




WHAT YOU'LL LEARN
Review the comorbidities of diabetic retinopathy
Optimize imaging prior to vitreoretinal surgery
Identify the four steps of vitrectomy
Understand best practices for post-operative care
Introduction
Diabetic retinopathy is the leading cause of vision impairment in the middle-aged population in the United States. The treatment options range from medical management in the clinic (e.g. intravitreal injections and laser for diabetic macular edema and proliferative diabetic retinopathy), to surgical management in the operating room for vitreous hemorrhage, retinal detachment, and membranectomy. This review highlights the important variables to consider before, during, and after surgery.

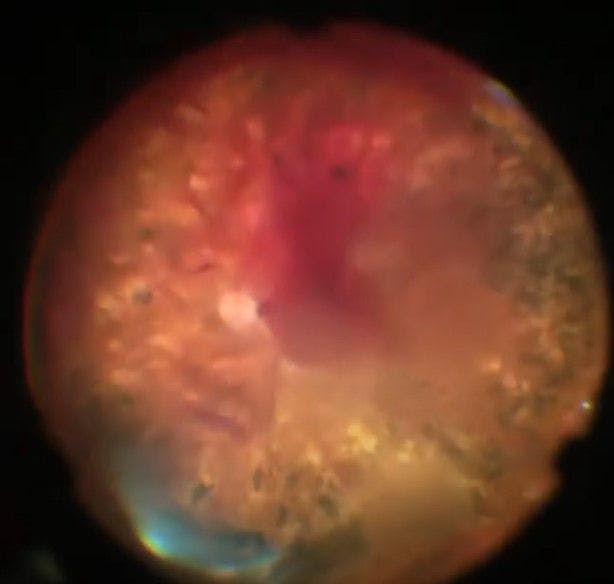
Figure 1: Diabetic vitreous hemorrhage.
Pre-operative checklist
Before surgery
The ophthalmology resident should take into consideration the patient's general systemic medical health to first better determine the patient’s risk for ocular disease, and the risks that may be encountered during surgery. Generally speaking, a patient’s diabetic control (e.g., hemoglobin A1C) and the duration of diabetes may factor in their risk stratification for ocular disease and the potential complexities encountered during surgery.
The patient’s comorbidities such as heart disease, stroke, hypertension should also be taken into consideration, as these may make a patient’s surgery more complex or complicated. As an illustrative example, a patient recently encountered had elevated troponins and an acute exacerbation of congestive heart failure. The cardiologist requested the need for vascular catheterization and workup; however, the cardiologist had no objection to proceeding with monitored anesthesia care (MAC) surgery because the patient would likely need to be on anticoagulation after their cardiac procedure.
Sometimes holding anticoagulation medicines (e.g. aspirin, plavix, warfarin, etc) prior to eye surgery can be difficult, depending on comorbidity or past cardiovascular events (e.g., myocardial infarction or stroke). Similarly, a patient with uncontrolled blood pressure may have more difficult hemostasis during surgery, especially as it relates to retinal neovascularization. A patient’s body habitus and ability to lay supine for prolonged time periods may also make surgery more difficult depending on the level of sedation they are given by the anesthesia team.
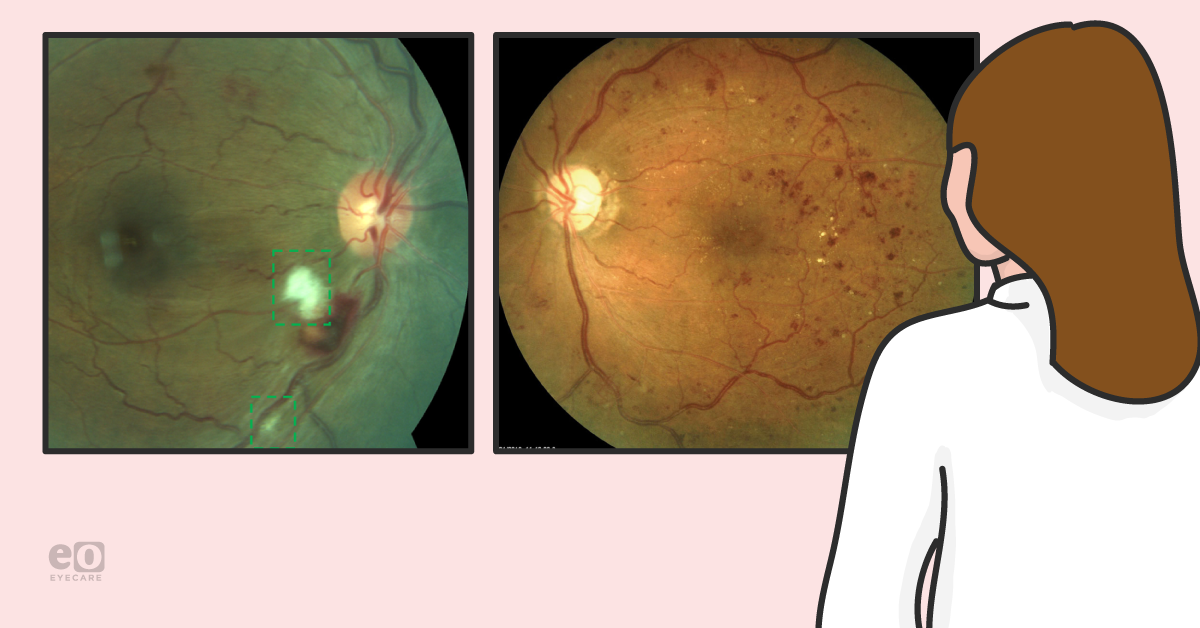
Moreover, a patient’s history of vision changes and their past treatment is an important consideration. For example, a patient who had good vision, with new onset vitreous hemorrhage one week prior, may behave very differently from a patient who has chronic light perception vision for several months or years prior. Similarly, a patient who has had several intravitreal injections or panretinal photocoagulation laser (see Figure 5), may be at lower risk for intraoperative bleeding or tractional detachment, than a patient who has never had any prior treatment to their eyes.
When honing into the eye exam, it is important to consider the clarity of the view posteriorly. Is the cornea clear? How clear or opaque is the cataract? If the patient is young, be sure to counsel the patient of cataract progression after retina surgery so that it is considered as an expectation, rather than a complication. In fact, cataract formation occurs in up to 80% of eyes after pars plana vitrectomy within two years. Sometimes, a clear lens with dense vitreous hemorrhage, is difficult to manage because blood will accumulate posterior to a clear lens making the view more challenging.
In cases where there is dense vitreous hemorrhage, especially just posterior to the native lens, it may be advantageous for the patient to undergo cataract surgery prior to retina surgery. If an intraocular lens was recently placed, is the centration and intraocular lens stable? Were there any complications during recent cataract surgery, such as a ruptured posterior capsule? Is the posterior capsule intact or hazy? Does the iris dilate well or is there neovascularization of the iris that may put the patient at risk for anterior segment bleeding intra- or post-operatively?
Imaging prior to vitreoretinal surgery should be optimized. If the vitreous hemorrhage, for example, is mild, fluorescein angiography and optical coherence tomography (OCT) imaging can often give a better idea of the macula status. The extent of the neovascularization and the health of the macula (e.g., macular edema, ischemia, epiretinal membrane) should be considered to give better counseling to the patient. Residents will do well to have a low threshold for ultrasound evaluation of diabetics in cases of difficult visualization to better determine hyaloid and vitreous separation status. This will also better determine if the periphery or posterior pole has any significant traction from neovascular membranes. Knowing this prior to surgery can empower the surgeon to better counsel the patient as to whether or not a patient may need intraocular gas or silicone oil tamponade.

