


Glaucoma is a group of optic neuropathies characterized by progressive retinal ganglion cell (RGC) atrophy with resultant distinctive structural and functional damage to the optic nerve. Although the exact mechanism of disease has not been completely elucidated, our understanding of the diagnosis and treatment of glaucoma has grown tremendously in the past few decades. Recent epidemiological studies have shown that though primary open angle glaucoma (POAG) is still responsible for the majority of glaucoma worldwide, angle closure glaucoma (ACG) is much more common than once thought. Investigations of the site of damage in glaucoma have renewed interest in evaluation of the macula in all stages of glaucoma.
As our knowledge of glaucoma has evolved, so have our tools; optical coherence tomography (OCT) has continued to add diagnostic parameters to aid in the detection and management of glaucoma.
Make sure you read this in-depth overview on utilizing OCT to treat and manage retinal pathology.
OCT for glaucoma was initially utilized for the evaluation of the retinal nerve fiber layer (RNFL) thickness.
This was a new parameter that was objective and highly reproducible which could be acquired quickly in most patients. Though not found in any of the classic landmark glaucoma studies, RNFL thickness as evaluated by OCT has become one of the gold standards in the management of glaucoma. The widespread use of OCT RNFL thickness measurements is due in part to a very high sensitivity and specificity of 87% and 92% combined with an inherent variability of merely 2.67%.1,2
The RNFL thickness is measured in a circular path of 3.46 mm diameter centered on the optic nerve head (ONH) and then analyzed as quadrants, clock hours, or a TSNIT curve. The individual eye is compared against a normative database and comparative statistics are calculated. This analysis is part of the RNFL and ONH:Optic Disc Cube and is the glaucoma workhorse of the Zeiss Cirrus OCT.

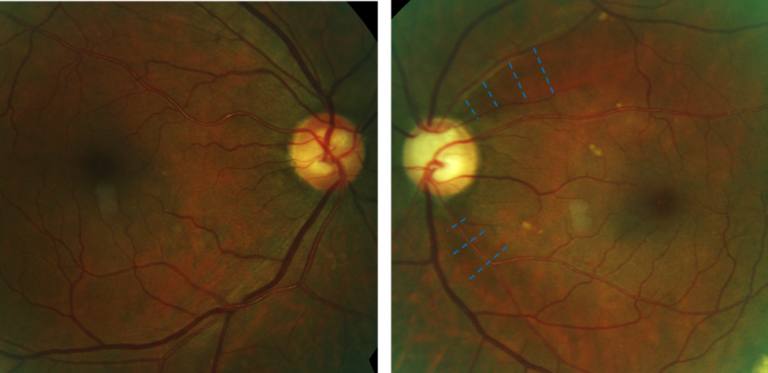
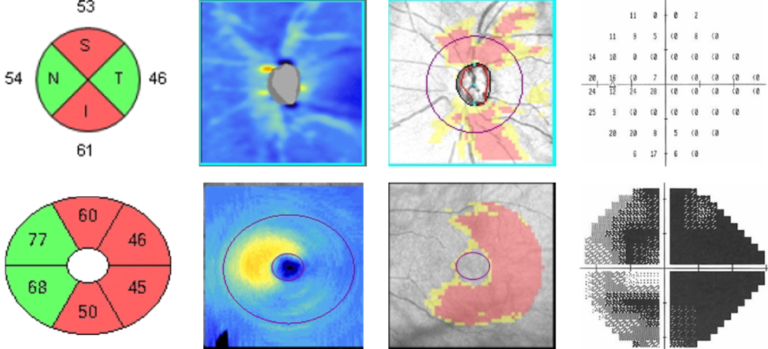
1a. Fundus photography reveals RNFL wedge defects superior-temporally and inferior-temporally of the left eye. The RNFL defects are consistent with the larger cup OS.

