




Diabetes is a growing public health issue and is the first non-infectious disease to be labeled an epidemic by the World Health Organization.1 Despite continued improvements in the care of diabetes mellitus, diabetic retinopathy (DR) and diabetic macular edema (DME) remain major causes of vision loss in patients with diabetes.2
In the last two decades, treatment paradigms have dramatically evolved for diabetic eye disease with the widespread use of vascular endothelial growth factor (VEGF) inhibitors and sustained released corticosteroids. Several clinical trials have demonstrated the use of both VEGF inhibitors and corticosteroids in the successful management of diabetic eye disease.
Here we present the role of corticosteroids in suppressing chronic inflammation and tissue injury specific to DME in the diabetic patient population.
Pathophysiology of diabetic macular edema
Historically, DME has been considered a purely microvascular complication of diabetic retinopathy, involving vascular injury such as endothelial cell damage, pericyte loss, and secondary breakdown of the inner blood–retinal barrier (BRB). However, as knowledge surrounding the pathophysiology of DME has advanced, other cellular processes have been identified that directly contribute to the pathogenesis of DME including chronic neuroinflammation, neurodegeneration, and microvascular insufficiency.3 In fact, neurodegeneration and neuroinflammation have been shown to precede the earliest manifestation of vasculopathy in diabetic retinopathy and considered central to disease progression.4

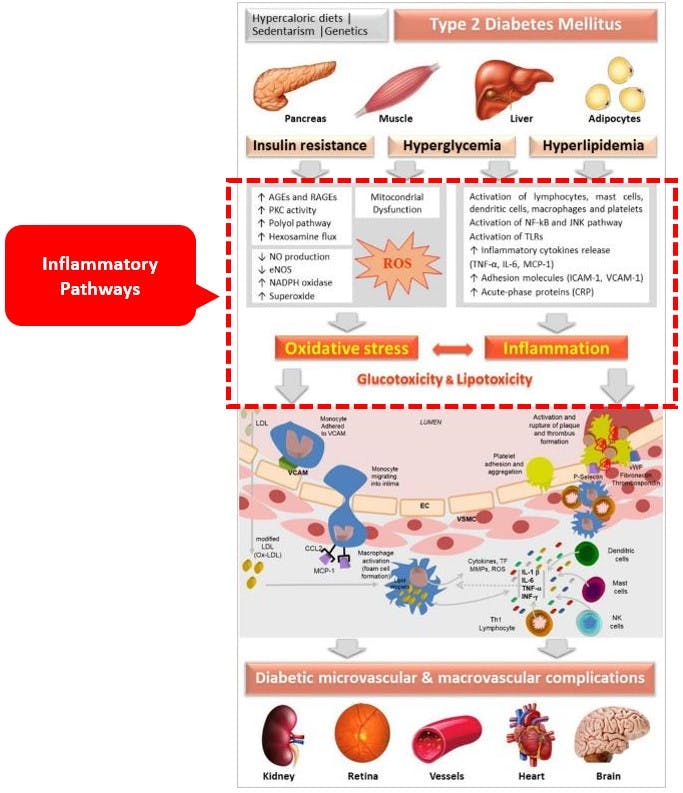
Figure 1: Pathophysiology of DME
Hyperglycemia, the main driving force in diabetic eye disease, leads to an array of metabolic and functional derangements in retinal vascular and neuronal cells including chronic inflammation and overproduction of reactive oxygen species (ROS).3 Precipitated by hyperglycemia, the prominent source of inflammatory cytokines lies in the Müller glial cells, spanning the entire width of the retina and are in intimate contact with the retinal vasculature as well as responsible to maintain the integrity of the BRB.5

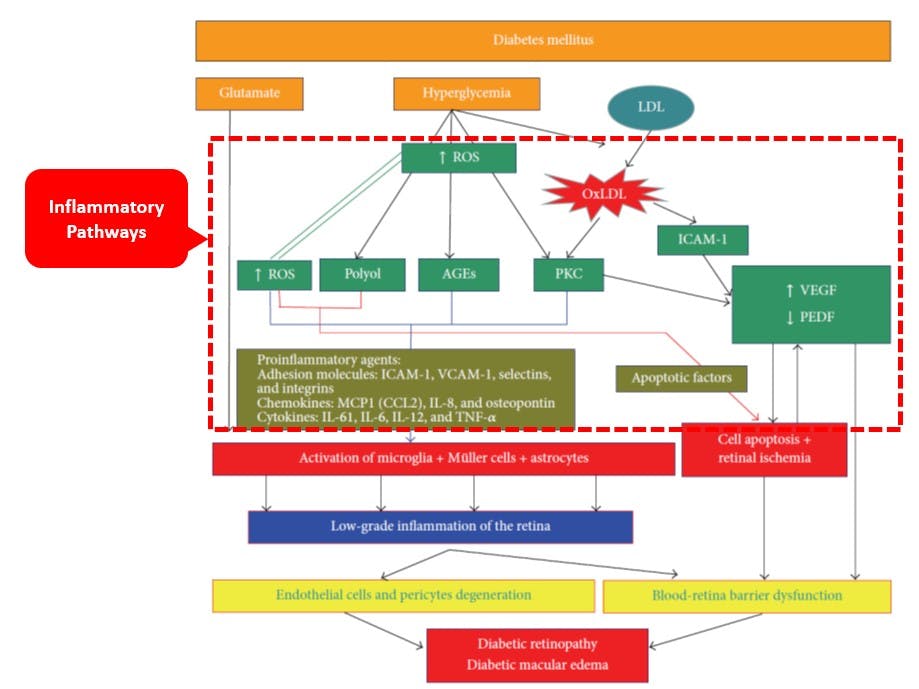
Figure 2: Cytokines