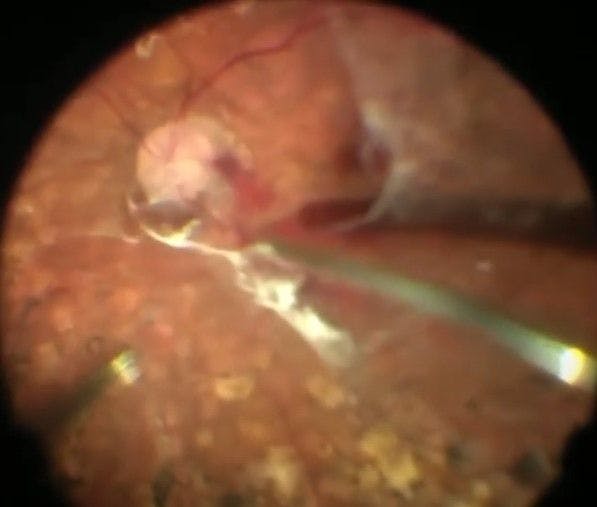
Figure 2: Removal of diabetic neovascular membranes.
Operating
During surgery
A majority of vitreoretinal surgical procedures for diabetic patients are done in the operating room, often in an ambulatory surgery center, as an outpatient. A straightforward retinal surgery can range in time; however, complicated surgeries involving extensive peeling of membranes or detachment repair can last significantly longer. A patient should expect to have a driver for transportation. An overwhelming majority of surgeries are done while awake but comfortable under MAC by a skilled anesthesia provider. Often patients ask if they will be put to sleep, and my response to them is that they will be “awake but comfortable”, “twilight”, or “like having a colonoscopy” so that they can better understand the expectations during surgery. I discuss that we will “numb” the eye via a peri- or retrobulbar anesthetic block. The patient should expect to feel minimal pain or discomfort with this local anesthesia.
After the patient is positioned appropriately, and anesthesia is administered, the surgery begins. A brief summary of a standard vitreoretinal surgical approach is summarized below:
A point is marked 4 mm posterior the inferotemporal limbus and a 25-gauge (sometimes 23-or 27-gauge) valved trocar/cannula is inserted using a beveled approach to obtain a three-plane insertion. The position and function of the infusion cannula are always confirmed prior to use to ensure that the cannula is not in the suprachoroidal or subretinal space. Similar cannulas are then placed in the superotemporal and superonasal quadrants.
The vitreous needs trimmed closely near the optic nerve and a vitreous detachment either induced or verified. A core posterior vitrectomy can then be performed with removal of all unopacified vitreous and any vitreous membranes or vitreous hemorrhage present. Sometimes a dilute 50% mixture of triamcinolone is injected into the vitreous cavity to better visualize the remaining vitreous as a chromovitrectomy technique. Any remaining vitreous is then removed with the vitreous cutter and scleral indentation.