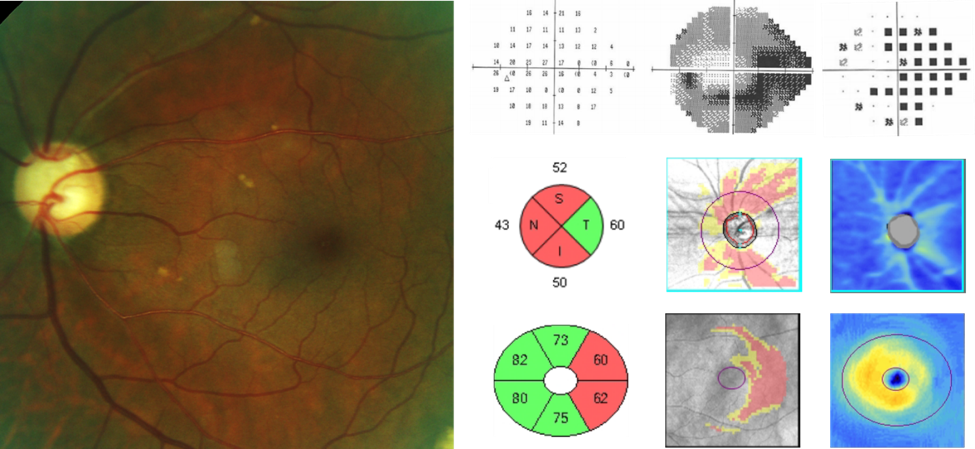
1b. Glaucomatous loss revealed with visual field testing, RNFL GCA measurements.

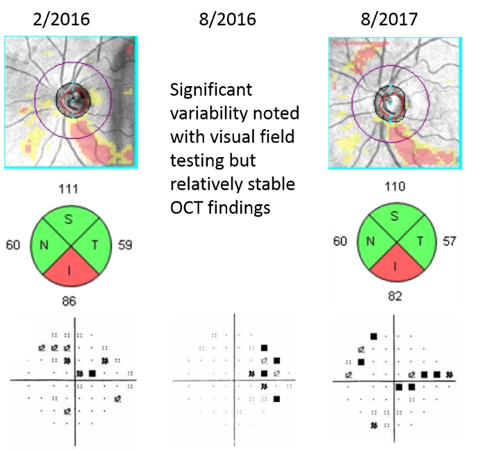
- Significant variability noted with visual field testing but the RNFL OCT findings remain relatively stable.
Although it is easy to glance at the quadrant and clock hour representations and quickly obtain significant information about the structure of the ONH, the TSNIT curve displays 256 data points that are plotted on the circular path around the ONH. The TSNIT curve display is a plot of all the data from which the quadrant and clock hour displays are derived. Focal changes or interocular asymmetries that might be difficult to appreciate using the quadrant or clock hour displays can be readily noted with the TSNIT curve display.

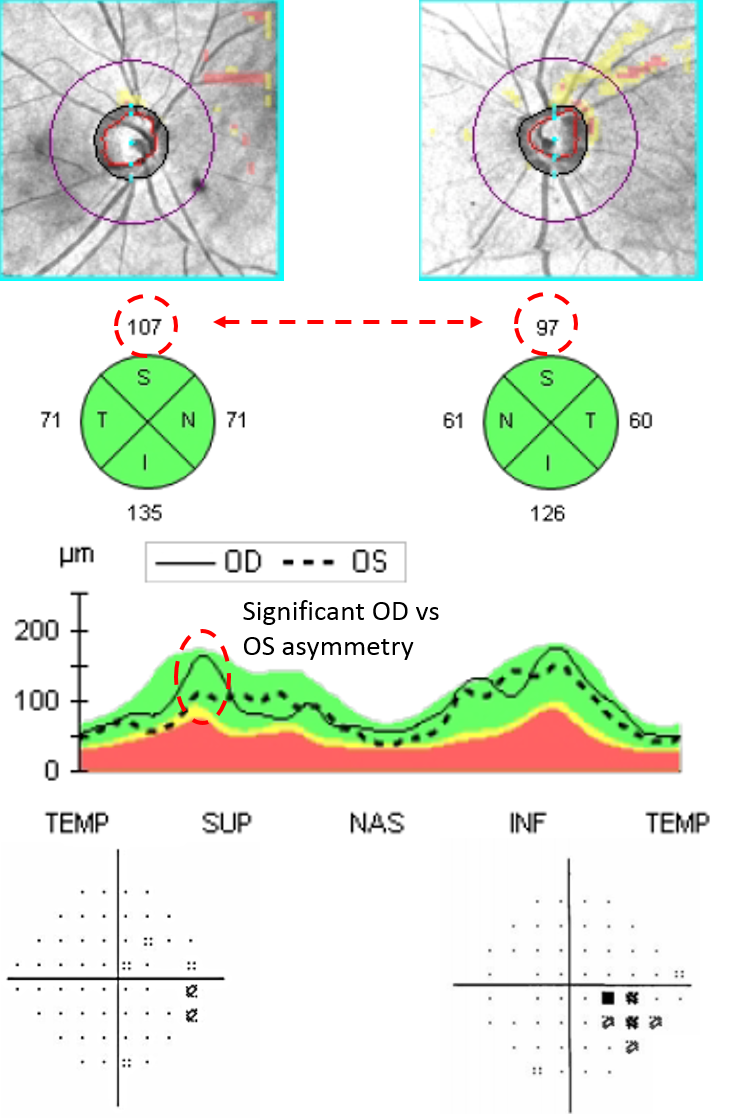
- Significant superior RNFL asymmetry noted on the TSNIT curve yet the corresponding quadrants are both green. Visual field testing reveals corresponding field loss.
