At a 2020 meeting of glaucoma specialists and cataract surgeons, Nathan Radcliffe, MD, found it surprising that not everyone in attendance saw as much value in canaloplasty as he did.
Therefore, in the episode of Interventional Mindset, he wanted to garner the expertise of I. Paul Singh, MD, who has a wealth of experience with
microinvasive glaucoma surgeries (MIGS) and can speak to the efficacy of using canaloplasty and viscodilation in conjunction with other procedures.
Interventional Mindset is an educational series that gives eye physicians the needed knowledge, edge, and confidence in mastering new technology to grow their practices and provide the highest level of patient care. Our focus is to reduce frustrations associated with adopting new technology by building confidence in your skills to drive transformation.
Browse through our videos on a variety of topics within cataract and refractive surgery, glaucoma, and ocular surface disease to learn practical insights into adopting a variety of new surgical techniques and technology.
Overview of canaloplasty
As a relatively new surgery, canaloplasty uses a microcatheter to open Schlemm’s canal through a 360º cannulation, thus promoting aqueous outflow pathways by targeting the areas of insult, including the collapse of Schlemm’s canal and collector channels, atrophy of the collector channels, and pathology of the trabecular meshwork (TM).
The non-penetrating technique is indicated mostly for patients who have been diagnosed with primary open-angle glaucoma (POAG). Both doctors feel there is compelling evidence to use the canal as a target in a number of surgical scenarios.
Where is the resistance?
When considering the best option to improve outflow, whether using TM bypass, canal dilation, cutting, stripping, or
canaloplasty, the first question to ask is, “Where exactly is the resistance?”
It is important to take into account that in many POAG patients, the TM is not always the main site of resistance and that, oftentimes, the canal is not evenly distributed from an anatomical perspective.
One study, represented in Figure 1 below, demonstrated that, when compared to normal eyes, significantly more POAG patients (up to 50%) had canal herniations with a complete collapse blocking the collector channel ostea.1-4 Therefore, performing a TM bypass only may result in missing the main point of resistance.
Glaucoma and resistance staging
In addition to disease
staging glaucoma in the traditional “mild, moderate, severe” ranking, Dr. Singh suggests also incorporating resistance staging. For example, when considering a pre-perimetric glaucoma patient with no visual field loss but an intraocular pressure (IOP) of 24mmHg and a daily regimen of four medications, Dr. Singh would dually stage this individual as early glaucoma with high resistance, most likely located beyond the TM.
Dr. Radcliffe describes it as a “matter of duration,” as resistance that originates in the TM may then migrate distally into the canal, which is a “use it or lose it” tissue. He suggests that an inactive collector channel shrinks, decreasing outflow even further and could increase disease severity. Herniation is a step beyond canal collapse, with the trabecular tissue becoming wedged, requiring reversal with surgical intervention.
The HydrOMNI procedure
When Dr. Singh assesses a patient with mild to moderate glaucoma who has been on multiple medications for an extended time and for whom selective laser trabeculoplasty (SLT) was not successful, his assumption is that there is resistance due to collapse in the canal. To fully address resistance, the next logical step is to target the entire conventional outflow pathway.
Therefore, the best way to proceed is to combine procedures, such as a
Hydrus Microstent (Alcon) and the
OMNI Surgical System (Sight Sciences) for canaloplasty to initially flush out the canal and then apply scaffolding to maintain outflow. He refers to this as the “HydrOMNI” procedure.
Combining the mechanisms of
viscodilation and cutting, OMNI enables surgeons to open the Schlemm’s canal, break up any offending herniations, and then flush out the outflow system using an ophthalmic viscoelastic device (OVD).
Surgical pearls for performing the HydrOMNI procedure
To illustrate this point, Dr. Singh shares a surgical video that demonstrates catheter canaloplasty with the iTrack catheter, which can facilitate a significant expansion of the canal and thinning of the TM after viscodilation. Anecdotally, this process goes beyond just breaking up herniations with the catheter.
Surgical pearl: During the procedure, Dr. Singh prefers to aim toward the TM at a 45° angle and use consistent pressure.
As further proof, Dr. Radcliffe showed a picture of a prior patient 2 years post-surgery, which affirmed how canaloplasty under the temporal wound with VISCO360 (Sight Sciences) notably inflated Schlemm's canal 180° from the surgical site and that the results have been maintained since the procedure.
Surgical pearl: Dr. Radcliffe often performs both the excisional dragging technique and the ripping technique to achieve optimal results.
As a fan of combining mechanisms of action, Dr. Singh shares two other surgical videos demonstrating the OMNI surgical technique with otomy as well as the HydrOMNI, which entails OMNI viscodilation and goniotomy 180 along with
Hydrus implantation.
