Blepharoptosis—or eyelid ptosis1—is a condition that causes a drooping of the eyelid in one or both eyes. Common in adults of all ages, “tired” or low-lying eyelids might seem like merely a superficial cosmetic issue and is often treated as such. In reality, ptosis can be much more significant, resulting in impairments in the visual field for some patients. Specifically, ptosis may be a downward displacement of the upper eyelid margin and results from a variety of myogenic, involutional, neurogenic, mechanical, traumatic, and developmental causes.5 The severity of the condition depends on the degree of the lid droop, which can also increase with age. It’s estimated that 1 in 10 adults over age 50 have ptosis,2 which corresponds to roughly 13 million patients in the U.S. alone. But this isn’t just a condition that affects older adults. Ptosis affects people of all ages, and if left untreated, ptosis may eventually reduce both visual field and visual acuity.
Because of the impact of lid position, ptosis can affect the field similarly to glaucoma3 and can make activities, such as driving, reading, and fine manual work, more difficult due to blurry vision and decreased visual field. As a reference, patients with unobstructed, normal eyelids have a superior visual field of about 50 degrees, when measured with perimetry equipment. It's generally considered that a superior visual loss of 12 degrees or more can have an impact on a patient’s vision, lifestyle, and well-being.5
The measurement used to assess ptosis is the marginal reflex distance 1 (MRD 1), which is the distance between the upper lid margin and the corneal light reflex.4 For reference, the typical cornea is 12 mm, with an upper lid sitting 1-2 mm over the top. For most patients, a normal MRD 1 is 4-5mm. A lower MRD 1 may indicate a ptosis condition that could limit the patient's visual field.
A simple method for diagnosing ptosis
Evaluating patients with ptosis incorporates many of the standard components of a comprehensive eye exam. Visual acuity and binocular vision assessments can aid in indicating a possible causative systemic disease. However, for some patients with ptosis, the impact on their vision may not come up during their exam, as many have learned how to compensate for their eyelid droop by raising their eyebrows. Patients with moderate to more severe ptosis may also be used to tilting their heads back into a chin-up position or raising their eyebrows in order to increase their visual fields.
Therefore, an appropriate lid assessment during gross assessment should really answer three questions:
- Can you see the full iris?
- Are the lids symmetrical?
- Does the patient have a visible lid platform?
The answer to the last question (lid platform) helps to differentiate between dermatochalasis (a redundancy and laxity of the eyelid skin and muscle) and ptosis. It's important to remember that it's possible to have both. This assessment takes just a few moments and can provide important insight on whether ptosis might be a concern.The bottom line is that even if the ptosis is minor, it can impact a patient's functional vision and lead to appearance-related concerns.
What is acquired ptosis?
Acquired ptosis refers to ptosis that occurs unrelated to a serious underlying medical condition and usually initiated when the muscles in the eyelid stretch and weaken, causing the upper eyelid to droop. Aponeurotic ptosis is the most prevalent form of adult-acquired ptosis and begins to present in the fifth or sixth decade of life. It is typically caused by a weakness, tear, or injury in the levator aponeurosis, which is the fascia that connects the levator palpebrae superioris muscle to the thick plate of connective tissue that lies in the upper eyelid. However, it's important to remember that ptosis affects patients of all ages.