Unlike some other platforms which utilize OCT for glaucoma, the Zeiss Cirrus OCT also has the capability to study the RNFL in a 6×6 mm area centered on the ONH. The RNFL deviation map has been found to be more sensitive in detecting RNFL defects than the quadrant or clock hour analysis alone.3
Want more content dedicated to ocular disease? Check out our medical optometry resource page for tons of clinical cases and images and information on using OCT and ultra-widefield imaging.
Leung, Weinreb, et al have shown that 18% of patients with mild glaucoma have RNFL defects close to the ONH within the 3.46 mm diameter and are therefore undetectable with the quadrant and clock hour analysis.4 Evaluation of the RNFL deviation map has been demonstrated to outperform the conventional quadrant and clock hour analysis, increasing the Zeiss Cirrus OCT sensitivity and specificity to 95% and 95.1% in the detection of glaucoma.3

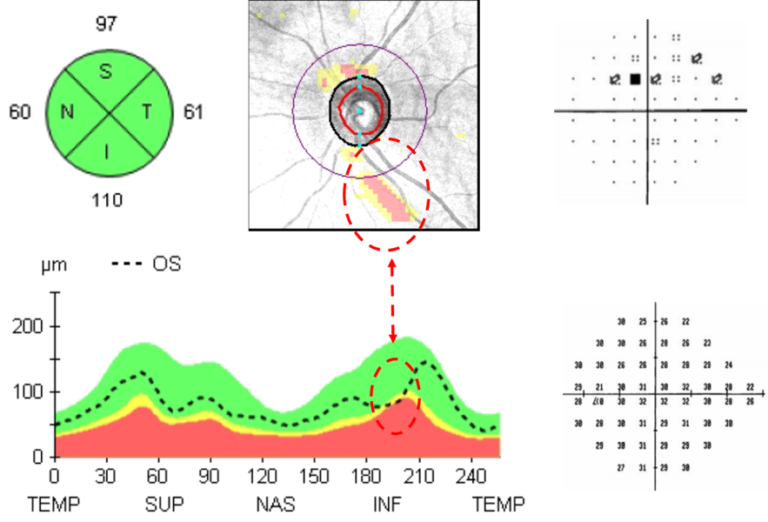
4. The RNFL deviation map reveals significant RNFL loss which is not noted on the quadrant analysis. Visual field testing reveals corresponding field loss.
