pain
- Frequently radiating down the arm (especially the inside part of the arm)
- Weakness in hand muscles
- Tingling and prickly sensations in the hand,(especially the ring and pinky fingers)
- These tumors are less likely to have typical lung cancer symptoms, such as shortness of breath and coughing.
Pancoast Tumor Diagnosis
- Pancoast tumors are also difficult to see on chest x-rays due to their location.
- A combination of CT scans and MRI (to look for nerve involvement) is often done.
- Then a biopsy to confirm the diagnosis.
Pancoast Tumor Treatment
- Surgery is difficult because of the tumors close proximity to vital structures (such as nerves and spine).
- Treatment may involve radiation and chemotherapy. Surgery may consist of the removal of the upper lobe of a lung together with its associated structures (subclavian artery, vein, branches of the brachial plexus, ribs and vertebral bodies), as well as mediastinal lymphadenectomy.
- Pancoast tumors have a better prognosis than tumors that are located more centrally in the lungs.
- Survival rate may be better than other cancers at a similar stage.
- The 5-year survival rate for pancoast tumors overall is around 30%.
Carotid Dissection
THIS IS 3rd ORDER POST-GANGLIONIC HORNERS
- Carotid artery dissection is a separation of the layers of the artery wall supplying oxygen-bearing blood to the head and brain, and is the most common cause of stroke in young adults.
- 70% of patients with carotid arterial dissection are between the ages of 35 and 50, with a mean age of 47 years.
Source - Amal Mattu; Deepi Goyal; Barrett, Jeffrey W.; Joshua Broder; DeAngelis, Michael; Peter Deblieux; Gus M. Garmel; Richard Harrigan; David Karras; Anita L'Italien; David Manthey (2007). Emergency medicine: avoiding the pitfalls and improving the outcomes. Malden, Mass: Blackwell Pub./BMJ Books. p. 46

Carotid Dissection Causes
- Spontaneous Carotid artery dissection
- May have a history of stroke in their family and/or hereditary connective tissue disorders, such as Marfan syndrome, Ehlers-Danlos syndrome, pseudoxanthoma elasticum, fibromuscular dysplasia, and osteogenesis imperfecta type I.
- Most people with spontaneous arterial dissections do not have associated connective tissue disorders.
- Traumatic Carotid artery dissection - Severe violent trauma to the head and/or neck.
An estimated 0.67% of patients admitted to the hospital after major motor vehicle accidents were found to have blunt carotid injury. - Fabian, TC, Patton, Joe, Croce, Martin, Minard, Gayle, Kudsk, Kenneth, Pritchard, F. (1996). "Blunt Carotid Injury". Annals of Surgery 223 (5): 513–52
The probable mechanism of injury for most internal carotid injuries is rapid deceleration, with resultant hyperextension and rotation of the neck, which stretches the internal carotid artery over the upper cervical vertebrae, producing an intimal tear. - Matsuura, JH, Rosenthal, D, Jerius, H, Clark, MD, Owens, DS (1997). "Traumatic Carotid Artery Dissection and Pseudoaneurysm Treated With Endovascular Coils and Stent". Journal of Endovascular Surgery 4 (4): 339–343.
Small tear forms in the innermost lining of the arterial wall --> Blood is then able to enter the space between the inner and outer layers of the vessel --> causing narrowing (stenosis) or complete occlusion. Blood clots form and break off from the site of the tear --> they form emboli--> travel through the arteries to the brain and block the blood supply to the brain --> resulting in an ischaemic stroke (infarction).
Carotid Dissection Symptoms
Divided into ischemic and non-ischemic categories:
Non-ischemic signs and symptoms Headache or neck pain Horner syndrome Ischemic signs and symptoms Transient vision loss Ischemic stroke
Carotid Dissection Treatment
- Observation
- Anticoagulation
- Stent implantation
- Carotid artery ligation
Raeder Syndrome
THIS IS 3rd ORDER POST-GANGLIONIC HORNERS
- Simply this is a NUMB and PAINFUL horner’s pupil.