Ultimately, various cytokines, including VEGF, are involved in the pathophysiology of DME and diabetic eye disease. Eyes with DME exhibit intraocular upregulation of a myriad of unique cytokines and growth factors such as: interleukin-6, interleukin-8, interleukin-1β, monocyte chemotactic protein-1, tumor necrosis factor α, and VEGF.6 In DME, the chronic low-grade inflammatory state caused by pathological hyperglycemia amplifies this inflammatory cytokine release.

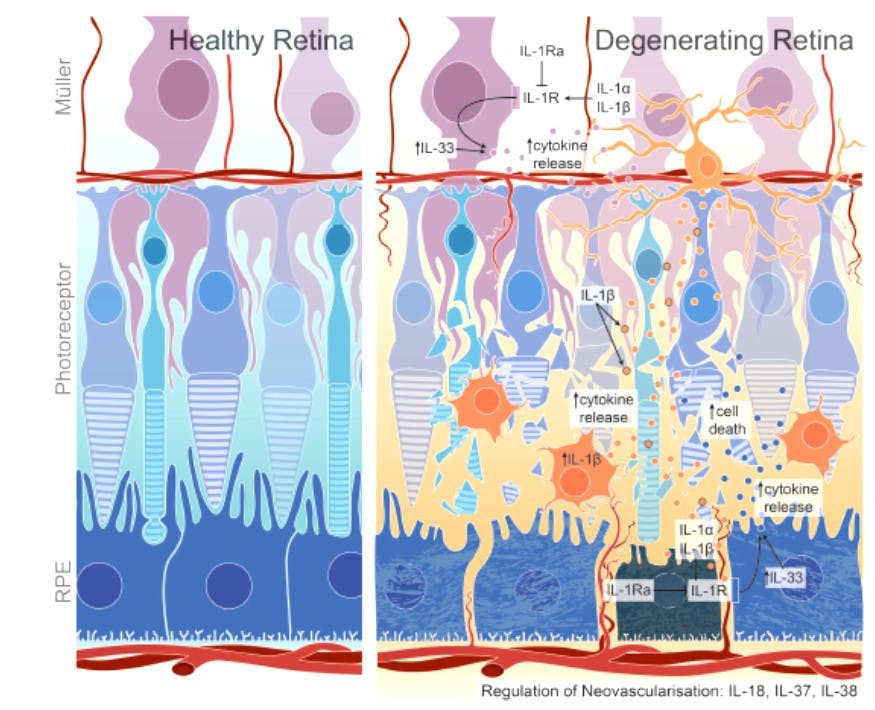
Figure 3: Retina adapted from Wooff et al. Frontiers Immunology 2019
Inflammatory cytokines recruit and activate immune cells causing direct downregulation of endothelial tight junctions, upregulation of ROS, and further production of cytokines such as VEGF; consequently, retinal pericyte death, endothelial cell damage, thickening of the capillary basement membrane, and deposition of extracellular matrix components occur.7 Breakdown of the blood-retinal barrier then ensues causing extracellular fluid to accumulate in the macula causing DME.8 Additionally, persistent inflammatory cytokine release also upregulates retinal cell death signaling, leading to neurodegeneration and thinning of the peripapillary retinal nerve fiber layer over time.9
The role of corticosteroids in DME and diabetic eye disease
Targeting many of the aforementioned immune-mediated processes, corticosteroids have demonstrated efficacy by means of wide spectrum anti-inflammatory effects including anti-apoptotic, anti-angiogenic, and neuroprotective effects.11 Three synthetic corticosteroids—triamcinolone acetonide, dexamethasone phosphate, fluocinolone acetonide—are currently used for the treatment of DME. The preferred method of administration is intravitreal injection as systemic corticosteroids are associated with the risk of hyperglycemia—the main precipitant of inflammation in DME, as well as several additional undesirable side effects. Corticosteroids exhibit a long duration of action and help minimize treatment burden in the management of DME.12 Common adverse events include cataract formation and progression and elevation of intraocular pressure.13-15