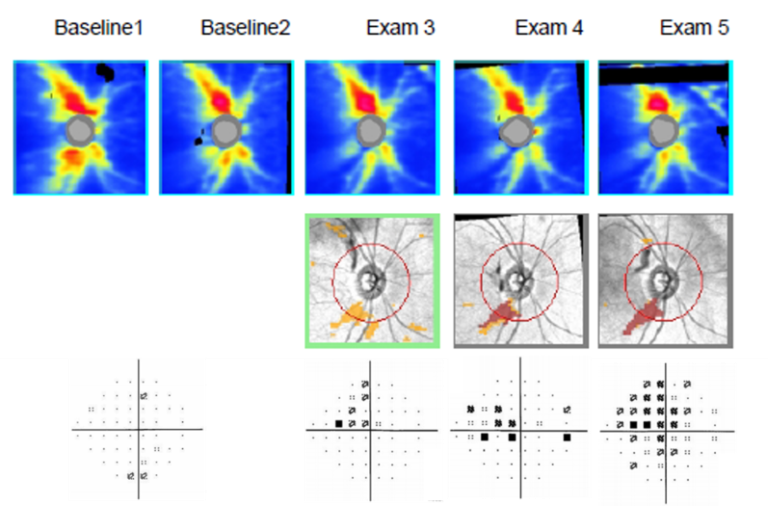
Due to the progressive nature of glaucoma, change from baseline is an important indicator in the detection of disease.
Consider a patient with a RNFL thickness that is 20% thicker than the normal range of the normative database. This patient can experience a 15% loss of RNFL thickness and still be considered normal in relation to the OCT database. For this reason, as with any glaucoma parameter, it is important to compare serial examinations against the baseline. Similar to the progression analysis of the Humphrey Visual Field, the Zeiss Cirrus also has progression analysis software that can reveal glaucomatous damage. The ONH/RNFL Guided Progression Analysis (GPA) creates a baseline from two ONH/RNFL scans and then compares all subsequent scans to this baseline; images are corrected for rotation so that proper comparisons can be made. Changes in RNFL thickness are only flagged if they are greater than the expected inter-scan variability. When using the GPA report, one must be mindful of the floor effect with OCTs. The floor effect is the measurement minimum, at which the RNFL thickness will no longer decrease though the disease process will continue. An eye with a visual field mean deviation of approximately -22dB will reach the measurement minimum of approximately 57 μm (these numbers apply specifically to the Cirrus OCT) at which point the RNFL thickness may no longer decrease but the eye will continue to lose vision, eventually reaching complete blindness.5 This effect is due in part to proliferation of glial tissue and the presence of non-axonal tissue such as blood vessels within the scan locus. For this reason, perimetry is the preferred method for monitoring more advanced stages of glaucoma. Another caveat in RNFL progression analysis is the discordance in rate of change of functional and structural testing, care should be taken when comparing progression between different modalities.

Glaucomatous damage of the macula has classically been thought to occur only in the advanced stages of the disease though investigators had published evidence to the contrary dating back to at least 1969.6,7,8
There has been recent interest in the glaucomatous damage of the macula as eye care professionals labor towards diagnosing glaucoma earlier and with greater accuracy. The macula has the highest density of RGCs, containing over 30% of the total population of RGCs in an area representing less than 2% of the retina.9 Due to this tremendous population of RGCs, it is thought that early atrophy can be noted earlier than in more peripheral regions. The Zeiss Cirrus OCT for glaucoma allows evaluation of the macular RGCs with the Ganglion Cell Analysis. This analysis is part of the 512 x 128 Macular Cube Scan and segments the RGC layer and inner plexiform layer creating a sectoral display similar to the RNFL quadrant analysis. Thinning of the GCA occurs most often on the temporal side and is more common in glaucoma with central or paracentral visual field defects. Investigations by Hood et al have demonstrated that an inferior paracentral region, that projects to an area dubbed the Macular Vulnerability Zone, is more likely to be affected by glaucoma than the superior paracentral region.10 The exact etiology for this preponderance is still unknown but since central visual fields are not commonly completed in clinical practice, examination of the Macular Vulnerability Zone can help detect glaucomatous damage. The Macular Vulnerability Zone can also be evaluated by looking at the RNFL thickness in the inferior-temporal region; defects in this area are most easily evident when analyzing the TSNIT curve. It is still unclear what role the detection of macular glaucomatous damage plays within the overall management of glaucoma, but leading experts agree that RGC measurements are complementary to RNFL measurements.