For example, acquired ptosis can also be caused when the levator muscle of the eyelid becomes overstretched due to long-term contact lens use, cataract surgery, or an underlying medical condition.. A characteristic feature of this type of ptosis is that the affected eyelid appears lower on down gaze and the upper eyelid may be thin with redundant skin.4
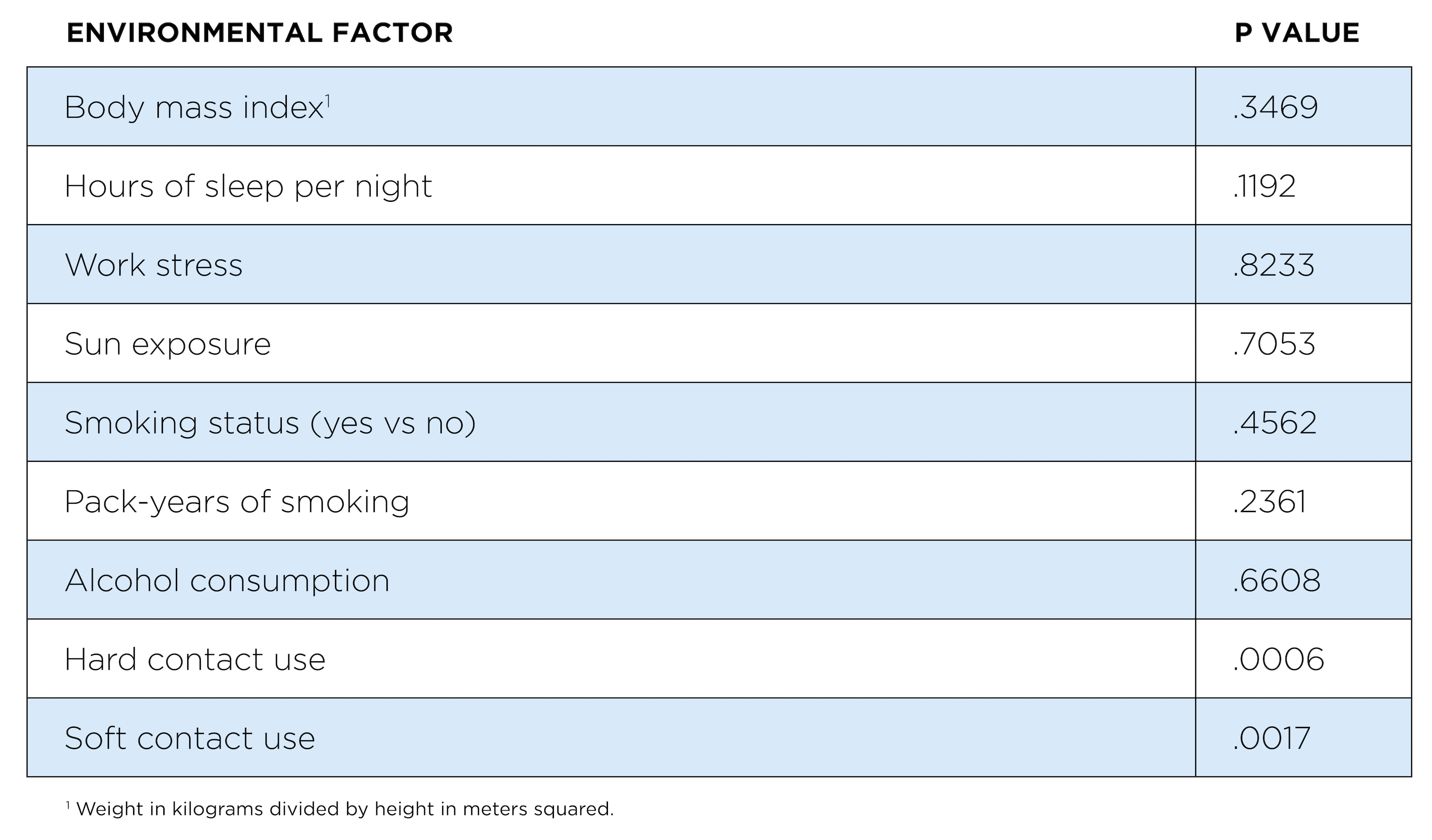
Contact lenses might be a surprising cause of ptosis, but worth mentioning to patients who wear them. In a twin study that examined the correlation of ptosis with nine different environmental factors, wearing either hard or soft contact lenses was associated with increased ptosis, with hard contact lens use more significantly associated with ptosis.5 Other factors—including body mass index, hours of sleep per night, work stress, smoking, and alcohol consumption—didn’t feature as significantly.
Table 1: Associations of ptosis with environmental factors
How is ptosis currently treated?