- The pathophysiologic site of the painful horner’s involves the location at which sympathetic fibers exit the internal carotid artery to join the ophthalmic division of the trigeminal nerve.
- It localizes to lesions of the middle cranial fossa involving sympathetic fibers originating from the internal carotid and traveling with the trigeminal and oculomotor nerves.
Raeder Syndrome Causes
- Head trauma
- Hypertension
- Vasculitis
- Migraine headaches
- Parasellar mass lesions
- Internal carotid artery dissection
- Internal carotid aneurysm
Raeder Syndrome Symptoms
MAINLY - unilateral facial pain and headache with ipsilateral Horner syndrome.
- Consists of facial pain and numbness - deep and boring and is localized in or around the eye.
- It occurs on one side of the face, usually centered around the cheek and eye.
- Sweating is preserved in Raeder syndrome, in contrast to Horner syndrome, since some third-order sympathetic fibers are spared.
Raeder Syndrome Management
- Diagnosis should be made using radiological imaging (MRI and MRA).
- Basic laboratory analysis to evaluate for inflammatory or infectious etiologies also may be warranted.
- A basic chemistry profile, a complete blood count (CBC), the erythrocyte sedimentation rate, antinuclear antibody, and rheumatoid factor may be helpful in screening for inflammatory or infectious causes.
- Pain medication, HA medication, muscle relaxers may be used, but really one must Tx the underlying cause.
Raeder Syndrome Prognosis
- Symptomatic resolution in Raeder’s usually occurs within an interval of 2-3 months.
- If pain persists or if atypical features are noted, investigate and manage secondary causes.
- Morbidity and mortality depend on the underlying etiology, and the diagnosis of the condition warrants a full evaluation to identify an underlying cause.
POCKET GUIDE TO HORNERS SYNDROME
1st Order / Central Lesion
- TYPE - Wallenburg Syndrome
- SYMPTOMS - A loss of pain and temperature sensation on the contralateral side of the body and ipsilateral side of the face
- CAUSES - Occlusion of PICA or Vertebral Artery
2nd Order / Pre-Ganglionic
- TYPE - Pancost Tumor
- SYMPTOMS - Paresthesia’s and pain running down the arm and hand
- CAUSES - Tumor on Apex of lung pressing on sympathetics
3rd Order / Post-Ganglionic
- TYPE - Carotid Dissection
- SYMPTOMS - Headache / neck pain –or- Transient vision loss or stroke
- CAUSES - Trauma, surgery, spontaneous, collagen vascular disease
- TYPE - RAEDER SYNDROME (Traumatic or spontaneous)
- SYMPTOMS - Numb and painful horners within the face only
- CAUSES - Caused by underlying general systemic disease
SOURCES
- Gold, Daniel H; Lewis, Richard; "Clinical Eye Atlas," pp. 396-397
- Leonard A Levin, Siv F. E. Nilsson, James Ver Hoeve, Samuel Wu, Paul L. Kaufman, Albert Alm; “Adler’s Physiology of the Eye”
- Am J Ophthalmol. 1987 Jul 15;104(1):69-73.The prevalence of simple anisocoria. Lam BL, Thompson HS, Corbett JJ.
- London, Richard; Ellen Richrer Erringer, Harry J. Wyafr, (March 1991). "Variation and Clinical Observation With Different Conditions of Illumination and Accommodation". Investigative Ophthalmology & Visual Science, 32 (3): 501–9.
- "Angel's Trumpet (Brugmansia arborea) and mydriasis in a child - A case report", Bulletin de la Societe Belge d'Ophtalmologie 292: 53–56, ISSN 0081-0746
- Am J Ophthalmol. 1980 Sep;90(3):394-402. Evaluation of the causes and accuracy of pharmacologic localization in Horner's syndrome. Maloney WF, Younge BR, Moyer NJ.
- a b wallenbergs at NINDS http://www.healthline.com/galecontent/wallenberg-syndrome
- Khedr E, Abo-Elfetoh N (October 2009). "Therapeutic role of rTMS on recovery of dysphagia in patients with lateral medullary syndrome and brain stem infarction". J. Neurol. Neurosurg. Psychiatr. 81 (5): 495–499. doi:10.1136/jnnp.2009.188482. PMID 19828479.