A promising role for GCA can be found in a recent investigation that found the measurement floor for GCA thickness to be lower than that of RNFL thickness, allowing for valid measurements in the advanced stages of glaucoma.11

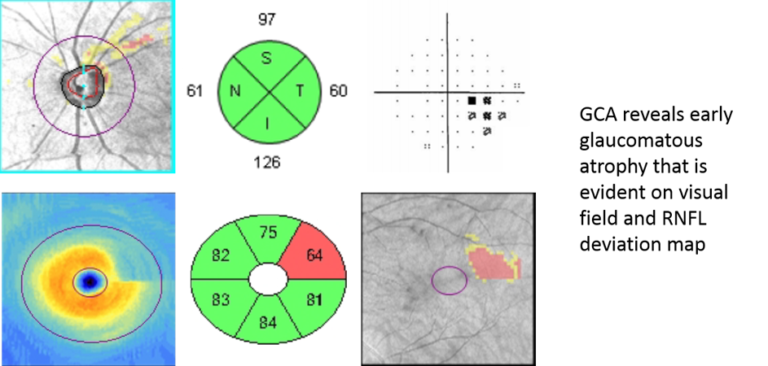
6. GCA reveals early glaucomatous atrophy that is evident with visual field testing and the RNFL deviation map. The quadrant analysis is not flagged but a significant superior vs inferior asymmetry is noted.
(Different patient below)

7. Concordant RNFL, GCA, and VF loss. Note that the GCA loss is more prominent on the temporal side of the fovea.
Similar to the ONH/RNFL GPA report, the GCA protocol has a progression analysis which compares serial images to a baseline of two scans. As previously discussed, glaucoma is a progressive disease and thus continuous atrophy is the hallmark indicator of structural loss. Due to the lower measurement floor of the GCA relative to RNFL thickness, the macula may be better suited for the evaluation of progression into advanced disease.12 Though perimetry is the gold standard in monitoring for progression in advanced disease and is unlikely to be replaced anytime soon but GCA progression analysis does offer several advantages to perimetry. Unlike visual fields which tend to have greater variability as the disease progresses, imaging of the macula is not affected by disease stage.12,13 Due to the nature of the perimetry protocol (SITA) used by most practitioners, a visual field will often take longer to finish as the disease progresses; imaging of the macula does not encounter this problem.13
Evaluation of the angle is imperative to the management of glaucoma.
It is impossible to accurately treat glaucoma without knowing the status of the iridocorneal angle. Nevertheless, investigators have found that in several cohorts, about half of glaucoma patients being treated do not have a recorded gonioscopic result.14,15 Clinicians may veer away from gonioscopy due to patient discomfort or inherent performance difficulty. The need for careful gonioscopic evaluation of all glaucoma patients and suspects has been reinforced by recent epidemiological studies showing that angle closure glaucoma is more common than was once thought. Approximately 80 million people will have glaucoma by 2020, with 36% having angle closure.16 There are significant racial predilections in the types of glaucoma, with Asian patients tending to have angle closure glaucoma and non-Asians manifesting the open angle form. Though less common, angle closure glaucoma is more likely to cause blindness with 47% of all cases of blindness due to glaucoma arising from angle closure.16 The gonioscopic evaluation of the iridocorneal angle gives a plethora of information that is invaluable in the distinction between open and closed angle glaucoma. Though not a replacement, when using OCT for glaucoma diagnosis and management, it can aid in the detection of angle closure and does provide several novel parameters which cannot be evaluated with gonioscopy.