Figure 3: Step 1 of a vitrectomy for a diabetic patient: Core vitrectomy
Critically, areas of neovascularization are segmented, dissected, peeled and removed with the vitreous cutter, and sometimes instruments like retinal forceps or a Tano membrane scraper can be used in addition. Panretinal photocoagulation is performed with an endolaser probe for 360 degrees to ensure complete treatment of the peripheral ischemic retina. Inspection is done with scleral indentation for 360 degrees to ensure there is no evidence of peripheral retinal breaks.

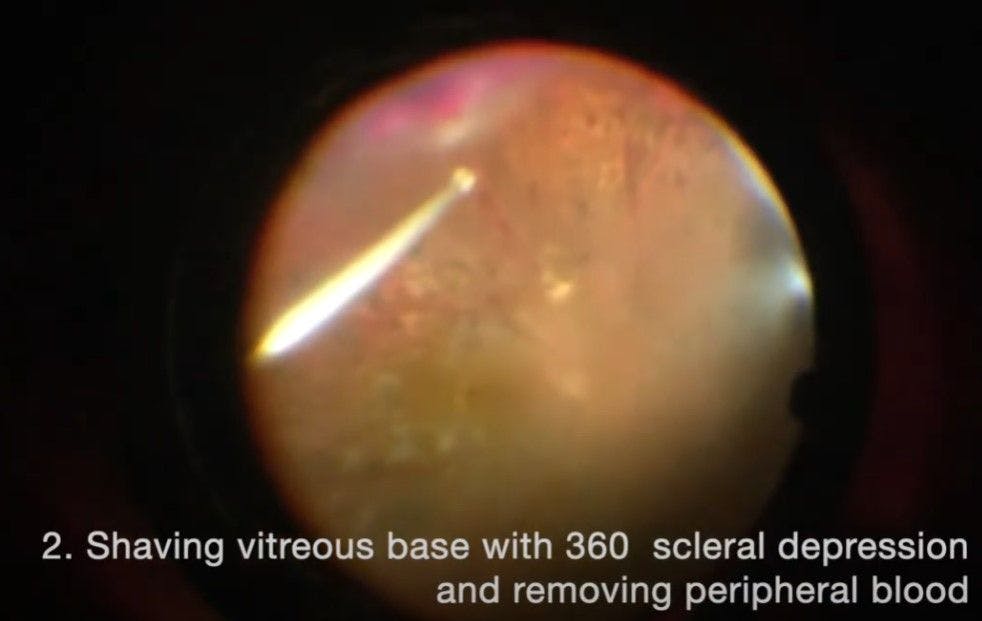
Figure 4: Step 2 of a vitrectomy for a diabetic patient: Peripheral vitrectomy


Figure 5: Step 3 of a vitrectomy for a diabetic patient: Endolaser panretinal photocoagulation
If tamponade is needed, such as in cases of tractional retinal detachment repair, a soft-tip silicone cannula is used to perform a complete air-fluid exchange. Then, approximately 45 mL of either SF6 or C3F8 gas (alternatively silicone oil) is injected via the superotemporal cannula while excess air/gas is allowed to escape via the superonasal cannula. The intraocular pressure is checked via palpation and care is made to ensure that an overfill is not present.