Up until now, surgery has been the primary prescribed treatment option and the prevalent method described in most literature to date. The rapid pace of innovation is leading to new, less-invasive alternatives to surgery, including eye drops.
As with other conditions, such as glaucoma, drops may represent a new first-line treatment option for eyecare providers, especially for patients who don’t wish to undergo surgery. While complications from ptosis surgery are rare, they may include undercorrection, poor lid crease, overcorrection, peaked lid, corneal staining, ectropion, entropion, and loss of lashes.6 A retrospective analysis of 1519 patients who underwent ptosis surgery revealed that revision was required in 8.7% of cases, with a 6.8% revision rate in patients who underwent a posterior-approach procedure and a 9.5% revision rate in those who underwent an anterior-approach procedure.7
How to measure ptosis
For those without significant experience with ptosis, it might be difficult to imagine how lid position can impact a patient’s vision so dramatically. To start, it’s helpful to know how to measure ptosis in order to determine the degree to which your patient may be affected. Proper evaluation for ptosis is essential to identify any asymmetry and can help determine the cause of the ptosis. It involves taking accurate measurements of the eyelids including:4
Margin to reflex distance (MRD)—the distance from the margin of the upper lid to the central corneal reflex (normal is 4.0-4.5mm). In general, eyelid asymmetry is confirmed when the relative difference in MRD between both eyelids is 1mm or greater.
Levator function—measures the distance of excursion of the upper eyelid margin from far downgaze to upgaze while the frontalis muscle is held still with the examiner’s hand (normal is 14mm or more).
Palpebral fissure—the distance between the upper and lower lid margin while the patient is in primary gaze (normal is 7-12mm).
Superior lid crease—the vertical distance of the superior lid margin from the natural lid crease in downgaze (normal is 8-10mm).
Vertical fissure height—The distance from the upper eyelid margin and lower margin.
The eyelid position is mainly controlled by the effects of the levator muscle complex, which is innervated by the oculomotor nerve. The Mueller muscle is responsible for about 2 mm of lid lift by providing sympathetic innervation to the lid position.8
Ptosis Exam Checklist
When examining the eyelid for ptosis, there are three easy questions to ask. These answers provide enough information to help consider whether the lid position is negatively impacting the patient in terms of both vision and psychosocial interactions.
1. Can you see the full iris?
If no, this could indicate ptosis. The typical cornea is 12mm and the upper lid sits 1-2mm over the top. Therefore a normal MRD 1* is around 4-5mm.
2. Are the lids symmetrical?
If no, this could indicate ptosis and that the levator muscle in the drooping lid is stretched or detached
3. Do you see an eyelid platform
Ptosis is an abnormal low-lying upper eyelid margin with the eye in primary gaze. Skin redundancy of the upper lid, or dermatochalasis, is a separate finding, and may occur in conjunction with ptosis.
*MRD 1 is the measurement in millimeters from the light reflex on the patient’s cornea to the level of the center of the upper-eyelid margin, with the patient gazing in the primary position.
📚
Get the ptosis exam checklist
Enter your email to download a ptosis exam guide that may make it even easier to identify eyelid ptosis in your patients.
What causes eyelid ptosis?
Eyelid ptosis occurs when there is a deficiency in the structure or function of Müller’s muscle or the levator muscle/aponeurosis complex in the posterior lamella.4 Ptosis in adults is typically referred to as involutional, aponeurotic, or acquired ptosis1 and occurs when the levator muscle stretches or separates from the eyelid. This can be a natural consequence of aging (considered to be over age 40), eye injury, or even as a side effect of surgery. Risk factors can include aging, contact lens wear, ocular surgery, trauma, underlying disease, and/or periocular neurotoxin injections. Various forms of ptosis can include:
- Neurogenic ptosis—occurs when there is reduced nervous system input to the upper eyelid retractor muscles
- Traumatic ptosis—caused by injury
- Mechanical ptosis—caused by excess skin or eyelid heaviness
- Myogenic ptosis—caused by primary muscle dysfunction
How to assess if blepharoptosis is a symptom of a serious condition
Ptosis can sometimes be a sign of an underlying neurological condition such as:
Horner’s syndrome—A combination of signs and symptoms caused by the disruption of a nerve pathway from the brain to the face and eye on one side of the body. It’s usually a result of another medical problem, such as a stroke, tumor, or spinal cord injury. Symptoms can include mild ptosis with ipsilateral pupil construction, eye redness, and anhidrosis (inability to sweat).