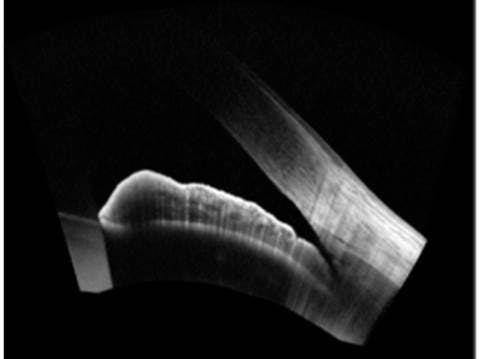
8. A high resolution of a narrow but open angle.
The iridocorneal angle can be imaged with the Zeiss Cirrus OCT using the Anterior Chamber Analysis which gives a cross sectional view of the whole anterior segment or the Wide Angle-to-Angle Analysis and HD Angle scans which allow for a higher resolution image of the iridocorneal angle. Though no standardized criteria for the evaluation of angle closure with OCT exists, many experts define an angle as closed on anterior segment OCT if iridocorneal touch anterior to the scleral spur is noted. The scleral spur is the most readily identified structure of the iridocorneal angle with OCT and is often used as a landmark in the evaluation of angle closure. Any irido contact anterior to the scleral spur with OCT is presumed to be comparable to an angle in which the posterior trabecular meshwork is not identified with gonioscopy. Using gonioscopy as the standard reference, a study by Nolan et al found that OCT correctly identified 98% of patients with angle closure.17 Though very sensitive, OCT was found to have a rather low specificity of 55%.17 The significant discrepancy in sensitivity and specificity was thought to be due to a difference in illumination conditions, anterior segment distortion during gonioscopy, and dissimilar criteria of angle closure between OCT and gonioscopy. When evaluating the iridocorneal angle with gonioscopy, though care is taken to prevent excess light exposure, it is impossible to complete this technique in relative darkness. Angles that may close in complete darkness may be opened with the minimal illumination and graded erroneously. OCT allows visualization of the iridocorneal angle without the use of significant visible light and thus may discern more angles with closure. The use of a gonioscopy lens and manipulation of the lids may deepen an angle due to the placement of inadvertent pressure by the observer. Due to the OCT limitations in imaging all angle structures as visualized with gonioscopy, different criteria must be used to identify closed angles which may lead to discordant results.
Despite the differences between OCT and gonioscopy in the evaluation of the iridocorneal angle, OCT is slowly finding its way into glaucoma care with the discovery of novel parameters that are independently associated with angle closure.

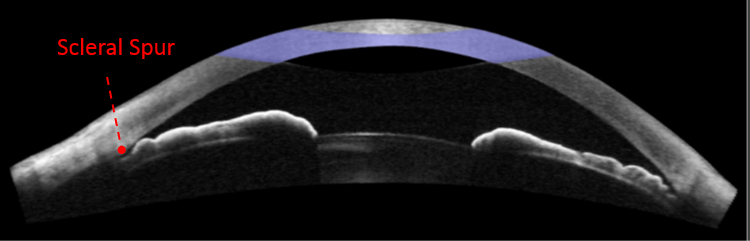
9. A closed angle with a shallow anterior chamber depth. Note the irido-corneal touch anterior to the scleral spur.

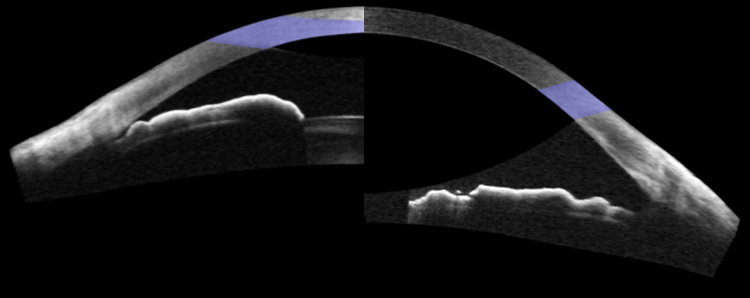
10. A composite image of the previous patient before cataract extraction (on the left side) and after cataract extraction (on the right side).
Anterior chamber width and lens vault are most readily evaluated with OCT and are not identifiable with gonioscopy. Anterior chamber width, defined as the distance between the temporal and nasal scleral spurs, has been shown to be associated with narrow angles as determined by gonioscopy. The presence of a smaller anterior chamber width increased the risk of angle closure 3.4 fold, after adjusting for age and gender.18 Lens vault, the width of the crystalline lens that is anterior to the scleral spur axis, has been shown to have a significant association with angle closure. In a study by Tan et al, patients with narrow angles had a mean lens vault of 776 μm and patients with open angles had a mean lens vault of 387 μm.19 Patients with a lens vaults greater than 668 μm were 2.2 times more likely to have angle closure than those with a lens vault less than 463 μm.19
Glaucoma is the leading cause of irreversible blindness in the world.
Researchers have estimated that close to 80 million people will be afflicted with glaucoma by the year 2020. As our understanding of the disease grows, we are no longer just trying to keep patients from going blind but are trying to detect and treat glaucoma before any visual loss occurs. OCT has allowed us to intervene in the disease process before any functional loss has occurred and revolutionized the way we think about glaucoma. The Zeiss Cirrus and other OCT for glaucoma management systems have been a cornerstone of glaucoma management for over a decade and continue to improve everyday, elevating the level of care that eye care practitioners provide to their patients.