- Paulson DL, Shaw RR (May 1960). "Results of bronchoplastic procedures for bronchogenic carcinoma". Ann. Surg. 151: 729–40. PMC 1613696. PMID 14431029.
- Dartevelle PG, Chapelier AR, Macchiarini P, et al. (June 1993). "Anterior transcervical-thoracic approach for radical resection of lung tumors invading the thoracic inlet". J. Thorac. Cardiovasc. Surg. 105 (6): 1025–34. PMID 8080467.
- Nazari S (August 1996). "Transcervical approach (Dartevelle technique) for resection of lung tumors invading the thoracic inlet, sparing the clavicle". J. Thorac. Cardiovasc. Surg. 112 (2): 558–60. PMID 8751536.Grunenwald D, Spaggiari L (February 1997). "Transmanubrial osteomuscular sparing approach for apical chest tumors". Ann. Thorac. Surg. 63 (2): 563–6. doi:10.1016/S0003-4975(96)01023-5. PMID 9033349.
- Rusch, V. Management of Pancoast Tumors. Lancet Oncology. 2006. 12:997-1005.
- Shen, K. et al. Special Treatment Issues in Lung Cancer. ACCP Evidence-Based Clinical Practice Guidelines (2nd Edition). Chest. 2007. 132(no. 3 suppl):290S-305S.
- a b Amal Mattu; Deepi Goyal; Barrett, Jeffrey W.; Joshua Broder; DeAngelis, Michael; Peter Deblieux; Gus M. Garmel; Richard Harrigan; David Karras; Anita L'Italien; David Manthey (2007). Emergency medicine: avoiding the pitfalls and improving the outcomes. Malden, Mass: Blackwell Pub./BMJ Books. p. 46. ISBN 1-4051-4166-2.
- Mount Sinai Hospital Patient Care Health Library: http://www.mshq.org/patient-care/health-library/diseases-and-conditions/aortic-dissection
- Kerry, R, Taylor, AJ (2006). "Cervical arterial dysfunction assessment and manual therapy". Manual therapy 11 (4): 243–53. doi:10.1016/j.math.2006.09.006. PMID 17074613.
- In: Neurology 2006;67:1809-1812. Mokri, B. (1997). "Spontaneous dissections of internal carotid arteries". Neurologist 3 (2): 104–119. doi:10.1097/00127893-199703000-00005
- Surv Ophthalmol. 1980 Jan-Feb;24(4):199-210.Raeder's syndrome. A clinical review.Grimson BS, Thompson HS.
- Fabian, TC, Patton, Joe, Croce, Martin, Minard, Gayle, Kudsk, Kenneth, Pritchard, F. (1996). "Blunt Carotid Injury". Annals of Surgery 223 (5): 513–52.doi:10.1097/00000658-199605000-00007.
- Matsuura, JH, Rosenthal, D, Jerius, H, Clark, MD, Owens, DS (1997). "Traumatic Carotid Artery Dissection and Pseudoaneurysm Treated With Endovascular Coils and Stent". Journal of Endovascular Surgery 4 (4): 339–343.
- Amal Mattu; Deepi Goyal; Barrett, Jeffrey W.; Joshua Broder; DeAngelis, Michael; Peter Deblieux; Gus M. Garmel; Richard Harrigan; David Karras; Anita L'Italien; David Manthey (2007). Emergency medicine: avoiding the pitfalls and improving the outcomes. Malden, Mass: Blackwell Pub./BMJ Books. p. 46. ISBN
Do you have any questions about this? Our entire team will help you if you post in the comments below! You will need to register or login.
The author of the content you just read, put in lots of work to provide you with this article. Even though we try our best, there is no guarantee the article is error free. NewGradOptometry.com, its sponsors, advertisers, staff and writers make no representation, warranty, or guarantee that this article and its contents are error-free and will bear no responsibility or liability for the results or consequences of the information contained within.