Myasthenia gravis—A chronic autoimmune disorder in which antibodies destroy the communication between nerves and muscle, resulting in a weakness of the skeletal muscles. The condition can present as unilateral or bilateral ptosis with upper eyelid position variability, often accompanied by diplopia (double vision) and/or strabismus (crossed eyes).
Chronic progressive external ophthalmoplegia—A condition characterized by weakness of the eye muscles. The condition typically appears in adults between the ages of 18 and 40 and may first present as symmetric, bilateral ptosis and ophthalmoparesis (an inability to move the globe into one or more fields of gaze and/or ocular misalignment).
Oculomotor nerve (CN III) palsy—When the cranial nerve III becomes paralyzed, it can cause ptosis associated with ophthalmoplegia (paralysis of the extraocular muscles that control the movements of the eye), diplopia (double-vision), and poorly-reactive dilated pupils. This condition can be present at birth or may be a result of ischemic injury or aneurysm.
Pseudoptosis—This condition may look like ptosis but may actually be dermatochalasis, or redundant eyelid skin that droops beyond the eyelid margin, creating the appearance of ptosis. Pseudoptosis can also be caused by brow ptosis, superior sulcus deformity, microphthalmos, hemifacial spasm. It can also be associated with thyroid disease.
Symptoms to watch for that may indicate further investigation include:
- Recent onset
- Acute presentation
- Unilateral ptosis
- Binocular diplopia (double vision)
- Asymmetry or aberrant pupil function
- Reduced levator function on either side
How ptosis affects vision
Even cases of mild ptosis can impact vision because the eye is such a delicate and sensitive organ. Besides drooping, patients with ptosis may complain about their tired appearance, blurry vision, and increased tearing.9 Additionally, it’s been shown that visual field deficit, rather than reduced acuity, contrast sensitivity, or stereoacuity, is a risk factor for incident falls. For each 10% loss in visual field, individuals experienced an 8% greater odds of falling after adjustment for other factors.10
Subjective visual quality is currently the major and common clinical criteria to assess the preoperative visual function of a ptotic eye and determine if an intervention is necessary. However, because subjective responses from patients can be inaccurate, a recent study set out to evaluate the objective visual quality of the ptosis eye compared to a normal eye.11 A matched case-control study was performed in 17 pairs of eyes in 17 unilateral congenital ptosis patients and found that when compared to normal eyes, the ptosis eyes showed significantly degraded optical quality.9
The study also found that the eyelid position was responsible for significant differences in both the vertical fissure heights (VFH) between the two groups (this measures the distance between the upper and lower lids) and in the best corrected visual acuities (BCVAs).9
In terms of reduction of the visual field, early ptosis studies established that superior visual field impairment is proportional to the extent of simulated ptosis.12 In the 2011 Report by the American Academy of Ophthalmology, researchers evaluated the functional indications for blepharoplasty and ptosis repair by assessing functional preoperative impairment and surgical outcomes.5 The authors completed a systematic review of earlier reported data and determined that the margin reflex distance (MRD 1) from the upper eyelid margin to the central corneal light reflex was the most predictive of field loss, which can occur when the MRD 1 is less than 4mm. When the MRD 1 is <2mm the superior field can be impaired by about 24-30%—which corresponds to 12-15 degrees of visual field loss. From their analysis of previous studies, the authors found that patients with a preoperative MRD 1 of <2mm measured in primary gaze were found to be functionally impacted in these qualitative findings:
- Self-reported functional impairment from upper eyelid droop in tasks like reading, find manual work, and watching TV
- Chin-up backward head tilt induced by visual field impairment caused by lids
- Interference with occupational duties and safety resulting from visual field impairment caused by the upper lids
- Symptoms of discomfort, eye strain, or visual interference due to the upper eyelid position5
What is the impact of acquired ptosis on cataract patients?