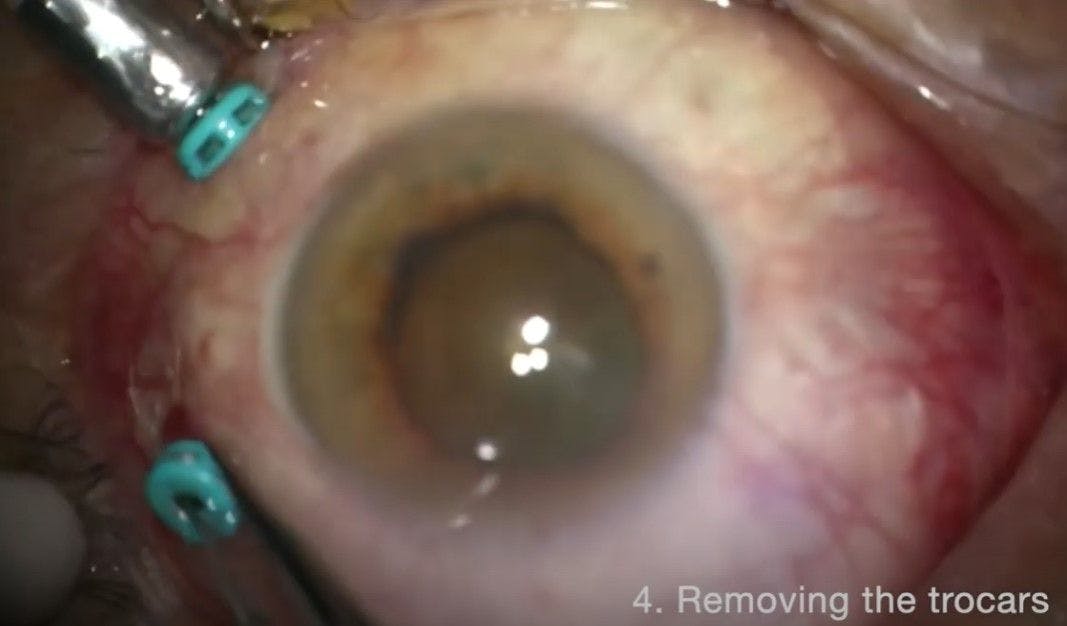
Figure 6: Step 4 of a vitrectomy for a diabetic patient: Trocar removal at conclusion of surgery
The cannulas are then removed from the superotemporal and superonasal sclerotomy sites, followed by the inferotemporal sclerotomy site. The sclerotomies are tested to ensure there are no leaks. Any leaking sclerotomy wounds are closed with 7-0 (or sometimes 8-0) Vicryl interrupted sutures. Finally, the eyelid speculum is removed and the eye is patched and a shield is applied.
Post-operative checklist
After Surgery
The patient should be expected to follow-up with their surgeon at the very least one day, one week, and one month after surgery. The purpose of these visits is to review the postoperative instructions. A blue patch is to be worn at night for the first 1-2 weeks so that the patient doesn’t inadvertently rub their eye. Typically, a topical antibiotic (e.g. ocuflox) and corticosteroid (e.g. prednisolone acetate) are started four times daily in the operative eye after their one day postoperative visit. If a tamponade agent is used (e.g. gas or oil) in the event of retinal detachment repair, positioning and restrictions related to gas are instructed. While a little bit controversial, a change in more than 2000 to 3000 feet in altitude is considered significant, and the patient should remain at lower altitudes for at least the first night after surgery if traveling to higher altitudes is necessary. Note that the location of the surgery may not necessarily be “0 feet” or sea level but is considered the reference level.
Mild residual or recurrent vitreous hemorrhage may be experienced in the early postoperative period due to oozing neovascular blood vessels that were removed or cauterized during the surgery. Sometimes the vitreous hemorrhage persists, but eventually reabsorbs since the native vitreous was removed during vitrectomy. Intravitreal injections in the postoperative period can sometimes help facilitate residual neovascular oozing from the optic nerve and diabetic macular edema. OCT imaging is advised to better follow the fluctuations in edema in the postoperative period. If the view is significantly improved, consider repeat angiography imaging to better evaluate the level of ischemia in the macula and peripheral retina.
While many patients do well postoperatively in terms of maintaining quiescence of proliferative retinal pathology after surgery, it is ultimately up to the patient to maintain good control of their diabetes, with a Hemoglobin A1c of less than 7 recommended to prevent further complications. Patients should work closely with their primary care doctor or endocrinologist to achieve improved health outcomes which in turn yield better ocular outcomes.