Sources:
- Chang, Robert T., et al. “Sensitivity and specificity of time-domain versus spectral-domain optical coherence tomography in diagnosing early to moderate glaucoma.” Ophthalmology 116.12 (2009): 2294-2299.
- Wong, Elizabeth, et al. “Cirrus HD-OCT short-term repeatability of clinical retinal nerve fiber layer measurements.” Optometry & Vision Science 92.1 (2015): 83-88.
- Leung, Christopher KS, et al. “Retinal nerve fiber layer imaging with spectral-domain optical coherence tomography: analysis of the retinal nerve fiber layer map for glaucoma detection.” Ophthalmology 117.9 (2010): 1684-1691.
- Leung, Christopher KS, et al. “Retinal nerve fiber layer imaging with spectral-domain optical coherence tomography: pattern of RNFL defects in glaucoma.” Ophthalmology 117.12 (2010): 2337-2344.
- Mwanza, Jean-Claude, et al. “Residual and Dynamic Range of Retinal Nerve Fiber Layer Thickness in Glaucoma: Comparison of Three OCT PlatformsRNFL Residual and Dynamic Range in Glaucoma.” Investigative ophthalmology & visual science 56.11 (2015): 6344-6351.
- Drance, Stephen M. “The early field defects in glaucoma.” Investigative Ophthalmology & Visual Science 8.1 (1969): 84-91.
- Langerhorst, C. T., et al. “Measurements for description of very early glaucomatous field defects.” Perimetry Update 1996/1997. Kugler, New York, 1997. 67-73.
- Schiefer, Ulrich, et al. “Spatial pattern of glaucomatous visual field loss obtained with regionally condensed stimulus arrangements.” Investigative ophthalmology & visual science 51.11 (2010): 5685-5689.
- Curcio, Christine A., and Kimberly A. Allen. “Topography of ganglion cells in human retina.” Journal of comparative Neurology 300.1 (1990): 5-25.
- Hood, Donald C., et al. “Glaucomatous damage of the macula.” Progress in retinal and eye research 32 (2013): 1-21.
- Bowd, Christopher, et al. “Estimating optical coherence tomography structural measurement floors to improve detection of progression in advanced glaucoma.” American journal of ophthalmology 175 (2017): 37-44.
- Shin, Joong Won, et al. “Ganglion Cell–Inner Plexiform Layer Change Detected by Optical Coherence Tomography Indicates Progression in Advanced Glaucoma.” Ophthalmology (2017).
- Chauhan, Balwantray C., and Chris A. Johnson. “Test-retest variability of frequency-doubling perimetry and conventional perimetry in glaucoma patients and normal subjects.” Investigative ophthalmology & visual science40.3 (1999): 648-656.
- Quigley, Harry A., David S. Friedman, and Steven R. Hahn. “Evaluation of practice patterns for the care of open-angle glaucoma compared with claims data: the Glaucoma Adherence and Persistency Study.” Ophthalmology114.9 (2007): 1599-1606.
- Fain, Joel M., et al. “A multicenter, retrospective chart review study comparing index therapy change rates in open-angle glaucoma or ocular hypertension patients newly treated with latanoprost or travoprost-Z monotherapy.” BMC ophthalmology 11.1 (2011): 13.
- Quigley, Harry A., and Aimee T. Broman. “The number of people with glaucoma worldwide in 2010 and 2020.” British journal of ophthalmology 90.3 (2006): 262-267.
- Nolan, Winifred P., et al. “Detection of primary angle closure using anterior segment optical coherence tomography in Asian eyes.” Ophthalmology 114.1 (2007): 33-39.
- Nongpiur, Monisha E., et al. “Novel association of smaller anterior chamber width with angle closure in Singaporeans.” Ophthalmology 117.10 (2010): 1967-1973.
- Tan, Gavin S., et al. “Determinants of lens vault and association with narrow angles in patients from Singapore.” American journal of ophthalmology 154.1 (2012): 39-46.