For cataract patients who are recommended to undergo surgery to replace their cloudy lens with an intraocular lens (IOL), the amount of light coming into the eye makes a difference in the success or failure of the cataract repair. In a 2015 case study,11 a patient with significant eyelid ptosis was complaining of ghosting or shadowing after a bilateral, sequential cataract extraction with toric intraocular lens implantation.13 The complaints arose a few weeks after cataract surgery, and by the second postoperative month, the patient’s keratometry had changed compared to preoperative measurements. The patient then underwent ptosis surgery, and four months later was found to have less corneal astigmatism than had been measured prior to cataract surgery.
In terms of planning for cataract surgery, it can be beneficial to evaluate ptosis before the cataract surgery. In some instances however, the cataract surgery can cause ptosis to occur. The incidence of ptosis after cataract surgery has been reported to be between 5% and 20%.14
In some cases, the choice of anesthesia can determine whether the levator muscle is exposed to the risk of developing ptosis. Topical anesthesia eliminates some problems with local anesthesia, including hematoma and edema of the eyelid as well as myotoxic effects of the levator. It was also determined that surgical technique can also determine exposure to risk factors for postoperative ptosis. An efficient surgeon can limit surgical time and subsequent eyelid complications that could lead to ptosis. Crum also dissuades use of bridle sutures or a rigid speculum, to limit the risk of ptosis.
Ptosis can decrease quality of life
In 2011, a report by the American Academy of Ophthalmology evaluated the functional indications and outcomes for blepharoplasty and ptosis repair by assessing functional preoperative impairment and surgical results in previously published studies.5 After evaluating 13 studies that included the effects and treatment results of simulated ptosis, conjunctiva-Muller’s muscle resection, frontalis suspension, external levator resection, and upper eyelid blepharoplasty, the report established that ptosis impaired patients’ well-being in addition to their visual fields.16 The report also emphasized that these effects increased with more severe upper eyelid malposition and indicated that intervention provides functionally significant improvements. Additionally, their report backed up earlier quality-of-life studies in large populations that substantiated the significant association between visual field impairment and difficulty with driving activities, subjective distance vision, and peripheral vision,5 as well a sense of dependency and decreased mental health.
Because ptosis affects the physical appearance of the eyes so dramatically, the condition also may impact the psychological state of patients. In a 2001 study, 210 individuals were asked to rate whole-face photos of a series of patients on the basis of 11 different personal characteristics including, intelligence, threat, friendliness, health, trustworthiness, hard work, mental illness, financial success, attractiveness, alcoholism, and happiness.17 Preoperative and postoperative photographs of male and female patients with bilateral ptosis and/or dermatochalasis (redundant eyelid skin that droops beyond the eyelid margin) were used. On all 11 characteristics in the study, the preoperative photos were rated more negatively than the postoperative images, showing that not only does ptosis affect a patient’s lifestyle—it also affects how a ptosis patient may be perceived by others.
Impact of acquired ptosis on physical appearance and emotional state
In addition to loss of visual field, visual quality, and visual function, patients with more severe forms of ptosis have also reported higher levels of anxiety, depression, and concern about their appearance compared to normal populations with scores comparable to previous research about disfiguring eye conditions.18 In a UK study conducted at Bristol Eye Hospital, the majority of ptosis patients were listed for surgery on the basis of visual symptoms and professional assessments— not solely because of concerns regarding their appearance. These ptosis patients reported appearance-related distress and dysfunction because of their ptosis, with mean scores higher than the population and 48.9% of female patients experiencing elevated levels of distress. These scores confirm the theory that ptosis has a similar emotional consequence as those with strabismus and other appearance-altering eye conditions.13 In all, 72% of female ptosis patients and 68% of male patients reported high levels of concern about their conditions.13
How to talk to patients about ptosis
Once an eyecare practitioner ascertains that the lid margin is within 2mm or less from the superior pupil margin (MRD 1 of < 3mm), then it’s important to inform the patient about the impact their ptosis can have on their vision. This is the ideal time to initiate a frank discussion about how ptosis can reduce a patient’s visual field and cause negative consequences, such as falls, accidents while driving, deterioration of occupational duties, backward head tilt, eye strain, discomfort, and other limitations.