The anti-inflammatory effect of glucocorticoids is mediated by several molecular pathways, including direct and indirect gene expression and second-messenger cascades. These processes help stabilize and reconstitute the BRB, cause capillary constriction, and downregulate inflammatory and angiogenic cytokine expression.16 Corticosteroid mechanism of action is best targeted for DME and these agents have been shown to preserve visual function with long-term visual acuity improvement in eyes with DME.17,18
Whereas VEGF inhibitors are routinely used for the management of DME and DR, anti-VEGF therapy monotherapy can be limited in treating the underlying chronic inflammation found in diabetic eye disease.
Multi-modality treatment paradigms (i.e., intravitreal VEGF inhibitors, intravitreal corticosteroids, laser photocoagulation, vitreoretinal surgery) may offer patients the best approach to the management of the varying spectrum of morbidity in diabetic eye disease. Whether considering patients with chronic, recalcitrant, or severe DME, as well as attempting to minimize treatment burden, optimal corticosteroid use ultimately needs to be tailored to each individual patient for the best possible outcomes.
Conclusions
In summary, chronic inflammation plays a critical role in DME and diabetic eye disease and is a fundamental therapeutic target in preventing irreversible vision loss. Multi-modality therapy of corticosteroids, in conjunction with VEGF inhibitors, provides a flexible management approach for addressing diabetic retinal pathology. As the treatment landscape for diabetic eye disease continues to evolve, we hope for elucidation of further tenets to mitigate disease progression and address the growing burden of diabetic eye disease.
References
- World Health Organization 2018: Diabetes, Who.int/newsroom/fact-sheets/detail/diabetes
- Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis (Lond). 2015;2:17. Published 2015 Sep 30. doi:10.1186/s40662-015-0026-2
- Haritoglou C, Maier M, Neubauer AS, Augustin AJ. Current concepts of pharmacotherapy of diabetic macular edema. Expert opinion on pharmacotherapy. 2020 Mar 3;21(4):467-75.
- Midena and Bino: Multimodal retinal imaging of diabetic macular edema: toward new paradigms of pathophysiology. Graefes Arch Clin Exp Ophthalmol 2016
- Abcouwer SF. Müller Cell–Microglia Cross Talk Drives Neuroinflammation in Diabetic Retinopathy. Diabetes. 2017 Feb 1;66(2):261-3.