Viscodilation/cutting procedure algorithm
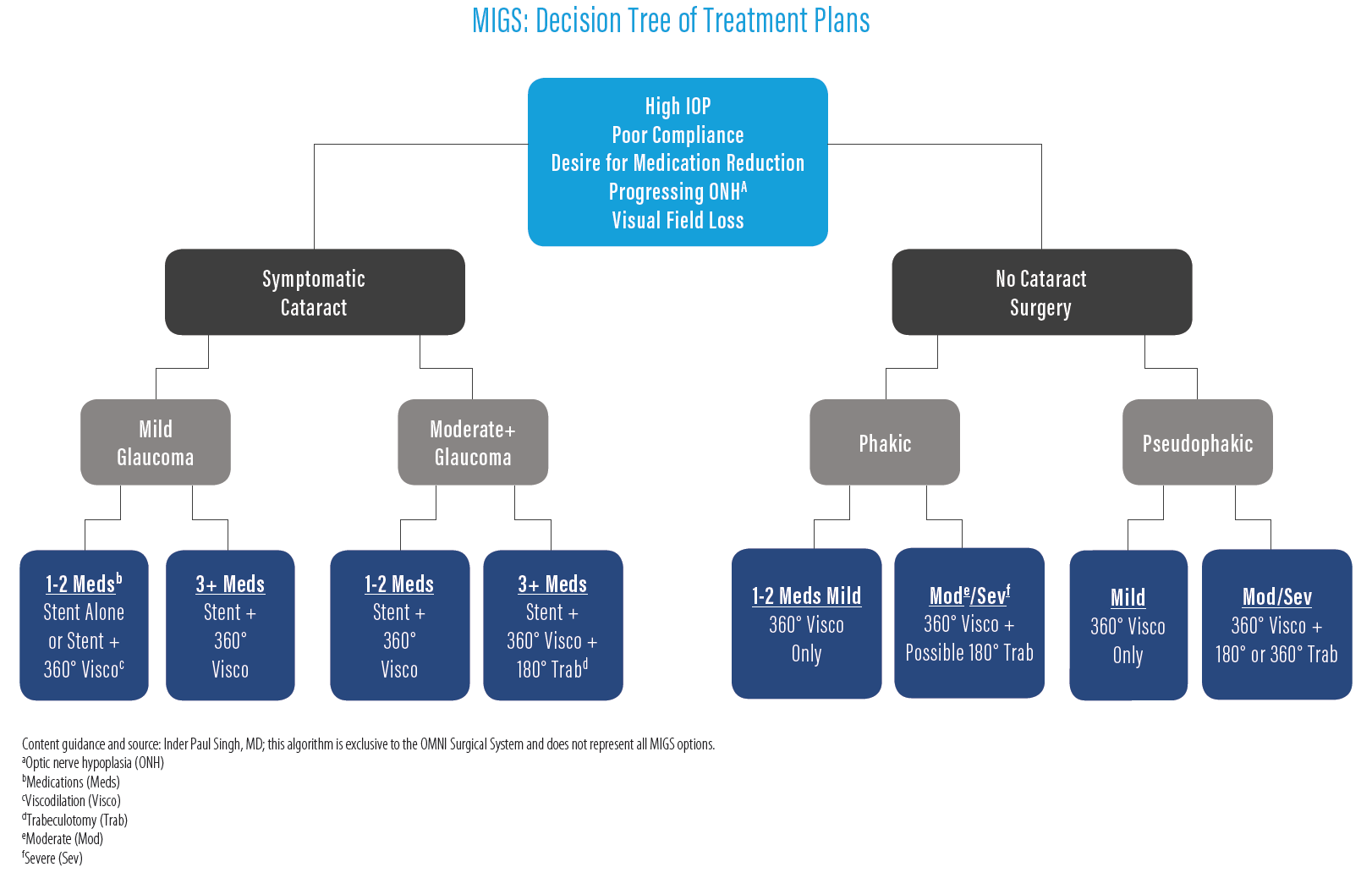
The formula used by Dr. Singh to decide on which MIGS procedure or a combination thereof to utilize begins with the level of disease state, determined by examining the visual fields and optic nerve coupled with the target IOP range.
Next, he gauges the resistance of outflow by accounting for IOP, number of medications, and past response to laser trabeculoplasty. He also considers lens status and whether the patient might already be scheduled to undergo
cataract surgery or is likely to require cataract surgery in the future.
Further, when there are minimal to no insurance hurdles, Dr. Radcliffe also prefers a combined approach and tailors treatment to the disease in a very similar fashion.
Figure 1 is a diagram that outlines the decision-making process for performing MIGS procedures.5
Figure 1: Courtesy of I. Paul Singh, MD.
In closing
Combination procedures like HydrOMNI can provide a way to balance both an effective approach to lowering IOP and a favorable safety profile with the potential added benefit of reducing the medication burden.
Having the ability to combine
MIGS procedures with different mechanisms further customizes the treatment for POAG patients, which is a key component to embracing an interventional mindset.