Due to the trust patients place in eyecare practitioners, this conversation may naturally lead to other concerns, including how ptosis may impact their daily activities, lifestyle, confidence, and wellbeing. If aesthetics are an issue, then it can be helpful to remind patients that ideal beauty is often measured in millimeters, and that many patients choose to correct minor ptosis for aesthetic reasons.
In terms of correction, it can give patients great comfort to learn that surgery is no longer the de facto solution and that other pharmacological options can be considered. Often, the relief of knowing that other possibilities exist to help address ptosis inspires patients to discuss the impact of their ptosis and what potential choices may be right for them.
References
- For the purpose of this Ultimate Guide, “ptosis” refers to “acquired ptosis.”
- Sridharan GV, Tallis RC, Leatherbarrow B, et al. A community survey of ptosis of the eyelid and pupil size of elderly people. Age and Ageing. 1995;24:21–4.
- Black AA, Wood JM, Lovie-Kitchin JE, et al. Visual field loss and falls among older adults with glaucoma. Invest Ophthalmol Vis Sci 2008;49:E-Abstract 5458.
- Koka K, Patel BC. Ptosis Correction. 2021 Nov 2. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 30969650.
- Satariano N, Brown MS, Zwiebel S, et al. Environmental factors that contribute to upper eyelid ptosis: a study of identical twins. Aesthet Surg J. 2015;35(3):235-241.
- Iliff CE, Complications of Ptosis Surgery. Journal of Pediatric Ophthalmology & Strabismus. 1982 Sept.;19(5):256.
- Bacharach J, Lee WW, Harrison AR, et al. A review of acquired blepharoptosis: prevalence, diagnosis, and current treatment options. Eye (Lond). 2021;35(9):2468-2481.
- Christopher I. Zoumalan, MD, Richard D. Lisman, MD, Evaluation and Management of Unilateral Ptosis and Avoiding Contralateral Ptosis, Aesthetic Surgery Journal, Volume 30, Issue 3, May/June 2010, Pages 320–328.
- Finsterer J. Ptosis: causes, presentation, and management. Aesthetic Plast Surg. 2003 May-Jun;27(3):193-204.
- Freeman EE, Muñoz B, Rubin G, et al. Visual field loss increases the risk of falls in older adults: the Salisbury eye evaluation. Invest Ophthalmol Vis Sci. 2007.
- Shen J, Cui H, Tang X, et al. "Optical Quality Assessment in Patients with Unilateral Congenital Ptosis: A Matched Case-Control Study", Journal of Ophthalmology, vol. 2020, Article ID 2653250, 9 pages, 2020.
- Meyer DR, Linberg JV, Powell SR, et al. Quantitating the superior visual field loss associated with ptosis. Arch Ophthalmol. 1989;107:840–3.
- Kuo IC. The effect of ptosis on cataract surgical planning. Case Rep Ophthalmol. 2015 Apr 14;6(1):132-8.
- Koh V, Tatsios J, Chew PT, Amrith S. Comparison of incidence of ptosis after combined phacotrabeculectomy with mitomycin C and phacoemulsification. Indian J Ophthalmol. 2015 Dec;63(12):895-8.
- Crum, Alison V and Bernardino, Robert. (2010). Preventing and managing post-surgery ptosis. Review of Ophthalmology. https://www.reviewofophthalmology.com/article/preventing-managing-post-surgical-ptosis.