- Sohn HJ, Han DH, Kim IT, Oh IK, Kim KH, Lee DY, Nam DH. Changes in aqueous concentrations of various cytokines after intravitreal triamcinolone versus bevacizumab for diabetic macular edema. American journal of ophthalmology. 2011 Oct 1;152(4):686-94.
- Boss JD, Singh PK, Pandya HK, Tosi J, Kim C, Tewari A, Juzych MS, Abrams GW, Kumar A. Assessment of neurotrophins and inflammatory mediators in vitreous of patients with diabetic retinopathy. Investigative ophthalmology & visual science. 2017 Oct 1;58(12):5594-603.
- Duh EJ, Sun JK, Stitt AW. Diabetic retinopathy: current understanding, mechanisms, and treatment strategies. JCI insight. 2017 Jul 20;2(14).
- Barber AJ, Baccouche B. Neurodegeneration in diabetic retinopathy: potential for novel therapies. Vision research. 2017 Oct 1;139:82-92.
- Petrachkov DV, Budzinskaya MV, Pavlov VG, Durzhinskaya MH, Khalatyan AS. Neurodegenerative biomarkers of the response to diabetic macular edema treatment. Vestnik Oftalmologii. 2020 Jan 1;136(4. Vyp. 2):201-6.
- Schwartz SG, Scott IU, Stewart MW, Flynn HW Jr. Update on corticosteroids for diabetic macular edema. Clin Ophthalmol. 2016;10:1723-1730. Published 2016 Sep 8. doi:10.2147/OPTH.S115546
- Whitcup SM, Cidlowski JA, Csaky KG, Ambati J. Pharmacology of Corticosteroids for Diabetic Macular Edema. Invest Ophthalmol Vis Sci. 2018;59(1):1-12. doi:10.1167/iovs.17-22259
- Chu YK, Chung EJ, Kwon OW, Lee JH, Koh HJ. Objective evaluation of cataract progression associated with a high dose intravitreal triamcinolone injection. Eye (Lond). 2008 Jul;22(7):895-9. doi: 10.1038/sj.eye.6702802. Epub 2007 Apr 13. PMID: 17435692.
- Agrawal S, Agrawal J, Agrawal TP. Management of intractable glaucoma following intravitreal triamcinolone acetonide. Am J Ophthalmol. 2005 Mar;139(3):575-6; author reply 576. doi: 10.1016/j.ajo.2004.10.025. PMID: 15767088.
- Moshfeghi DM, Kaiser PK, Scott IU, Sears JE, Benz M, Sinesterra JP, Kaiser RS, Bakri SJ, Maturi RK, Belmont J, Beer PM, Murray TG, Quiroz-Mercado H, Mieler WF. Acute endophthalmitis following intravitreal triamcinolone acetonide injection. Am J Ophthalmol. 2003 Nov;136(5):791-6. doi: 10.1016/s0002-9394(03)00483-5. PMID: 14597028.
- Zhang X, Wang N, Schachat AP, Bao S, Gillies MC. Glucocorticoids: structure, signaling and molecular mechanisms in the treatment of diabetic retinopathy and diabetic macular edema. Curr Mol Med. 2014;14(3):376–384.
- Martidis A, Duker JS, Greenberg PB, et al. Intravitreal triamcinolone acetonide for refractory diabetic macular edema. Ophthalmology. 2002;109(5):920–927
- Sohn HJ, Han DH, Kim IT, Oh IK, Kim KH, Lee DY, Nam DH. Changes in aqueous concentrations of various cytokines after intravitreal triamcinolone versus bevacizumab for diabetic macular edema. American journal of ophthalmology. 2011 Oct 1;152(4):686-94.
- Puliafito CA, Cousins SW, Bacharach J, Gonzalez VH, Holekamp NM, Merrill PT, Ohr MP, Parrish RK 2nd, Riemann CD. Forming a Consensus: Data and Guidance for Physicians Treating Diabetic Macular Edema. Ophthalmic Surg Lasers Imaging Retina. 2016 Apr;47(4 Suppl):S4-S15. doi: 10.3928/23258160-20160224-01. PMID: 27096289.

